A Nnual R Eport 2 0 0 1 / 2 0
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Memorandum of Understanding
MOU – Effective June 2009 (expected amendment November 2009) MEMORANDUM OF UNDERSTANDING Between MASSEY UNIVERSITY SCHOOL OF AVIATION And WINGS FLIGHT TRAINING And FOXPINE AIRPARK LTD And FLIGHT TRAINING MANAWATU And THE SQUARE TRUST RESCUE HELICOPTER And HELIPRO And AIR FREIGHT NZ LTD And AIRWORK FLIGHT OPERATIONS LTD And SUNAIR AVIATION LTD And ROYAL NEW ZEALAND AIRFORCE And AIR NELSON LTD And MT COOK AIRLINES And AIR NEW ZEALAND LTD And in conjunction with PALMERSTON NORTH AIRPORT LTD And AIRWAYS CORPORATION OF NZ LTD 1 MOU – Effective June 2009 (expected amendment November 2009) 1 PARTIES 1.1 Massey University School of Aviation is a flight training organisation located at Palmerston North Airport 1.2 Wings Flight Training is a flight training organisation also located at Palmerston North Airport. 1.3 Foxpine Airpark Ltd is an airport operator and a flight training organisation and is the owner of and operating from Foxpine Airport. 1.4 Flight Training Manawatu is a flight training organisation located at Feilding Aerodrome 1.5 The Square Trust Rescue Helicopter is located at the Palmerston North Hospital. 1.6 Helipro is a commercial helicopter operator also involved in flight training and has a base located at the Palmerston North Airport. 1.7 Air Freight NZ Ltd is a commercial operator based in Auckland and operates freight aircraft types Convair 580 / 5800 under the call sign of “Air Freight” 1.8 Airwork Flight Operations Ltd is a commercial operator based in Auckland and operates both F27 and Metro aircraft types on freight operations under the call sign of “Post”. -

1.4. Coding and Decoding of Airlines 1.4.1. Coding Of
1.4. CODING AND DECODING OF AIRLINES 1.4.1. CODING OF AIRLINES In addition to the airlines' full names in alphabetical order the list below also contains: - Column 1: the airlines' prefix numbers (Cargo) - Column 2: the airlines' 2 character designators - Column 3: the airlines' 3 letter designators A Explanation of symbols: + IATA Member & IATA Associate Member * controlled duplication # Party to the IATA Standard Interline Traffic Agreement (see section 8.1.1.) © Cargo carrier only Full name of carrier 1 2 3 40-Mile Air, Ltd. Q5 MLA AAA - Air Alps Aviation A6 LPV AB Varmlandsflyg T9 ABX Air, Inc. © 832 GB Ada Air + 121 ZY ADE Adria Airways + # 165 JP ADR Aegean Airlines S.A. + # 390 A3 AEE Aer Arann Express (Comharbairt Gaillimh Teo) 809 RE REA Aeris SH AIS Aer Lingus Limited + # 053 EI EIN Aero Airlines A.S. 350 EE Aero Asia International Ltd. + # 532 E4 Aero Benin S.A. EM Aero California + 078 JR SER Aero-Charter 187 DW UCR Aero Continente 929 N6 ACQ Aero Continente Dominicana 9D Aero Express Del Ecuador - Trans AM © 144 7T Aero Honduras S.A. d/b/a/ Sol Air 4S Aero Lineas Sosa P4 Aero Lloyd Flugreisen GmbH & Co. YP AEF Aero Republica S.A. 845 P5 RPB Aero Zambia + # 509 Z9 Aero-Condor S.A. Q6 Aero Contractors Company of Nigeria Ltd. AJ NIG Aero-Service BF Aerocaribe 723 QA CBE Aerocaribbean S.A. 164 7L CRN Aerocontinente Chile S.A. C7 Aeroejecutivo S.A. de C.V. 456 SX AJO Aeroflot Russian Airlines + # 555 SU AFL Aeroflot-Don 733 D9 DNV Aerofreight Airlines JSC RS Aeroline GmbH 7E AWU Aerolineas Argentinas + # 044 AR ARG Aerolineas Centrales de Colombia (ACES) + 137 VX AES Aerolineas de Baleares AeBal 059 DF ABH Aerolineas Dominicanas S.A. -

Aircraft Refuelling Guide
aircraft refuelling guide 2019/20 australia & new zealand Horn Island australia l Avgas Darwin Gove u Christmas Island Aurukun Jet ] Tindal Jet FS II Kununurra Derby Cairns Halls Creek Broome Townsville Port Hedland NORTHERN Karratha TERRITORY Mt Isa Cloncurry Mackay Cloudbreak Solomon Mine Christmas Creek Barimunya Ginbata/Roy Hill Mine Coondewanna Alice Springs QUEENSLAND Newman Longreach WESTERN Yulara AUSTRALIA (Ayers Rock) Carnarvon Meekatharra Caloundra Roma Redcliffe Toowoomba Brisbane SOUTH Archerfield AUSTRALIA Coolangatta Lismore Leonora NEW SOUTH Olympic Dam Moree Kalgoorlie WALES Inverell Perth Broken Hill Tamworth Jandakot Ceduna Port Macquarie Dubbo Bunbury Maitland Esperance Newcastle Manjimup Bathurst Parafield Sydney Adelaide Bankstown Albany Camden Wagga Wagga Swan Hill Canberra Mangalore Merimbula Horsham Ballarat Essendon Melbourne Moorabbin Warrnambool Stated hours of operation may change without notice. Some airports are not attended VICTORIA continuously during the hours nominated and notice may be required to obtain service. At some locations, an after hours call out fee may apply, which is normally Devonport Launceston calculated by and paid directly to the operator. We recommend pilots phone ahead to check fuel availability and call out fee if applicable. All information and details are correct at the time of printing, November 2019. Hobart Air BP strongly advise that pilots check with the Airfield Representative at relevant TASMANIA locations to accommodate flight requirements. australia head office customer -

Tecnam P2008 Arrives in New Zealand Wet Wings Over Wairarapa
KiwiFlyerTM The New Zealand Aviators’ Marketplace Issue 15 February / March 2011 $ 5.90 inc GST ISSN 1170-8018 Tecnam P2008 arrives in New Zealand Wet Wings Over Wairarapa Walsh Memorial Scout Flying School Products, Services, Accessories, Business News, Events, Training and more. KiwiFlyer The New Zealand Aviators’ Marketplace Comment and Contents From the Editor In this issue WELCOME to our 15th issue of KiwiFlyer. We hope you’ll find 4. First Tecnam P2008 Arrives in NZ plenty of interesting reading and information within. This edition We take a close look at the distinctive announces the arrival of the first Tecnam P2008 LSA for New and capable P2008 which arrived in New Zealand. It is without question a very smart looking aircraft that Zealand just two weeks ago. exhibits some real potential to take on flying school duties as a 10. Wings Over Wairarapa Cessna 152 replacement. When considered along with the P2006T Although rained out on Sunday, there were Twin, for which NZ and Australian sales are accumulating, 2011 is still plenty of spectators and some great shaping up to be a significant year for the company in Australasia. flying displays on Friday and Saturday. In spite of being scheduled for the middle of Summer, the three 16. The Red Checkers Return day Wings Over Wairarapa Airshow had to be cancelled on Sunday After standing down last year, the Red P2008 LSA following torrential rain that virtually submerged the airfield. Checkers are back. Chris Gee interviewed Fortunately, a good many spectators attended on Friday and SQNLDR Jim Rankin. Saturday and enjoyed some superb displays during better patches in the weather. -
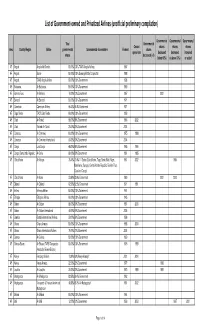
List of Government-Owned and Privatized Airlines (Unofficial Preliminary Compilation)
List of Government-owned and Privatized Airlines (unofficial preliminary compilation) Governmental Governmental Governmental Total Governmental Ceased shares shares shares Area Country/Region Airline governmental Governmental shareholders Formed shares operations decreased decreased increased shares decreased (=0) (below 50%) (=/above 50%) or added AF Angola Angola Air Charter 100.00% 100% TAAG Angola Airlines 1987 AF Angola Sonair 100.00% 100% Sonangol State Corporation 1998 AF Angola TAAG Angola Airlines 100.00% 100% Government 1938 AF Botswana Air Botswana 100.00% 100% Government 1969 AF Burkina Faso Air Burkina 10.00% 10% Government 1967 2001 AF Burundi Air Burundi 100.00% 100% Government 1971 AF Cameroon Cameroon Airlines 96.43% 96.4% Government 1971 AF Cape Verde TACV Cabo Verde 100.00% 100% Government 1958 AF Chad Air Tchad 98.00% 98% Government 1966 2002 AF Chad Toumai Air Tchad 25.00% 25% Government 2004 AF Comoros Air Comores 100.00% 100% Government 1975 1998 AF Comoros Air Comores International 60.00% 60% Government 2004 AF Congo Lina Congo 66.00% 66% Government 1965 1999 AF Congo, Democratic Republic Air Zaire 80.00% 80% Government 1961 1995 AF Cofôte d'Ivoire Air Afrique 70.40% 70.4% 11 States (Cote d'Ivoire, Togo, Benin, Mali, Niger, 1961 2002 1994 Mauritania, Senegal, Central African Republic, Burkino Faso, Chad and Congo) AF Côte d'Ivoire Air Ivoire 23.60% 23.6% Government 1960 2001 2000 AF Djibouti Air Djibouti 62.50% 62.5% Government 1971 1991 AF Eritrea Eritrean Airlines 100.00% 100% Government 1991 AF Ethiopia Ethiopian -

Team 1148 Report 2014
TEAM 1148 REPORT 2014 If Mount Taranaki erupted, how much would it cost the aviation industry? Introduction: New Zealand is home to over 60 volcanoes, this is because of the boundaries of the Australasian and pacific volcanic plates that New Zealand is located smack bang in the middle of. Making new Zealand a volcanic hotspot, that has created volcanoes nationwide. The thing with New Zealand is that it also brings over 2,700,000 tourist into the country annually. Mt Taranaki is situated in New Plymouth which is slightly under the centre of the north island of New Zealand on the west coast shown in the picture to the right. Now if an eruption from Mt Taranaki occurred sending tephra (volcanic ash) into the sky it would definitely have an effect on the domestic flights of New Zealand. Like when Mt Eyjafjallajӧkull in Iceland erupted in 2010 producing over 0.25 cubic kilometres of tephra. Closing down around 20 countries airspace and costing the airline industries an estimated $200 million USD per day (estimated by the International Air Transport Association). So it is our task to investigate and find out how much it would cost the aviation industry if Mt Taranaki was to erupt. Taranaki has had a long history of eruptions, right back to 130, 000 years ago. Since then, Taranaki has been actively erupting every 500 years with many of the eruptions being of a Plinian type. Plinian eruptions are a specific type/process of eruptions that have specific qualities about them that differentiates them from many other types of eruptions. -
Commerce Commission Draft Determinations
ISSN NO. 0114-2720 J5633/J5645 PUBLIC VERSION Commerce Commission Draft Determinations Determinations pursuant to the Commerce Act 1986 in the matter of an application for authorisation of a business acquisition and in the matter of an application for authorisation of certain restrictive business practices and involving: QANTAS AIRWAYS LIMITED and AIR NEW ZEALAND LIMITED The Commission: MJ Belgrave PR Rebstock PJ Taylor DF Curtin D Bates QC Summary of Applications: The subscription by Qantas Airways Limited of up to 22.5% of the voting equity in Air New Zealand Limited pursuant to a Subscription Agreement between Air New Zealand Limited and Qantas Airways Limited (the proposed Acquisition); and The implementation by Air New Zealand Limited and Qantas Airways Limited of the terms of a Strategic Alliance arrangement which creates a Joint Airline Operation network (the proposed Arrangement) Draft Determinations: The Commission’s draft determination, on the basis of the information provided to date, is that it would be likely to decline an authorisation for the proposed Acquisition pursuant to s 67(3)(c) of the Act. The Commission’s draft determination, on the basis of the information provided to date, is that it would be likely to decline an authorisation for the proposed Arrangement pursuant to s 61(1)(b) of the Act. Date 10 April 2003 CONFIDENTIAL MATERIAL IN THIS REPORT IS CONTAINED IN SQUARE BRACKETS CONTENTS EXECUTIVE SUMMARY........................................................................................................ 9 Proposed -

Commerce Commission Final Determination
ISSN NO. 0114-2720 J5633 PUBLIC VERSION Commerce Commission Final Determination Determinations pursuant to the Commerce Act 1986 in the matter of an application for authorisation of a business acquisition and in the matter of an application for authorisation of certain restrictive business practices and involving: AIR NEW ZEALAND LIMITED and QANTAS AIRWAYS LIMITED The Commission: PR Rebstock PJ Taylor DF Curtin D Bates QC Summary of Applications: The subscription by Qantas Airways Limited of up to 22.5% of the voting equity in Air New Zealand Limited pursuant to a Subscription Agreement between Air New Zealand Limited and Qantas Airways Limited (the proposed Acquisition); and The implementation by Air New Zealand Limited and Qantas Airways Limited of the terms of a Strategic Alliance arrangement which creates a Joint Airline Operation network (the proposed Arrangement) Final Determinations: The Commission determines to decline authorisation for the proposed Acquisition pursuant to s 67(3)(c) of the Act. The Commission determines to decline authorisation for the proposed Arrangement pursuant to s 61(6) of the Act. Date: 23 October 2003 CONFIDENTIAL MATERIAL IN THIS REPORT IS CONTAINED IN SQUARE BRACKETS i EXECUTIVE SUMMARY1 Proposed Alliance Between Air NZ and Qantas 1. On 9 December 2002 the Commerce Commission (the Commission) received two interdependent applications for authorisation from Air New Zealand Ltd (Air NZ) and Qantas Airways Ltd (Qantas). 2. The first application by Qantas, made under section 67(1) of the Commerce Act, relates to a proposed “share purchase agreement” whereby Qantas would acquire 22.5% of the voting equity in Air NZ. -
(EC) No 748/2009 on the List of Aircraft Operators
11.2.2012 EN Official Journal of the European Union L 39/1 II (Non-legislative acts) REGULATIONS COMMISSION REGULATION (EU) No 100/2012 of 3 February 2012 amending Regulation (EC) No 748/2009 on the list of aircraft operators that performed an aviation activity listed in Annex I to Directive 2003/87/EC of the European Parliament and of the Council on or after 1 January 2006 specifying the administering Member State for each aircraft operator also taking into consideration the expansion of the Union emission trading scheme to EEA-EFTA countries (Text with EEA relevance) THE EUROPEAN COMMISSION, dependent on the inclusion in the list of aircraft operators established by the Commission on the basis of Article 18a (3) of that Directive. Having regard to the Treaty on the Functioning of the European Union, (5) Directive 2008/101/EC was incorporated into the Agreement on the European Economic Area by Having regard to Directive 2003/87/EC of the European Decision of the EEA Joint Committee No 6/2011 of Parliament and of the Council of 13 October 2003 establishing 1 April 2011, amending Annex XX (Environment) to a scheme for greenhouse gas emission allowance trading within the EEA Agreement ( 4). the Community and amending Council Directive 96/61/EC ( 1), and in particular Article 18a(3)(b) thereof, (6) The extension of the aviation provisions of the Union emission trading scheme to EEA-EFTA countries implies Whereas: that the criteria set under Article 18a (1) of Directive 2003/87/EC to determine aircraft operator's adminis tering Member State must be continuously taken into (1) Directive 2008/101/EC of the European Parliament and account, thus, certain aircraft operators should be 2 of the Council ( ) amended Directive 2003/87/EC to allocated to the EEA-EFTA countries for administration. -

Queenstown Bungy Limited and Taupo Bungy Limited Together Are Termed the Parties
Public Version COMMERCE ACT 1986: BUSINESS ACQUISITION SECTION 66: NOTICE SEEKING CLEARANCE Date: 30 August 2019 The Registrar Mergers and Acquisitions Commerce Commission PO Box 2351 Wellington Pursuant to section 66(1) of the Commerce Act 1986 notice is hereby given seeking clearance of a proposed business acquisition. Part 1: Overview This is an application for clearance pursuant to section 66(1) of the Commerce Act 1986 made by Queenstown Bungy Limited (Purchaser ) to acquire adventure tourism operations located at Taupo owned by Taupo Bungy Limited (the Vendor ) (the Proposed Acquisition ). Queenstown Bungy Limited and Taupo Bungy Limited together are termed the Parties . The assets the Purchaser will acquire in the Proposed Acquisition comprise the business and physical assets used for the Vendor’s bungy and swing business in Taupo, known as Taupo Bungy. The Purchaser operates bungy, swing, catapult jump sites, and related businesses in Queenstown and Auckland, but does not currently have any operations in the Taupo area or surrounding region. The Purchaser considers that Taupo Bungy’s operations occur within a broad retail tourism activities market, but appreciates that it may be appropriate to consider defining the relevant market for the purposes of this application as the market for the provision of retail tourism adventure activities in the Central North Island region. This is similar to the market defined in the Commission’s 2003 clearance of Bungy New Zealand’s acquisition of Pipeline Bungy in Queenstown. The Proposed Acquisition will not, and will not be likely to, cause a substantial lessening of competition as: 1.5.1 It will not result in any aggregation of market share, as the Purchaser does not currently operate in the Central North Island region. -

Use CTL/F to Search for INACTIVE Airlines on This Page - Airlinehistory.Co.Uk
The World's Airlines Use CTL/F to search for INACTIVE airlines on this page - airlinehistory.co.uk site search by freefind search Airline 1Time (1 Time) Dates Country A&A Holding 2004 - 2012 South_Africa A.T. & T (Aircraft Transport & Travel) 1981* - 1983 USA A.V. Roe 1919* - 1920 UK A/S Aero 1919 - 1920 UK A2B 1920 - 1920* Norway AAA Air Enterprises 2005 - 2006 UK AAC (African Air Carriers) 1979* - 1987 USA AAC (African Air Charter) 1983*- 1984 South_Africa AAI (Alaska Aeronautical Industries) 1976 - 1988 Zaire AAR Airlines 1954 - 1987 USA Aaron Airlines 1998* - 2005* Ukraine AAS (Atlantic Aviation Services) **** - **** Australia AB Airlines 2005* - 2006 Liberia ABA Air 1996 - 1999 UK AbaBeel Aviation 1996 - 2004 Czech_Republic Abaroa Airlines (Aerolineas Abaroa) 2004 - 2008 Sudan Abavia 1960^ - 1972 Bolivia Abbe Air Cargo 1996* - 2004 Georgia ABC Air Hungary 2001 - 2003 USA A-B-C Airlines 2005 - 2012 Hungary Aberdeen Airways 1965* - 1966 USA Aberdeen London Express 1989 - 1992 UK Aboriginal Air Services 1994 - 1995* UK Absaroka Airways 2000* - 2006 Australia ACA (Ancargo Air) 1994^ - 2012* USA AccessAir 2000 - 2000 Angola ACE (Aryan Cargo Express) 1999 - 2001 USA Ace Air Cargo Express 2010 - 2010 India Ace Air Cargo Express 1976 - 1982 USA ACE Freighters (Aviation Charter Enterprises) 1982 - 1989 USA ACE Scotland 1964 - 1966 UK ACE Transvalair (Air Charter Express & Air Executive) 1966 - 1966 UK ACEF Cargo 1984 - 1994 France ACES (Aerolineas Centrales de Colombia) 1998 - 2004* Portugal ACG (Air Cargo Germany) 1972 - 2003 Colombia ACI -

ZK Register Review August-October-2012
ZK Register Review provided courtesy of Hawker Pacific contributed by Penny Belworthy ARRIVALS - August/September/October 2012 DHP Beech B200 Hawker Pacific NZ Ltd Papakura Aeroplane in Singapore with 14 Squadron and increased reserve power, improved altitude FEB The Vintage Aviator FE2b-1 The Vintage Aviator Limited Masterton Aeroplane FKG Fokker D-VII Replica Dr G G Ritchie Ashburton Microlight Class 1 ZK-VNM DH112 Venom remembers it as a “potent warplane due to performance, fifth seat, and large baggage HAK MBB BO 105 CBS-5 Oceania Aviation Limited Papakura Helicopter HCE Robinson R66 R J & J D Griffiths Westport Helicopter its capacity to carry a couple of thousand- compartment. Operations Manager for HMI Bell 206B Helicopters South Canterbury Ltd Timaru Helicopter pound bombs, rockets and cannon”. The Outgro Aviation, Brian Knight said they HQC MBB MBB-BK117 A-3 Airwork (NZ) Limited Papakura Helicopter HQD MBB MBB-BK117 A-3 Airwork (NZ) Limited Papakura Helicopter colour scheme on VNM is based on the now have two R66 aircraft in operation HQI MBB MBB-BK117 B-2 Helicopters Otago Limited Mosgiel Helicopter HQJ MBB MBB-BK117 A-3 Airwork (NZ) Limited Papakura Helicopter original Venom scheme that Trevor Bland around New Zealand and have flown HQO MBB MBB-BK117 A-3 Airwork (NZ) Limited Papakura Helicopter IAI MBB BO 105 S Mr B J Comerford Porirua Helicopter flew while serving. over 800 hours to date between the two. IAJ MBB BO 105 S Mr B J Comerford Porirua Helicopter IBV Aerospatiale AS 350B2 Mr B J Comerford Porirua Helicopter Around 1400 Venoms were built and For any more information email: info@ ICP Robinson R44 II North Shore Helicopters Limited Albany Helicopter it was developed into a night fighter and a outgroaviation.co.nz IJH Bell 206L-3 Salt Air Limited Paihia Helicopter FOR ALL FIXED WING AND ROTARY IJO Eurocopter AS 350 B3 Faram Aviation Group Limited Hastings Helicopter MAINTENANCE, REPAIR AND naval version, the Sea Venom.