Information for Students of Medical Faculties
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

General Pathomorpholog.Pdf
Ukrаiniаn Medicаl Stomаtologicаl Аcаdemy THE DEPАRTАMENT OF PАTHOLOGICАL АNАTOMY WITH SECTIONSL COURSE MАNUАL for the foreign students GENERАL PАTHOMORPHOLOGY Poltаvа-2020 УДК:616-091(075.8) ББК:52.5я73 COMPILERS: PROFESSOR I. STАRCHENKO ASSOCIATIVE PROFESSOR O. PRYLUTSKYI АSSISTАNT A. ZADVORNOVA ASSISTANT D. NIKOLENKO Рекомендовано Вченою радою Української медичної стоматологічної академії як навчальний посібник для іноземних студентів – здобувачів вищої освіти ступеня магістра, які навчаються за спеціальністю 221 «Стоматологія» у закладах вищої освіти МОЗ України (протокол №8 від 11.03.2020р) Reviewers Romanuk A. - MD, Professor, Head of the Department of Pathological Anatomy, Sumy State University. Sitnikova V. - MD, Professor of Department of Normal and Pathological Clinical Anatomy Odessa National Medical University. Yeroshenko G. - MD, Professor, Department of Histology, Cytology and Embryology Ukrainian Medical Dental Academy. A teaching manual in English, developed at the Department of Pathological Anatomy with a section course UMSA by Professor Starchenko II, Associative Professor Prylutsky OK, Assistant Zadvornova AP, Assistant Nikolenko DE. The manual presents the content and basic questions of the topic, practical skills in sufficient volume for each class to be mastered by students, algorithms for describing macro- and micropreparations, situational tasks. The formulation of tests, their number and variable level of difficulty, sufficient volume for each topic allows to recommend them as preparation for students to take the licensed integrated exam "STEP-1". 2 Contents p. 1 Introduction to pathomorphology. Subject matter and tasks of 5 pathomorphology. Main stages of development of pathomorphology. Methods of pathanatomical diagnostics. Methods of pathomorphological research. 2 Morphological changes of cells as response to stressor and toxic damage 8 (parenchimatouse / intracellular dystrophies). -

Clinical Case
Annals of Oncology 9: 95-100. 1998. © 1998 Kluwer Academic Publishers. Printed in the Netherlands. Clinical case Management of an isolated thymic mass after primary therapy for lymphoma S. Anchisi, R. Abele, M. Guetty-Alberto & P. Alberto Division of Oncology, Department of Medicine, University Hospital, Geneva, Switzerland Key words: CT scan, galliumscintigraphy, Hodgkin's disease, lymphoma, residual mass, thymus hyperplasia Introduction pose tissue constituting less than 40% of the total mass. The patient is still in CR 51 months after the end of The appearance of an anterior mediastinal mass during treatment. the follow-up of patients successfully treated for lym- phoma is worrisome, and may suggest treatment failure. Case 2 However, benign 'rebound' thymic hyperplasia (TH), a well documented phenomenon in children [1-3] and in A 26-year-old woman presented with a stage IVB young adults treated for malignant testicular teratoma nodular sclerosing HD, with liver and spleen infiltration [4], is an important differential diagnosis even in the and a bulky mediastinum. adult population [5]. Magnetic resonance imaging (MRI) disclosed a dif- fuse infiltration of the thoracic and lumbar vertebral bodies. The result of a bone-marrow biopsy was normal. Case reports Five courses of VEMP chemotherapy (vincristine, eto- poside, mitoxantrone, prednisone) produced a partial Between July 1990 and December 1994, we observed response greater than 75%. The treatment was intensi- two cases of TH among 58 adults treated consecutively fied with a BEAM chemotherapy (carmustine, etoposide, at our institution. Thirty of the 58 had de novo Hodgkin's cytosine arabinoside, melphalan), followed by an autol- disease (HD) and 28 had aggressive non-Hodgkin's ogous bone marrow transplant (BMT). -

Preventing Thymus Involution in K5.Cyclin D1 Transgenic Mice Sustains the Naïve T Cell Compartment with Age
The Texas Medical Center Library DigitalCommons@TMC The University of Texas MD Anderson Cancer Center UTHealth Graduate School of The University of Texas MD Anderson Cancer Biomedical Sciences Dissertations and Theses Center UTHealth Graduate School of (Open Access) Biomedical Sciences 12-2015 PREVENTING THYMUS INVOLUTION IN K5.CYCLIN D1 TRANSGENIC MICE SUSTAINS THE NAÏVE T CELL COMPARTMENT WITH AGE Michelle L. Bolner Follow this and additional works at: https://digitalcommons.library.tmc.edu/utgsbs_dissertations Part of the Cell Biology Commons, Immunology and Infectious Disease Commons, Molecular Biology Commons, and the Molecular Genetics Commons Recommended Citation Bolner, Michelle L., "PREVENTING THYMUS INVOLUTION IN K5.CYCLIN D1 TRANSGENIC MICE SUSTAINS THE NAÏVE T CELL COMPARTMENT WITH AGE" (2015). The University of Texas MD Anderson Cancer Center UTHealth Graduate School of Biomedical Sciences Dissertations and Theses (Open Access). 636. https://digitalcommons.library.tmc.edu/utgsbs_dissertations/636 This Dissertation (PhD) is brought to you for free and open access by the The University of Texas MD Anderson Cancer Center UTHealth Graduate School of Biomedical Sciences at DigitalCommons@TMC. It has been accepted for inclusion in The University of Texas MD Anderson Cancer Center UTHealth Graduate School of Biomedical Sciences Dissertations and Theses (Open Access) by an authorized administrator of DigitalCommons@TMC. For more information, please contact [email protected]. PREVENTING THYMUS INVOLUTION IN K5.CYCLIN D1 TRANSGENIC MICE SUSTAINS THE NAÏVE T CELL COMPARTMENT WITH AGE BY Michelle Lynn Bolner, Ph.D. Candidate APPROVED: _____________________________________ Ellen R. Richie, Ph.D., Supervisory Professor _____________________________________ Shawn B. Bratton, Ph.D. _____________________________________ David G. Johnson, Ph.D. -

Rebound Thymic Hyperplasia After Chemotherapy in Children
View metadata, citation and similar papers at core.ac.uk brought to you by CORE + MODEL provided by Elsevier - Publisher Connector Pediatrics and Neonatology (2016) xx,1e7 Available online at www.sciencedirect.com ScienceDirect journal homepage: http://www.pediatr-neonatol.com ORIGINAL ARTICLE Rebound Thymic Hyperplasia after Chemotherapy in Children with Lymphoma Chih-Ho Chen a, Chih-Chen Hsiao a, Yu-Chieh Chen a, Sheung-Fat Ko b, Shu-Hua Huang c, Shun-Chen Huang d, Kai-Sheng Hsieh a, Jiunn-Ming Sheen a,* a Department of Pediatrics, Chang Gung Memorial HospitaldKaohsiung Medical Center, Chang Gung University College of Medicine, Kaohsiung, Taiwan b Department of Radiology, Chang Gung Memorial HospitaldKaohsiung Medical Center, Chang Gung University College of Medicine, Kaohsiung, Taiwan c Department of Nuclear Medicine, Chang Gung Memorial HospitaldKaohsiung Medical Center, Chang Gung University College of Medicine, Kaohsiung, Taiwan d Department of Pathology, Chang Gung Memorial HospitaldKaohsiung Medical Center, Chang Gung University College of Medicine, Kaohsiung, Taiwan Received Sep 24, 2015; received in revised form Nov 30, 2015; accepted Feb 5, 2016 Available online --- Key Words Background: Development of mediastinal masses after completion of chemotherapy in pediat- lymphoma; ric patients with malignant lymphoma is worrisome and challenging to clinicians. prognosis; Methods: We performed a retrospective review of 67 patients with lymphoma treated at our rebound thymic hospital from January 1, 2001 to June 1, 2013. Patients who received at least two chest hyperplasia; computed tomography (CT) examinations after complete remission (CR) was achieved were recurrence further analyzed. Gallium-67 scans and positron emission tomography (PET) were recorded and compared between these patients. -

Normative Values of Thymus in Healthy Children; Stiffness by Shear Wave Elastography
Diagn Interv Radiol 2020; 26:147–152 PEDIATRIC RADIOLOGY © Turkish Society of Radiology 2020 ORIGINAL ARTICLE Normative values of thymus in healthy children; stiffness by shear wave elastography Zuhal Bayramoğlu PURPOSE Mehmet Öztürk Thymus grows after birth, reaches maximal size after the first few years and involutes by puber- Emine Çalışkan ty. Because of the postnatal developmental and involutional duration, we aimed to investigate normal stiffness values of mediastinal thymus by shear wave elastography (SWE) in different age Hakan Ayyıldız groups of children and discuss imaging findings of thymus. İbrahim Adaletli METHODS We prospectively examined 146 children (90 girls, 56 boys) who underwent a thyroid or neck ultrasound examination. All subjects underwent ultrasound and SWE evaluation of mediastinal thymus by parasternal and suprasternal approach. We grouped the subjects based on age as 0 to 2 months, >2 to 6 months, >6 months to 2 years, >2 to 5 years, >5 to 8 years, and greater than 8 years old. We investigated differences of mean shear wave elasticity (kPa) and shear wave veloc- ity (m/s) values among age groups and the association of SWE values with age, body mass index (BMI), height, and weight of the patients. RESULTS Median and range of age, height, weight, and BMI were 24 months (2–84 months), 85 cm (55– 120 cm), 12 kg (4.55–22 kg), 15.37 kg/m2 (13.92–17.51 kg/m2), 11 cc (2.64–23.15 cc), respectively. Mean shear wave elasticity of thymus of all participants was 6.76±1.04 kPa. Differences of mean elasticity values among the age and gender groups were not statistically significant. -

(12) Patent Application Publication (10) Pub. No.: US 2007/0292883 A1 Ossovskaya Et Al
US 20070292883A1 (19) United States (12) Patent Application Publication (10) Pub. No.: US 2007/0292883 A1 Ossovskaya et al. (43) Pub. Date: Dec. 20, 2007 (54) METHOD OF TREATING DISEASES WITH (52) U.S. Cl. ............................. 435/6: 435/723: 514/394; PARP INHIBITORS 514/543; 514/309; 514/312: 435/91.2: 514/415: 514/457 (76) Inventors: Valeria S. Ossovskaya, San Francisco, CA (US); Barry M. Sherman, Hillsborough, CA (US) (57) ABSTRACT Correspondence Address: SSSSSS(pDRICH & ROSAT The present invention relates to methods of identifying a PALO ALTO, CA 94304-1050 (US) disease treatable with PARP modulators by identifying a 9 level of PARP in a sample of a subject, making a decision (21) Appl. No.: 11/818,210 regarding identifying the disease treatable by the PARP modulators wherein the decision is made based on the level (22) Filed: Jun. 12, 2007 of PARP. The method further comprises of treating the O O disease in the subject with the PARP modulators. The Related U.S. Application Data methods relate to identifying up-regulated PARP in a disease (60) Provisional application No. 60/804,563, filed on Jun. and making a decision regarding the treatment of the disease 12, 2006. Provisional application No. 60/866,602, with PARP inhibitors. The extent of PARP up-regulation in filed on Nov. 20, 2006. a disease can also help in determining the efficacy of the treatment with PARP inhibitors. The present invention dis Publication Classification closes various diseases that have up-regulated or down regulated PARP and can be treated with PARP inhibitors or (51) , C. -

Hacettepe University Faculty D~Partment of Radiology Computed Tomography
T.C. HACETTEPE UNIVERSITYFACULTY OF EDICI, E D~PARTMENT OF RADIOLOGY DIAGNOSIS OF THYMOMA BY COMPUTED TOMOGRAPHY Dr. 11. Naz t r Far 1d 19YL Ankara ~5394 - .... '::~·.. - . -~ .· : . Contents 1- Introduction. 1 2- Anatomy of the tl1y::::us. .. ................ 5 3- Subjects and met11ocs. 19 4- Results. 22 5- Dlscussion. 24 6- Conclusion. • ..•............... -... ' ...• ' ..... 3 1 7- References. ' .......................... ,' ... 3 3 (t) Introduction Thymomas are solid neoplasms that occur in association with myasthenia gravis or others less common conditions ( red cell aplasia,hypogammaglob~linemia) or sporadically .. Because of the proximity of the thymus gland to the major mediastinal vascular structure, small thymic lesions often are not detectable on plain chest radiography or conventional tomography. So as a result computed tomography of the mediastinum sho~ld be the imaging procedure of choice ·when thymic pathology is suspected (1). The 10-15% incidence of thymomas in patients with myasthenia gravis has led to routine CT screening of the ·anterior superior mediastinum in many of these patients, especially if these patients recently exacerbated the symptoms. Comput~d tomography also "is r~commended to search for a thymic·carcinoid whenever there is clinical suspicion of ectopic adrencorticotrphic hormone (ACTH) production causing cushing syndrome (2). The presence of thymoma must always be suspected in patients with myasthenia gravis because about 10-15% will have such a tumor (4). Accuracy of radiologic detection of thymoma in association with myasthenia gravis has varied widely (2-7). The evaluations is complicated because fats cpntents of thymus increase with the age- and thymic size is highly variable (8-12). Other method including atteriography (13) Thymic venography (14) Pneumomediastinography (15) ultrasonography (16) and several other methods have been ( 2) found useful in some cases but none of these methods have been ~idely accepted for screening patients with myasthenia gravis. -
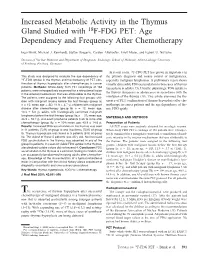
Increased Metabolic Activity in the Thymus Gland Studied with 18F-FDG PET: Age Dependency and Frequency After Chemotherapy
Increased Metabolic Activity in the Thymus Gland Studied with 18F-FDG PET: Age Dependency and Frequency After Chemotherapy Ingo Brink, Michael J. Reinhardt, Stefan Hoegerle, Carsten Altehoefer, Ernst Moser, and Egbert U. Nitzsche Division of Nuclear Medicine and Department of Diagnostic Radiology, School of Medicine, Albert-Ludwigs University of Freiburg, Freiburg, Germany In recent years, 18F-FDG PET has grown in importance in This study was designed to evaluate the age dependency of the primary diagnosis and course control of malignancies, 18F-FDG uptake in the thymus and the frequency of PET con- especially malignant lymphomas. A preliminary report shows firmation of thymus hyperplasia after chemotherapy in cancer visually discernible FDG accumulation in two cases of thymus patients. Methods: Whole-body FDG PET recordings of 168 hyperplasia in adults (15). Usually, physiologic FDG uptake in patients were retrospectively examined for a retrosternal lesion the thymus disappears in adolescence in accordance with the in the anterior mediastinum that was attributable to the thymus. The patients were assigned to the following four groups: chil- involution of the thymus (16). This article examines the fre- dren with malignant lesions before the first therapy (group Ia; quency of PET confirmation of thymus hyperplasia after che- n ϭ 15; mean age Ϯ SD, 11.9 Ϯ 3.7 y), children with malignant motherapy in cancer patients and the age dependency of thy- disease after chemotherapy (group Ib; n ϭ 12; mean age, mic FDG uptake. 10.3 Ϯ 5.0 y), adults with histologically confirmed malignant lymphoma before the first therapy (group IIa; n ϭ 37; mean age, MATERIALS AND METHODS 43.9 Ϯ 16.7 y), and adult lymphoma patients 3 wk to 4 mo after chemotherapy (group IIb; n ϭ 104; mean age, 40.9 Ϯ 14.6 y). -

W O 2009/100159 A3
(12) INTERNATIONAL APPLICATION PUBLISHED UNDER THE PATENT COOPERATION TREATY (PCT) (19) World Intellectual Property Organization IN International Bureau (10) International Publication Number (43) International Publication Date 13 August 2009 (13.08.2009) PCT W O 2009/100159 A3 (51) International Patent Classification: (74) Agents: HOFFMANN, David, C. et al.; Morrison & Fo C12Q 1/68 (2006.01) C07H 21/00 (2006.01) erster LLP, 755 Page Mill Road, Palo Alto, CA C12N15/11 (2006.01) A61K 48/00 (2006.01) 94304-1018 (US). (21) International Application Number: (81) Designated States (unless otherwise indicated, for every PCT/US2009/033117 kind of nationalprotection available>: A, AG, AL, AM, BY, BZ, (22) International Filing Date:AT, AU, AZ, BA, BB, BG, , BR, BW, CA, N , C O , CR , C U , CZ , D E, D K , D M , D O , D Z , 4 In er a io4 a209Feruay Fiin 04.2.209)Date: EC, EE,C H , EG,C ES, Fl, GB, GD, GE, GH, GM, GT, FIN, (25) Filing Language: English HR, HU, ID, IL, IN, IS, JP, KE, KG, KM, KN, KP, KR, KZ, LA, LC, LK, LR, LS, LT, LU, LY, MA, MD, ME, (26) Publication Language: English MG, MK, MN, MW, MX, MY, MZ, NA, NG, NI, NO, (30) Priority Data: NZ, OM, PG, PH, PL, PT, RO, RS, RU, SC, SD, SE, SG, 61/026,077 4 February 2008 (04.02.2008) US SK, SL, SM, ST, SV, SY, TJ, TM, TN, TR, TT, TZ, UA, UG, US, UZ, VC, VN, ZA, ZM, ZW. (71) Applicant (for all designated States except US): BIPAR SCIENCES, INC. -

GENOMIC and EPIGENOMIC PREDICTORS for VARIOUS CLINICAL PHENOTYPES of MYASTHENIA GRAVIS DOI: 10.36740/Wlek202103117
© Aluna Publishing Wiadomości Lekarskie, VOLUME LXXIV, ISSUE 3 PART 1, MARCH 2021 ORIGINAL ARTICLE GENOMIC AND EPIGENOMIC PREDICTORS FOR VARIOUS CLINICAL PHENOTYPES OF MYASTHENIA GRAVIS DOI: 10.36740/WLek202103117 Elena M. Klimova1, Larisa A. Drozdova1, Elena V. Lavinskaya1, Dmitriy V. Minukhin2, Iryna O. Kudrevych3, Oleksandr M. Kudrevych4 1STATE INSTITUTION «ZAYCEV V.T. INSTITUTE OF GENERAL AND URGENT SURGERY OF NATIONAL ACADEMY OF MEDICAL SCIENCES OF UKRAINE», KHARKIV, UKRAINE 2KHARKIV NATIONAL MEDICAL UNIVERSITY, KHARKIV, UKRAINE 3KHARKIV MEDICAL ACADEMY OF POSTGRADUATE EDUCATION, KHARKIV, UKRAINE 4 V. N. KARAZIN KHARKIV NATIONAL UNIVERSITY, KHARKIV, UKRAINE ABSTRACT The aim: To evaluate the relationship of certain alleles of HLA class II leukocyte antigens and the profile of antibodies to various subunits of nicotinic acetylcholine receptors (nAChR), the level of Treg lymphocytes and the serum concentration of anti-inflammatory IL-10 for various clinical myasthenia gravis phenotypes. Materials and methods: We examined 217 patients with thymus-independent myasthenia (n = 42) and thymus-dependent myasthenia, among them patients with thymus hyperplasia (n = 108) and thymoma (n = 67). We used the following methods: ELISA, flow cytometry, light and fluorescence microscopy. Results: Certain genomic (polymorphism of leukocyte HLA-DR antigens) and epigenomic (antibodies to α1 and α7 nAChR subunits, expression of Treg lymphocytes and concentration of cytokines) predictors were identified for various myasthenia phenotypes. The presence of HLA haplotypes DR2 and DR7 in some young patients with M with disease progression led to the development of myasthenia gravis with thymoma (MT) at an older age. The presence of α7 nAChR subunit on thymocyte mitochondria was revealed, which is an additional autoimmune target for autoantibodies in patients with myasthenia gravis. -

421.Full.Pdf
THE AMERICAN TOURNAL OF CANCER d A Continuation of The Journal of Cancer Research THE THYMOMA AND THYMIC HYPERPLASIA IN MYASTHENIA GRAVIS WITH OBSERVATIONS ON THE GENERAL PATHOLOGY' E. H. NORRIS, M.D (From the DcpnrtmPnt oj Pathology, Unizlersity of Minnerota) Since the comprehensive study by Bell in 1917 no systematic treatise on the thymic tumors of myasthenia gravis has appeared. It might be expected that the past twenty years would have added the records of many more cases to the literature and have extended our knowledge of the pathological anatomy of myasthenia gravis and the associated thymic tumors. On the contrary but few cases with autopsy findings have been reported and our conceptions con- cerning the morbid anatomy of this disease are much the same as they were in 1917. In the period from 1901, the year in which Weigert published the record of the first case of myasthenia gravis with an associated thymus tumor, to 1917, Bell found published reports of 56 autopsied cases of this disease. He wrote: '' The thymus was described as enlarged in seventeen of these cases; and in ten others it contained a tumor. Therefore some form of thymic involvement seems to occur in nearly half the cases of myasthenia gravis." Since 1917 the records of 6 more autopsies have been published and 5 of these showed thymic lesions. Of the 4 cases to be reported here, 2 had thymic lesions which were recognized. I am of the opinion that pathologic changes may be found in the thymus in cases of myasthenia gravis in direct ratio to the care with which they are sought. -

Seminars in Immunology
SEMINARS IN IMMUNOLOGY SEMINARS IN IMMUNOLOGY Edited by András Kristóf Fülöp Written and translated by Éva Pállinger Edit Buzás András Falus György Nagy Marianna Csilla Holub Sára Tóth László Kőhidai Zsuzsanna Pál Scientific reviewers Edit Buzás András Falus English proofreading Adrienn Ádám Semmelweis University • Budapest, 2012 © András Kristóf Fülöp, 2012 2 Manuscript closed on 31 May 2012 ISBN 978-963-9129-82-5 Semmelweis University Responsible for publishing: Semmelweis University Editor: András Kristóf Fülöp Technical editor: Adrienn Ádám Length: 223 pages 3 CONTENTS 1. INTRODUCTION (ÉVA PÁLLINGER) ......................................................................................................... 10 1.1. Basic terms ..................................................................................................................................... 10 1.1.1. Innate and acquired immunity ......................................................................................................... 10 1.1.2. What does the immune system recognize? .................................................................................... 11 1.1.3. What types of receptors can recognize antigens? .......................................................................... 11 1.1.3.1. PRR (pattern recognition receptors, pathogen recognition receptors) ............................................ 11 1.1.3.2. T cell receptor (TCR) ......................................................................................................................