The Hidden Injury. Updating Awareness of the Latest Research of Concussion in Tennis
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
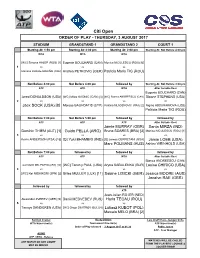
Citi Open ORDER of PLAY - THURSDAY, 3 AUGUST 2017
Citi Open ORDER OF PLAY - THURSDAY, 3 AUGUST 2017 STADIUM GRANDSTAND 1 GRANDSTAND 2 COURT 1 Starting At: 1:50 pm Starting At: 2:00 pm Starting At: 2:00 pm Starting At: Not Before 4:00 pm WTA WTA WTA [WC] Simona HALEP (ROU) [1] Eugenie BOUCHARD (CAN) Monica NICULESCU (ROU) [6] 1 vs vs vs Mariana DUQUE-MARIÑO (COL) Andrea PETKOVIC (GER) Patricia Maria TIG (ROU) Not Before 4:00 pm Not Before 4:00 pm followed by Starting At: Not Before 4:00 pm ATP ATP WTA After Suitable Rest Eugenie BOUCHARD (CAN) Jared DONALDSON (USA) [WC] Milos RAONIC (CAN) [3] [WC] Bianca ANDREESCU (CAN) Sloane STEPHENS (USA) 2 vs vs vs vs Jack SOCK (USA) [8] Marcos BAGHDATIS (CYP) Kristina MLADENOVIC (FRA) [2] Nigina ABDURAIMOVA (UZB) Patricia Maria TIG (ROU) Not Before 5:00 pm Not Before 5:00 pm followed by followed by ATP ATP ATP After Suitable Rest Jamie MURRAY (GBR) Sania MIRZA (IND) Dominic THIEM (AUT) [1] Guido PELLA (ARG) Bruno SOARES (BRA) [3] Monica NICULESCU (ROU) [1] 3 vs vs vs vs Kevin ANDERSON (RSA) [15] [Q] Yuki BHAMBRI (IND) [Q] James CERRETANI (USA) Jamie LOEB (USA) Marc POLMANS (AUS) Ashley WEINHOLD (USA) Not Before 7:00 pm followed by followed by followed by ATP ATP WTA After Suitable Rest Bianca ANDREESCU (CAN) Juan Martin DEL POTRO (ARG) [13] [WC] Tommy PAUL (USA) Aryna SABALENKA (BLR) Louisa CHIRICO (USA) 4 vs vs vs vs [WC] Kei NISHIKORI (JPN) [2] Gilles MULLER (LUX) [11] Sabine LISICKI (GER) Jessica MOORE (AUS) Jocelyn RAE (GBR) followed by followed by followed by ATP Jean-Julien ROJER (NED) Alexander ZVEREV (GER) [5] Daniil MEDVEDEV (RUS) Horia TECAU (ROU) 5 vs vs vs Tennys SANDGREN (USA) [WC] Grigor DIMITROV (BUL) [4] Lukasz KUBOT (POL) Marcelo MELO (BRA) [2] Kerrilyn Cramer Keely O'Brien Lars Graff/ Hans-Juergen Ochs WTA Supervisor(s) Tournament Director(s) ATP Supervisor(s) Order of Play released : 3 August 2017 at 01:34 Pablo Juarez ATP - Tour Manager Ali Nili ATP / WTA - Referee MATCHES WILL BE CALLED ANY MATCH ON ANY COURT FROM THE PLAYERS' LOUNGE & MAY BE MOVED LOCKER-ROOM. -

The Liverpool International Tennis Tournament 18Th to 22Nd June
THE LIVERPOOL INTERNATIONAL TENNIS TOURNAMENT 18TH TO 22ND JUNE 2 14 Partnership Proposal for the biggest Tennis Exhibition in Europe www.northern-vision.co.uk www.liverpooltennis.co.uk Liverpool International Tennis Tournament 2002-2014 2 Events - Sports Marketing - Player Management by Anders Borg Tournament Director The Liverpool International tennis Tournament (LITT) was We have introduced over 60,000 children to tennis established in 2002 as a warm up event for Wimbledon through our School Programme during the Liverpool to give top ATP and WTA players as much grass court International. Moving forward we will work closely with practice as possible prior to the most important tennis Liverpool City Council to guide as many of the children tournament in the world. The event organisers Northern who attend the programme in the park into public tennis Vision has since 2002 gathered an incredible list of the clubs in Liverpool. world’s best players competing in Calderstones such as Novak Djorkovic, David Ferrer, Mardy Fish, Marat Safin, In addition to its academy programmes and clinics, Caroline Wozniacki, Laura Robson and Viktoria Azarenka Liverpool International has projects involving students, to mention a few. local businesses and charities, making it a very community oriented event . Our new partnership with the The Tournament added on legends to its program in title sponsor Liverpool Hope University, has added extra 2004 and has since hosted the three most famous tennis value to the tournament in terms of the promotion of legends of the Open era, Bjorn Borg, John McEnroe and Education, Sport, Health and Business Networking.W Martina Navratilova,as well as other legends including Martina Hingis, Ilie Nastase, Michael Stich, Richard Our relationship with Liverpool City Council is invaluable, Krajicek, former British Number One and US Open Finalist, but for this event to be sustainable and to add to the Greg Rusedski and the Iranian tennis trickster with the tourism economy of the city, it is important for the private unmistakable ‘tash’, Mansour Bahrami. -

2020 Women’S Tennis Association Media Guide
2020 Women’s Tennis Association Media Guide © Copyright WTA 2020 All Rights Reserved. No portion of this book may be reproduced - electronically, mechanically or by any other means, including photocopying- without the written permission of the Women’s Tennis Association (WTA). Compiled by the Women’s Tennis Association (WTA) Communications Department WTA CEO: Steve Simon Editor-in-Chief: Kevin Fischer Assistant Editors: Chase Altieri, Amy Binder, Jessica Culbreath, Ellie Emerson, Katie Gardner, Estelle LaPorte, Adam Lincoln, Alex Prior, Teyva Sammet, Catherine Sneddon, Bryan Shapiro, Chris Whitmore, Yanyan Xu Cover Design: Henrique Ruiz, Tim Smith, Michael Taylor, Allison Biggs Graphic Design: Provations Group, Nicholasville, KY, USA Contributors: Mike Anders, Danny Champagne, Evan Charles, Crystal Christian, Grace Dowling, Sophia Eden, Ellie Emerson,Kelly Frey, Anne Hartman, Jill Hausler, Pete Holtermann, Ashley Keber, Peachy Kellmeyer, Christopher Kronk, Courtney McBride, Courtney Nguyen, Joan Pennello, Neil Robinson, Kathleen Stroia Photography: Getty Images (AFP, Bongarts), Action Images, GEPA Pictures, Ron Angle, Michael Baz, Matt May, Pascal Ratthe, Art Seitz, Chris Smith, Red Photographic, adidas, WTA WTA Corporate Headquarters 100 Second Avenue South Suite 1100-S St. Petersburg, FL 33701 +1.727.895.5000 2 Table of Contents GENERAL INFORMATION Women’s Tennis Association Story . 4-5 WTA Organizational Structure . 6 Steve Simon - WTA CEO & Chairman . 7 WTA Executive Team & Senior Management . 8 WTA Media Information . 9 WTA Personnel . 10-11 WTA Player Development . 12-13 WTA Coach Initiatives . 14 CALENDAR & TOURNAMENTS 2020 WTA Calendar . 16-17 WTA Premier Mandatory Profiles . 18 WTA Premier 5 Profiles . 19 WTA Finals & WTA Elite Trophy . 20 WTA Premier Events . 22-23 WTA International Events . -

Partnership Proposal for the Biggest Tennis Exhibition in Europe
Partnership Proposal for the biggest Tennis Exhibition in Europe For more information please visit: www.northern-vision.co.uk www.liverpooltennis.co.uk by Anders Borg Liverpool Hope International Tennis Tournament Director Tournament 2002-2015 The Liverpool Hope International Tennis Tournament We have introduced over 60,000 children to tennis (LITT) was established in 2002 as a warm up event for through our School Programme during the Liverpool Wimbledon to give top ATP and WTA players as much International. Moving forward we will work closely with grass court practice as possible prior to the most Liverpool City Council to guide as many of the children important tennis tournament in the world. The event who attend the programme in the park into public tennis organisers Northern Vision has since 2002 gathered an clubs in Liverpool. incredible list of the world’s best players competing in Liverpool such as Novak Djorkovic, David Ferrer, Mardy In addition to our CSR program Liverpool International Fish, Marat Safin, Caroline Wozniacki, Laura Robson and has projects involving students, local businesses and Viktoria Azarenka to mention a few. charities, making it a very community oriented event . Our partnership with the title sponsor Liverpool Hope The Tournament added on legends to its program in University, has added extra value to the tournament in 2004 and has since hosted the three most famous tennis terms of the promotion of Education, Sport, Health and players of the Open era, Bjorn Borg, John McEnroe and Business Networking. Martina Navratilova,as well as Martina Hingis, Virgina Wade , Ilie Nastase, Michael Stich, Richard Krajicek, former Our relationship with Liverpool City Council is invaluable, British Number One and US Open Finalist, Greg Rusedski but for this event to be sustainable due to the austerity and the Iranian tennis trickster with the unmistakable faced by the public sector it is important for the private ‘tash’, Mansour Bahrami. -

EUGENIE BOUCHARD (CAN #272) Vs
MATCH NOTES ISTANBUL - TURKEY | Sep 08 - Sep 13, 2020 | $225,500 | INTERNATIONAL [Q] EUGENIE BOUCHARD (CAN #272) vs. PATRICIA MARIA TIG (ROU #88) Head to Head: First meeting EUGENIE BOUCHARD PATRICIA MARIA TIG 272 WTA RANKING 88 106 PORSCHE RACE TO SHENZHEN LEADERBOARD 103 25-02-1994 (26) DATE OF BIRTH (AGE) 27-07-1994 (26) $46,871 YTD PRIZE MONEY $39,547 $6,469,693 CAREER PRIZE MONEY $732,365 0 / 1 SINGLES TITLES (YTD / CAREER) 0 / 0 0 / 1 DOUBLES TITLES (YTD / CAREER) 0 / 0 4-0 ISTANBUL W-L (MD) * 4-0 YTD / CAREER W-L (MD) * 8-2 / 149-133 8-4 / 32-32 3-2 / 41-52 YTD / CAREER 3-SET W-L (MD) * 1-0 / 7-9 2-2 / 40-24 YTD / CAREER TIE-BREAK W-L (MD) * 1-0 / 9-3 6-1 / 41-25 YTD / CAREER CLAY W-L (MD) * 4-2 / 15-13 0-0 / 9-11 YTD / CAREER Left Hander W-L (MD) * 1-0 / 2-1 0-0 / 3-14 YTD / CAREER TOP 5 W-L (MD & Q) * 0-0 / 0-0 0-0 / 12-29 YTD / CAREER TOP 10 W-L (MD & Q) * 0-0 / 0-0 0-0 / 18-47 YTD / CAREER TOP 20 W-L (MD & Q) * 0-1 / 2-3 * Updated entering 2020 Istanbul final ROAD TO THE FINAL [Q] EUGENIE BOUCHARD (CAN #272) PATRICIA MARIA TIG (ROU #88) R2-Q: d. LEONIE KUNG (SUI #148) 6-4,6-4 (1h33) SF: d. TEREZA MARTINCOVA (CZE #136) 6-3,6-3 (1h49) R1-Q: d. -

Tournament Notes
TOURNAMENT NOTES as of September 17, 2015 2015 COLEMAN VISION TENNIS CHAMPIONSHIPS ALBUQUERQUE, NM • SEPTEMBER 20–27 USTA PRO CIRCUIT RETURNS TO ALBUQUERQUE TOURNAMENT INFORMATION The 2015 Coleman Vision Tennis Championships return to Albuquerque for Site: Tanoan Country Club – Albuquerque, N.M. the 18th consecutive year. It is the second event following the US Open and the only Websites: www.colemanvision.com USTA Pro Circuit tournament held in New procircuit.usta.com Dishman USTA/Ned Mexico this year. Facebook: Coleman Vision This tournament will be streamed live on Sunday, Sept. 20 Qualifying Draw Begins: www.procircuit.usta.com. Main Draw Begins: Tuesday, Sept. 22 To follow the tournament, download the Main Draw: 32 Singles / 16 Doubles USTA Pro Circuit’s new phone app by searching “procircuit” in the app store. Nicole Gibbs received a wild card into this Surface: Hard / Outdoor year’s US Open and won her first-round Prize Money: $75,000 match. Gibbs captured consecutive NCAA Notable players competing in the main draw singles titles in 2012 and 2013 for Stanford Tournament Director: include: University, becoming the fifth player in Sue Jollensten, (505) 822-1694 history—and the fourth from Stanford—to Nicole Gibbs, who earned a wild card into win back-to-back NCAA Division I women’s [email protected] singles championships. this year’s US Open and won her first-round Tournament Press Contact: match. Last year, Gibbs advanced to the Cee Ann Vaughan, (478) 973-4388 third round of the 2014 US Open—her in 2012, she defeated teammate Mallory [email protected] career-best result—while competing as Burdette in the NCAA singles title match USTA Communications Contact: a wild card after winning the USTA Pro and then teamed with Burdette to win the Amanda Korba, (914) 697-2219, [email protected] Circuit’s US Open Wild Card Challenge. -

BNP Paribas Open ORDER of PLAY - FRIDAY, 9 MARCH 2018
BNP Paribas Open ORDER OF PLAY - FRIDAY, 9 MARCH 2018 STADIUM 1 STADIUM 2 STADIUM 3 STADIUM 4 STADIUM 5 STADIUM 6 STADIUM 7 STADIUM 8 STADIUM 9 Starting At: 11:00 am Starting At: 11:00 am Starting At: 11:00 am Starting At: 11:00 am Starting At: 11:00 am Starting At: 11:00 am Starting At: 11:00 am Starting At: 11:00 am Starting At: 11:00 am ATP WTA ATP WTA ATP WTA WTA WTA WTA Andreja KLEPAC (SLO) Gael MONFILS (FRA) Petra KVITOVA (CZE) [9] [Q] Marcos BAGHDATIS (CYP) Johanna KONTA (GBR) [11] Mikhail YOUZHNY (RUS) Aryna SABALENKA (BLR) Samantha STOSUR (AUS) María José MARTÍNEZ SÁNCHEZ (ESP) [8] Elise MERTENS (BEL) [22] 1 vs vs vs vs vs vs vs vs vs Matthew EBDEN (AUS) Yulia PUTINTSEVA (KAZ) [PR] Yoshihito NISHIOKA (JPN) Marketa VONDROUSOVA (CZE) Joao SOUSA (POR) Svetlana KUZNETSOVA (RUS) [19] Kristina MLADENOVIC (FRA) [14] Kirsten FLIPKENS (BEL) Qiang WANG (CHN) Nina STOJANOVIC (SRB) followed by followed by followed by followed by followed by followed by followed by followed by followed by ATP WTA ATP ATP ATP WTA ATP WTA WTA [WC] Philipp PETZSCHNER (GER) Barbora KREJCIKOVA (CZE) Frances TIAFOE (USA) CoCo VANDEWEGHE (USA) [17] Viktor TROICKI (SRB) Pierre-Hugues HERBERT (FRA) Dominic THIEM (AUT) Naomi OSAKA (JPN) [Q] Yuki BHAMBRI (IND) Katerina SINIAKOVA (CZE) [6] Barbora STRYCOVA (CZE) [25] 2 vs vs vs vs vs vs vs vs vs [WC] Ernesto ESCOBEDO (USA) Kaia KANEPI (EST) Marton FUCSOVICS (HUN) Gilles SIMON (FRA) Jamie MURRAY (GBR) Agnieszka RADWANSKA (POL) [31] [Q] Nicolas MAHUT (FRA) Mihaela BUZARNESCU (ROU) Petra MARTIC (CRO) Bruno SOARES (BRA) -

2019 World Teamtennis Media Information
2019 World TeamTennis Media Information FACTS & FIGURES ..................................................................................................... 2 BROADCAST OUTLETS & HAWK-EYE LIVE ................................................................. 4 TEAM ROSTERS ......................................................................................................... 6 2019 WTT SCHEDULE ............................................................................................... 8 TEAM VENUES ........................................................................................................ 10 MORE ABOUT WORLD TEAMTENNIS ...................................................................... 11 Important Things To Know .................................................................................. 12 Innovations & Firsts ............................................................................................ 14 Milestones .......................................................................................................... 15 WTT FINALS & CHAMPIONS ................................................................................... 17 FACTS & FIGURES What: World TeamTennis showcases the best in professional tennis with the innovative team format co-founded by Billie Jean King in the 1970s. Recognized as the leader in professional team tennis competition, WTT features many of the world’s best players competing annually for the King Trophy, the league’s championship trophy named after King. 2019 Teams: New York -

Dubai Duty Free Tennis Championships ORDER of PLAY - MONDAY, 18 FEBRUARY 2019
Dubai Duty Free Tennis Championships ORDER OF PLAY - MONDAY, 18 FEBRUARY 2019 CENTRE COURT COURT 1 COURT 2 COURT 3 COURT 7 Starting at: 11:00 AM Starting at: 12:00 noon Starting at: 12:00 noon Starting at: 12:00 noon Starting at: 12:00 noon Ons JABEUR (TUN) vs Donna VEKIC (CRO) followed by Starting at: 12:00 noon Starting at: 12:00 noon Starting at: 12:00 noon Starting at: 12:00 noon Shuko AOYAMA (JPN) Nadiia KICHENOK (UKR) Julia GOERGES (GER) [13] Sofia KENIN (USA) Lidziya MAROZAVA (BLR) [LL] Dalila JAKUPOVIC (SLO) Veronika KUDERMETOVA (RUS) vs vs vs vs vs Alison RISKE (USA) Mihaela BUZARNESCU (ROU) Viktoria KUZMOVA (SVK) [Q] Zarina DIYAS (KAZ) [WC] Sarah Beth GREY (GBR) Ajla TOMLJANOVIC (AUS) Eden SILVA (GBR) followed by followed by followed by followed by after suitable rest Belinda BENCIC (SUI) [Q] Jennifer BRADY (USA) Katerina SINIAKOVA (CZE) Shuai ZHANG (CHN) Daria KASATKINA (RUS) vs vs vs vs Jelena OSTAPENKO (LAT) Petra MARTIC (CRO) Anett KONTAVEIT (EST) [15] Irina BARA (ROU) Dalila JAKUPOVIC (SLO) followed by followed by followed by followed by followed by after suitable rest after suitable rest after suitable rest Anna-Lena GROENEFELD (GER) Andreja KLEPAC (SLO) [Alt] Eugenie BOUCHARD (CAN) [Q] Lin ZHU (CHN) Barbora STRYCOVA (CZE) Demi SCHUURS (NED) [8] Saisai ZHENG (CHN) Sofia KENIN (USA) vs vs vs vs vs Elise MERTENS (BEL) [16] Carla SUÁREZ NAVARRO (ESP) Mihaela BUZARNESCU (ROU) Ons JABEUR (TUN) Abigail SPEARS (USA) Alicja ROSOLSKA (POL) Alison RISKE (USA) Zhaoxuan YANG (CHN) Not Before 7:00 pm Not Before 7:00 pm followed by -

Tournament Notes
TournamenT noTes as of march 26, 2015 THE WILDE LEXUS WOMEN’S USTA PRO CIRCUIT EVENT OSPREY, FL • MARCH 29-APRIL 5 USTA PRO CIRCUIT WOMEN’S TENNIS RETURNS TO OSPREY TournamenT InFormaTIon The Wilde Lexus Women’s USTA Pro Circuit Event will take place in Osprey for the Site: The Oaks Club – Osprey, Fla. seventh consecutive year. The event is the USOpen.org first $50,000 USTA Pro Circuit women’s Websites: www.theoaksclub.com event of the season and one of eight women’s procircuit.usta.com events taking place in Florida this year. The Facebook: 2015 Wilde Lexus Women’s tournament kicks off a series of clay-court USTA Pro Circuit Event events held in the lead-up to the French Open. In conjunction with USTA Player Development, Qualifying Draw Begins: Sunday, March 29 the USTA Pro Circuit continues to emphasize Main Draw Begins: Tuesday, March 31 the importance of increased training for younger players on clay. Main Draw: 32 Singles / 16 Doubles Surface: Clay / Outdoor This tournament will be streamed live on www.procircuit.usta.com. Prize Money: $50,000 Tournament Director: To follow the tournament, download the USTA Tom Whitten, (530) 515-0728 Pro Circuit’s new phone app by searching [email protected] “procircuit” in the app store. Tournament Press Contact: Notable players competing in the main draw Madison Brengle reached the fourth round of Susan Greene, (941) 882-2335 include: this year’s Australian Open and is currently [email protected] ranked a career-best No. 44 in the world. USTA Communications Contacts: Madison Brengle, who is ranked a career- high No. -

Rogers Cup Presented by National Bank ORDER of PLAY - TUESDAY, 8 AUGUST 2017
Rogers Cup presented by National Bank ORDER OF PLAY - TUESDAY, 8 AUGUST 2017 CENTRE COURT GRANDSTAND COURT 1 COURT 3 COURT 4 Starting at: 11:00 AM Starting at: 11:00 AM Starting at: 11:00 AM Starting at: 2:00 PM Starting at: 11:00 AM Julia GOERGES (GER) [Q] Sorana CIRSTEA (ROU) Oceane DODIN (FRA) Mirjana LUCIC-BARONI (CRO) 1 vs vs vs vs Catherine BELLIS (USA) Caroline GARCIA (FRA) [Q] Ashleigh BARTY (AUS) [LL] Magdalena RYBARIKOVA (SVK) Not Before 1:00 pm followed by followed by followed by [WC] Charlotte ROBILLARD-MILLETTE (CAN) [Q] Donna VEKIC (CRO) Shuai PENG (CHN) Elena VESNINA (RUS) [16] Carol ZHAO (CAN) 2 vs vs vs vs [WC] Eugenie BOUCHARD (CAN) Ekaterina MAKAROVA (RUS) Alison RISKE (USA) Ana KONJUH (CRO) Anastasija SEVASTOVA (LAT) followed by followed by followed by Starting at: 2:00 PM followed by TBA - After suitable rest TBA - After suitable rest [WC] Eugenie BOUCHARD (CAN) Anna-Lena GROENEFELD (GER) Ashleigh BARTY (AUS) Agnieszka RADWANSKA (POL) [10] Anastasia PAVLYUCHENKOVA (RUS) Karolina PLISKOVA (CZE) Kveta PESCHKE (CZE) [8] Casey DELLACQUA (AUS) [7] 3 vs vs vs vs vs CoCo VANDEWEGHE (USA) Alizé CORNET (FRA) Dominika CIBULKOVA (SVK) Nao HIBINO (JPN) Julia GOERGES (GER) Kirsten FLIPKENS (BEL) Alicja ROSOLSKA (POL) Olga SAVCHUK (UKR) Not Before 5:00 pm followed by Chia-Jung CHUANG (TPE) Elina SVITOLINA (UKR) [5] Renata VORACOVA (CZE) 4 vs vs Daria KASATKINA (RUS) Lucie HRADECKA (CZE) Katerina SINIAKOVA (CZE) [6] Not Before 7:00 pm followed by Timea BABOS (HUN) Barbora STRYCOVA (CZE) 5 vs vs [WC] Bianca ANDREESCU (CAN) Daria GAVRILOVA (AUS) followed by [Q] Ekaterina ALEXANDROVA (RUS) 6 vs Caroline WOZNIACKI (DEN) [6] Karl Hale 7 August 2017 at 20:11 Tony Cho Giulia Orlandi / Mariana Alves Tournament Director Order of Play released Referee WTA Supervisor ANY MATCH ON ANY COURT MAY BE MOVED Singles Lucky-Losers Sign-in Deadline : 10.30 MATCHES WILL BE OFFICIALLY CALLED BY THE REFEREE Doubles Alternates Sign-in Deadline : 11.30 CHECK FOR THE DESIGNATED MEETING POINT www.wtatennis.com | facebook.com/WTA | twitter.com/WTA | youtube.com/WTA. -

Teams by Year
World TeamTennis - teams by year 1974 LEAGUE CHAMPIONS: DENVER RACQUETS EASTERN DIVISION Atlantic Section Baltimore Banners: Byron Bertram, Don Candy, Bob Carmichael, Jimmy Connors, Ian Crookenden, Joyce Hume, Kathy Kuykendall, Jaidip Mukerjea, Audrey Morse, Betty Stove. Boston Lobsters: Pat Bostrom, Doug Crawford, Kerry Melville, Janet Newberry, Raz Reid, Francis Taylor, Roger Taylor, Ion Tiriac, Andrea Volkos, Stephan Warboys. New York Sets: Fiorella Bonicelli, Carol Graebner, Ceci Martinez, Sandy Mayer, Charlie Owens, Nikki Pilic, Manuel Santana, Gene Scott, Pam Teeguarden, Virginia Wade, Sharon Walsh. Philadelphia Freedoms: Julie Anthony, Brian Fairlie, Tory Fretz, Billie Jean King, Kathy Kuykendall, Buster Mottram, Fred Stolle. COACH: Billie Jean King Central Section Cleveland Nets: Peaches Bartkowicz, Laura DuPont, Clark Graebner, Nancy Gunter, Ray Moore, Cliff Richey, Pat Thomas, Winnie Wooldridge. Detroit Loves: Mary Ann Beattie, Rosie Casals, Phil Dent, Pat Faulkner, Kerry Harris, Butch Seewagen, Lendward Simpson, Allan Stone. Pittsburgh Triangles: Gerald Battrick, Laura DuPont, Isabel Fernandez, Vitas Gerulaitis, Evonne Goolagong, Peggy Michel, Ken Rosewall. COACH: Ken Rosewall Toronto/Buffalo Royals: Mike Estep, Ian Fletcher, Tom Okker, Jan O’Neill, Wendy Overton, Laura Rossouw. WESTERN DIVISION Gulf Plains Section Chicago Aces: Butch Buchholz, Barbara Downs, Sue Eastman, Marcie Louie, Ray Ruffels, Sue Stap, Graham Stilwell, Kim Warwick, Janet Young. Florida Flamingos: Mike Belkin, Maria Esther Bueno, Mark Cox, Cliff Drysdale, Lynn Epstein, Donna Fales, Frank Froehling, Donna Ganz, Bettyann Stuart. Houston EZ Riders: Bill Bowrey, Lesley Bowrey, Cynthia Doerner, Peter Doerner, Helen Gourlay- Cawley, Karen Krantzcke, Bob McKinley, John Newcombe, Dick Stockton. Minnesota Buckskins: Owen Davidson, Ann Hayden Jones, Bob Hewitt, Terry Holladay, Bill Lloyd, Mona Guerrant Wendy Turnbull.