Orbit, Eyelids, and Lacrimal System
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

MR Imaging of the Orbital Apex
J Korean Radiol Soc 2000;4 :26 9-0 6 1 6 MR Imaging of the Orbital Apex: An a to m y and Pat h o l o g y 1 Ho Kyu Lee, M.D., Chang Jin Kim, M.D.2, Hyosook Ahn, M.D.3, Ji Hoon Shin, M.D., Choong Gon Choi, M.D., Dae Chul Suh, M.D. The apex of the orbit is basically formed by the optic canal, the superior orbital fis- su r e , and their contents. Space-occupying lesions in this area can result in clinical d- eficits caused by compression of the optic nerve or extraocular muscles. Even vas c u l a r changes in the cavernous sinus can produce a direct mass effect and affect the orbit ap e x. When pathologic changes in this region is suspected, contrast-enhanced MR imaging with fat saturation is very useful. According to the anatomic regions from which the lesions arise, they can be classi- fied as belonging to one of five groups; lesions of the optic nerve-sheath complex, of the conal and intraconal spaces, of the extraconal space and bony orbit, of the cav- ernous sinus or diffuse. The characteristic MR findings of various orbital lesions will be described in this paper. Index words : Orbit, diseases Orbit, MR The apex of the orbit is a complex region which con- tains many nerves, vessels, soft tissues, and bony struc- Anatomy of the orbital apex tures such as the superior orbital fissure and the optic canal (1-3), and is likely to be involved in various dis- The orbital apex region consists of the optic nerve- eases (3). -

Extraocular Muscles Orbital Muscles
EXTRAOCULAR MUSCLES ORBITAL MUSCLES INTRA- EXTRA- OCULAR OCULAR CILIARY MUSCLES INVOLUNTARY VOLUNTARY 1.Superior tarsal muscle. 1.Levator Palpebrae Superioris 2.Inferior tarsal muscle 2.Superior rectus 3.Inferior rectus 4.Medial rectus 5.Lateral rectus 6.Superior oblique 7.Inferior oblique LEVATOR PALPEBRAE SUPERIORIOS Origin- Inferior surface of lesser wing of sphenoid. Insertion- Upper lamina (Voluntary) - Anterior surface of superior tarsus & skin of upper eyelid. Middle lamina (Involuntary) - Superior margin of superior tarsus. (Superior Tarsus Muscle / Muller muscle) Lower lamina (Involuntary) - Superior conjunctival fornix Nerve Supply :- Voluntary part – Oculomotor Nerve Involuntary part – Sympathetic ACTION :- Elevation of upper eye lid C/S :- Drooping of upper eyelid. Congenital ptosis due to localized myogenic dysgenesis Complete ptosis - Injury to occulomotor nerve. Partial ptosis - disruption of postganglionic sympathetic fibres from superior cervical sympathetic ganglion. Extra ocular Muscles : Origin Levator palpebrae superioris Superior Oblique Superior Rectus Lateral Rectus Medial Rectus Inferior Oblique Inferior Rectus RECTUS MUSCLES : ORIGIN • Arises from a common tendinous ring knows as ANNULUS OF ZINN • Common ring of connective tissue • Anterior to optic foramen • Forms a muscle cone Clinical Significance Retrobulbar neuritis ○ Origin of SUPERIOR AND MEDIAL RECTUS are closely attached to the dural sheath of the optic nerve, which leads to pain during upward & inward movements of the globe. Thyroid orbitopathy ○ Medial & Inf.rectus thicken. especially near the orbital apex - compression of the optic nerve as it enters the optic canal adjacent to the body of the sphenoid bone. Ophthalmoplegia ○ Proptosis occur due to muscle laxity. Medial Rectus Superior Rectus Origin :- Superior limb of the tendonous ring, and optic nerve sheath. -

T20 FUNCTIONAL UPPER EYELID BLEPHAROPLASTY Policy Author
Policy T20 Blepharoplasty THRESHOLD POLICY – T20 FUNCTIONAL UPPER EYELID BLEPHAROPLASTY Policy author: West Suffolk CCG and Ipswich and East Suffolk CCG, with support from Public Health Suffolk. Policy start date: January 2008 Subsequent reviews July 2012 September 2014 February 2017 Next review date: February 2020 1. Policy Summary 1.1 Blepharoplasty is considered a low priority treatment and will only be funded by Ipswich and East Suffolk CCG & West Suffolk CCG when the following criteria are met. It will not be funded for cosmetic reasons. 1.2 This policy doesn’t apply to anyone <19 years of age. 2. Eligibility Criteria 2.1 Upper eyelid blepharoplasty is considered medically necessary for the following indications: a) To repair defects predisposing to corneal or conjunctival irritation such as entropion or pseudotrichiasis. OR b) To treat periorbital sequelae of thyroid disease, nerve palsy, blepharochalasis, floppy eyelid syndrome and chronic inflammatory skin conditions. OR c) To relieve symptoms of blepharospasm or significant dermatitis on the upper eyelid caused by redundant tissue. OR d) Following skin grafting for eyelid reconstruction. OR e) At the same time as ptosis correction for the upper eyelid if the surplus skin is felt to be excess on lifting the ptotic eyelid 2.2 For all other individuals, the following criteria apply: a) Documented patient complaints of interference with vision or visual field related activities such as difficulty reading or driving due to upper eye lid skin drooping, looking through the eyelids or seeing the upper eye lid skin AND b) There is redundant skin overhanging the upper eye lid margin and resting on the eyelashes when gazing straight ahead AND S:\Clinical Quality\00 Chief Nursing Office\Clinical Oversight Group\POLICIES\T\Policies\T20 blepharoplasty\T20 Blepharoplasty E.docx 1 Policy T20 Blepharoplasty c) Supporting evidence from visual field testing that eyelids impinge on visual fields reducing field to 120° horizontally and/or 40° or less vertically. -

Inferior Rectus Paresis After Secondary Blepharoplasty
Br J Ophthalmol: first published as 10.1136/bjo.68.8.535 on 1 August 1984. Downloaded from British Journal of Ophthalmology, 1984, 68, 535-537 Inferior rectus paresis after secondary blepharoplasty EDUARDO ALFONSO, ANDREW J. LEVADA, AND JOHN T. FLYNN From the Bascom Palmer Eye Institute, Department of Ophthalmology, University ofMiami School ofMedicine, Miami, Florida, USA SUMMARY A 52-year-old woman underwent a secondary cosmetic blepharoplasty for repair of residual dermatochalasis. Afterthis procedure vertical diplopia was noted. Ultrasound examination and the findings at operation were consistent with trauma to the inferior rectus muscle. We present this as an additional complication of cosmetic blepharoplasty. Numerous complications ofblepharoplasty have been The patient was examined by an ophthalmologist reported. They include blindness, orbital and eyelid and observation was recommended. One year later haematoma, epiphora, ectropion, lagophthalmos, she was examined by a second ophthalmologist in ptosis, incision' complications, scar thickening, Munich. A left hypertropia of 260 and exotropia of incomplete or excessive removal of orbital fat, 12° were found, and both inferior recti were thought lacrimal gland injury, exposure keratitis, and corneal to be involved. The patient could fuse only in gaze up ulcer. '-" Disturbances of ocular motility are and left. On 21 October 1981 she underwent a 5 mm uncommon, but superior oblique palsy,2 inferior recession ofthe right superior rectus muscle combined oblique injury,- superior rectus incarceration in the with release of conjunctival scar inferiorly, myotomy to ofthe inferior rectus muscle, and insertion of a Teflon wound,4 and restriction secondary retrobulbar http://bjo.bmj.com/ haemorrhage5 have been reported. -

Whole Exome Sequencing Gene Package Vision Disorders, Version 6.1, 31-1-2020
Whole Exome Sequencing Gene package Vision disorders, version 6.1, 31-1-2020 Technical information DNA was enriched using Agilent SureSelect DNA + SureSelect OneSeq 300kb CNV Backbone + Human All Exon V7 capture and paired-end sequenced on the Illumina platform (outsourced). The aim is to obtain 10 Giga base pairs per exome with a mapped fraction of 0.99. The average coverage of the exome is ~50x. Duplicate and non-unique reads are excluded. Data are demultiplexed with bcl2fastq Conversion Software from Illumina. Reads are mapped to the genome using the BWA-MEM algorithm (reference: http://bio-bwa.sourceforge.net/). Variant detection is performed by the Genome Analysis Toolkit HaplotypeCaller (reference: http://www.broadinstitute.org/gatk/). The detected variants are filtered and annotated with Cartagenia software and classified with Alamut Visual. It is not excluded that pathogenic mutations are being missed using this technology. At this moment, there is not enough information about the sensitivity of this technique with respect to the detection of deletions and duplications of more than 5 nucleotides and of somatic mosaic mutations (all types of sequence changes). HGNC approved Phenotype description including OMIM phenotype ID(s) OMIM median depth % covered % covered % covered gene symbol gene ID >10x >20x >30x ABCA4 Cone-rod dystrophy 3, 604116 601691 94 100 100 97 Fundus flavimaculatus, 248200 {Macular degeneration, age-related, 2}, 153800 Retinal dystrophy, early-onset severe, 248200 Retinitis pigmentosa 19, 601718 Stargardt disease -

Policy 96018: Blepharoplasty, Blepharoptosis Repair, and Brow
Policy: 96018 Initial Effective Date: 11/22/1996 SUBJECT: Blepharoplasty, Blepharoptosis Repair, and Annual Review Date: 11/16/2020 Brow Ptosis Repair Last Revised Date: 11/16/2020 Prior approval is required for some or all procedure codes listed in this Corporate Medical Policy. Definition: The term blepharoplasty refers to a collection of surgical procedures that involve removal of redundant eyelid tissue (skin, muscle, and fat). Although the primary indication for blepharoplasty is to improve the eyelid appearance, redundant lax eyelid tissue (dermatochalasis) can obstruct the superior visual field and interfere with activities of daily living in some individuals. In these cases, blepharoplasty may be considered in order to produce functional improvement in vision. The pathophysiology of dermatochalasis has not been well described, but much of the process appears to involve skin changes associated with the aging process. Less commonly, systemic disorders such as Ehlers-Danlos syndrome may predispose patients to develop dermatochalasis at a younger age. Clinical manifestations are mainly cosmetic, but in severe cases eyelid tissue may obstruct the superior visual field. The most common symptoms include difficulty reading and loss of peripheral vision when driving. Blepharoplasty may help to improve function for patients with clinically significant dermatochalasis. Blepharochalasis is sometimes confused with dermatochalasis. Though similar in nomenclature, these two disorders are quite different in presentation and etiology. Blepharochalasis is a rare condition characterized by intermittent, recurrent eyelid edema, resulting in relaxation of the eyelid tissue and resultant atrophy. The lower eyelids are less commonly involved. Blepharochalasis typically presents in adolescence or young adulthood, with intermittent attacks that occur less commonly as the person ages. -

Eyelid Conjunctival Tumors
EYELID &CONJUNCTIVAL TUMORS PHOTOGRAPHIC ATLAS Dr. Olivier Galatoire Dr. Christine Levy-Gabriel Dr. Mathieu Zmuda EYELID & CONJUNCTIVAL TUMORS 4 EYELID & CONJUNCTIVAL TUMORS Dear readers, All rights of translation, adaptation, or reproduction by any means are reserved in all countries. The reproduction or representation, in whole or in part and by any means, of any of the pages published in the present book without the prior written consent of the publisher, is prohibited and illegal and would constitute an infringement. Only reproductions strictly reserved for the private use of the copier and not intended for collective use, and short analyses and quotations justified by the illustrative or scientific nature of the work in which they are incorporated, are authorized (Law of March 11, 1957 art. 40 and 41 and Criminal Code art. 425). EYELID & CONJUNCTIVAL TUMORS EYELID & CONJUNCTIVAL TUMORS 5 6 EYELID & CONJUNCTIVAL TUMORS Foreword Dr. Serge Morax I am honored to introduce this Photographic Atlas of palpebral and conjunctival tumors,which is the culmination of the close collaboration between Drs. Olivier Galatoire and Mathieu Zmuda of the A. de Rothschild Ophthalmological Foundation and Dr. Christine Levy-Gabriel of the Curie Institute. The subject is now of unquestionable importance and evidently of great interest to Ophthalmologists, whether they are orbital- palpebral specialists or not. Indeed, errors or delays in the diagnosis of tumor pathologies are relatively common and the consequences can be serious in the case of malignant tumors, especially carcinomas. Swift diagnosis and anatomopathological confirmation will lead to a treatment, discussed in multidisciplinary team meetings, ranging from surgery to radiotherapy. -

Involutional Type of Entropion in a Child with Cutis Laxa
1432 Br J Ophthalmol 2000;84:1432–1438 Br J Ophthalmol: first published as 10.1136/bjo.84.12.1432 on 1 December 2000. Downloaded from LETTERS TO THE EDITOR Involutional type of entropion in a child with cutis laxa EDITOR,—The diVuse elastic tissue disease called cutis laxa (CL) is a serious, even lethal systemic illness, involving not only the skin but connective tissues throughout the body.1 The skin hangs in loose folds, producing the appearance of premature ageing. Internal manifestations such as emphysema, ectasia of the aorta, and multiple hernias are usually present. We report a child with cutis laxa, who presented with an unusual ophthalmic mani- festation of the disease. CASE REPORT Our patient, who is nowa4yearoldboyand Figure 2 Eyelid tissue stained for elastic fibres showing marked granular degeneration of the elastic the third child to a normal first degree cousin fibres. Aldehyde-fuscin, ×400. couple, was noted to have redundant skin and a hoarse cry at the age of 3 months. Skin biopsy Surgical correction was carried out using a arrangements; hence the term “generalised was consistent with cutis laxa (elastin stain lateral tarsal strip in addition to two full elastolysis”. showed focal thickening of the elastic fibres thickness lid sutures. A small piece of resected Goltz and coworkers suggested an imbalance with tapered ends). His 7 month old sister was eyelid tissue was sent for pathological examina- between the circulating pancreatic elastase and also diagnosed as having cutis laxa at 3 months tion. its inhibitor (pancreatic elastase inhibiting sub- of age. Her ophthalmic examination revealed Staining for elastic tissue revealed marked stance, EIS), with a diminution of the latter in no abnormalities. -
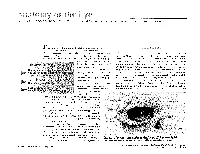
The Orbit Is Composed Anteri
DAVID L. PARVER, MD The University of Texas Southwestern Medical Center, Dallas Theability to successfully assess and treat The Orbit physical ailments requires an understanding of the anatomy involved in the injury or The eye itself lies within a protective shell trauma. When dealing with injuries and called the bony orbits. These bony cavities are trauma associated with the eye, it is neces- located on each side of the root of the nose. sary to have a work- Each orbit is structured like a pear with the ing knowledge of optic nerve, the nerve that carries visual im- basic ocular anatomy pulses from the retina to the brain, represent- so that an accurate ing the stem of the orbtt (Duke-Elder, 1976). Understa eye also diagnosis can be Seven bones make up the bony orbit: frontal, achieved and treat- zygomatic, maxillary, ethmoidal, sphenoid, ment can be imple- lacrimal, and palatine (Figures 1 and 2). in a bony " mented. The roof of the orbit is composed anteri- . .. The upcoming ar- orly of the orbital plate of the frontal bone ticles in this special and posteriorly by the lesser wing of the sphe- Each portion of the 01 I noid bone. The lateral wall is separated from .r. theme section the nervc an eye will deal specifically 2 with recognizing ocular illness, disease, and injuries, and will also address the incidence of sports related eye injuries and trauma. This paper covers the ba- sics of eye anatomy, focusing on the eye globe and its surrounding struc- tures. Once one gains an understand- ing of the normal anatomy of the eye, it will be easier to recognize trauma, injury, or illness. -

Eyelash Inversion in Epiblepharon: Is It Caused by Redundant Skin?
ORIGINAL RESEARCH Eyelash inversion in epiblepharon: Is it caused by redundant skin? Hirohiko Kakizaki1 Purpose: To evaluate the effect of redundant lower eyelid skin on the eyelash direction in Igal Leibovitch2 epiblepharon. Yasuhiro Takahashi3 Materials and methods: Asian patients with epiblepharon participated in this study. The Dinesh Selva4 lower eyelid skin was pulled downward in the upright position with the extent just to detach from eyelash roots, and the direction of the eyelashes was examined. These evaluations were 1Department of Ophthalmology, Aichi Medical University, Nagakute, repeated before surgery while the patients were lying supine under general anesthesia. Aichi 480-1195, Japan; 2Division of Results: The study included 41 lower eyelids of 25 patients (17 females, 8 males, average age; Oculoplastic and Orbital Surgery, 5.6 years, 16 cases bilateral, 9 unilateral). In the upright position, without downward traction Department of Ophthalmology, Tel-Aviv Medical Center, of the skin, the eyelashes were vertically positioned and touching the cornea. The redundant Tel-Aviv University, Tel-Aviv, Israel; skin touched only the eyelash roots and had minimal contribution to eyelash inversion. With 3 Department of Ophthalmology downward skin traction, there was no signifi cant change in the eyelash direction. In the spine and Visual Sciences, Osaka City University Graduate School position, the eyelashes were touching the cornea, and there was marked redundant skin that was of Medicine, Osaka 545-8585, Japan; pushing the eyelashes inward. With downward skin traction, there was no signifi cant change. 4 South Australian Institute Conclusions: The direction of lower eyelashes in patients with epiblepharon was less infl uenced of Ophthalmology and Discipline For personal use only. -

Original Article Anatomic Study of the Lacrimal Fossa and Lacrimal Pathway
Original Article Anatomic study of the lacrimal fossa and lacrimal pathway for bypass surgery with autogenous tissue grafting Hai Tao, Zhi‑zhong Ma1, Hai‑Yang Wu, Peng Wang, Cui Han Purpose: To study the microsurgical anatomy of the lacrimal drainage system and to provide anatomical Access this article online evidence for transnasal endoscopic lacrimal drainage system bypass surgery by autogenous tissue grafting. Website: Materials and Methods: A total of 20 Chinese adult cadaveric heads in 10% formaldehyde, comprising www.ijo.in 40 lacrimal ducts were used. The middle third section of the specimens were examined for the following DOI: features: the thickness of the lacrimal fossa at the anterior lacrimal crest, vertical middle line, and posterior 10.4103/0301-4738.121137 lacrimal crest; the cross section of the upper opening, middle part, and lower opening of the nasolacrimal PMID: canal; the horizontal, 30° oblique, and 45° oblique distances from the lacrimal caruncle to the nasal cavity; ***** the distance from the lacrimal caruncle to the upper opening of the nasolacrimal duct; and the included Quick Response Code: angle between the lacrimal caruncle–nasolacrimal duct upper opening junction and Aeby’s plane. Results: The middle third of the anterior lacrimal crest was significantly thicker than the vertical middle line and the posterior lacrimal crest (P > 0.05). The horizontal distance, 30° oblique distance, and 45° oblique distance from the lacrimal caruncle to the nasal cavity exhibited no significant differences (P > 0.05). The included angle between the lacrimal caruncle and the lateral wall middle point of the superior opening line of the nasolacrimal duct and Aeby’s plane was average (49.9° ± 1.8°). -

Evisceration, Enucleation and Exenteration
CHAPTER 10 EVISCERATION, ENUCLEATION AND EXENTERATION This chapter describes three operations that either remove the contents of the eye (evisceration), the eye itself (enucleation) or the whole orbital contents (exenteration). Each operation has specific indications which are important to understand. In many cultures the removal of an eye, even if blind, is resisted. If an eye is very painful or grossly disfigured an operation will be accepted more readily. However, if the eye looks normal the patient or their family may be very reluctant to accept its removal. Therefore tact, compassion and patience are needed when recommending these operations. ENUCLEATION AND EVISCERATION There are several reasons why either of these destructive operations may be necessary: 1. Malignant tumours in the eye. In the case of a malignant tumour or suspected malignant tumour the eye should be removed by enucleation and not evisceration.There are two important intraocular tumours, retinoblastoma and melanoma and for both of them the basic treatment is enucleation. Retinoblastoma is a relatively common tumour in early childhood. At first the growth is confined to the eye. Enucleation must be carried out at this stage and will probably save the child’s life. It is vital not to delay or postpone surgery. If a child under 6 has a blind eye and the possibility of a tumour cannot be ruled out, it is best to remove the eye. Always examine the other eye very carefully under anaesthetic as well. It may contain an early retinoblastoma which could be treatable and still save the eye. Retinoblastoma spreads along the optic nerve to the brain.