Alveolar Bone Grafting - a Summary of History and Current Literature on the Technique
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Análisis De La Morfología Dental En Escolares Afrocolombianos De Villa Rica, Cauca, Colombia
ANÁLISIS DE LA MORFOLOGÍA DENTAL EN ESCOLARES AFROCOLOMBIANOS DE VILLA RICA, CAUCA, COLOMBIA DENTAL MORPHOLOGY ANALYSIS OF AFRO-COLOMBIAN SCHOOLCHILDREN FROM VILLA RICA, CAUCA, COLOMBIA ISABELLA MARCOVICH1, ELIANA PRADO 1, PAOLA DÍAZ 1, YENNY ORTIZ 1, CARLOS MARTÍNEZ 2, FREDDY MORENO 3 RESUMEN. Introducción: el estudio de la morfología dental permite esclarecer el estado evolutivo (distancia biológica y grado de mestizaje) de una población, aportando información sobre los procesos etnohistóricos de las comunidades colombianas, dentro de los contextos antropológico, odontológico y forense. Métodos: estudio descriptivo transversal cuantitativo que caracterizó la morfología dental mediante el sistema Asudas (Arizona State University Dental Anthropology System) de trece rasgos morfológicos dentales coronales (winging, crowding, incisivos centrales y laterales en pala, doble pala, rasgo de Carabelli, reducción del hipocono, pliegue acodado, protostílido, patrón cuspídeo, número de cúspides, cúspides 6 y 7) observados en 116 modelos de yeso (59 mujeres y 57 hombres) de un grupo de escolares afrocolombianos del municipio de Villa Rica, departamento del Cauca. Resultados: se observaron frecuencias significativas del rasgo de Carabelli, configuración de los patrones cuspídeos X5 y X6 (LM1) y +4 y +5 (LM2), ausencia de reducción del hipocono, frecuencia relativa de la cúspide 7 y bajas frecuencias de incisivos en pala y doble pala. También, se puede afirmar que los Rasgos Morfológicos Dentales Coronales (RMDC) estudiados no presentan dimorfismo sexual y asimetría bilateral.Conclusiones: la muestra observada cuenta con una morfología dental propia de poblaciones que conforman el complejo dental caucasoide, sin embargo, es evidente la influencia de grupos regionales de origen mongoloide y la afinidad biológica con grupos regionales de mestizos caucasoides y de afrocolombianos. -

Research Article
s z Available online at http://www.journalcra.com INTERNATIONAL JOURNAL OF CURRENT RESEARCH International Journal of Current Research Vol. 12, Issue, 07, pp.12447-12456, July, 2020 DOI: https://doi.org/10.24941/ijcr.39159.07.2020 ISSN: 0975-833X RESEARCH ARTICLE DENTAL ANTHROPOLOGY –TODAY & TOMORROW (AN OVERVIEW) *Sonalee Shah Government Dental College, Raipur, Chhattisgarh, India ARTICLE INFO ABSTRACT Article History: Dental Anthropology is a scientific discipline, which deals with studies of sexual dimorphism, Received 21st April, 2020 paleodemography, oral health, lifestyle, evolutionary trends, paleodiet, biodistance and Received in revised form paleopathology through the analysis of the dentition of extinct and modern human populations and 30h May, 2020 hence, is concerned with the study of morphological variation (dental morphological features) and Accepted 07th June, 2020 metrics of the dentition of human populations over time (prehistoric and modern) and in space th Published online 28 July, 2020 (ie.ethnic influences) and their relation with the processes of adaptation and dietary changes that led to the evolution of the dental system and the human race.(1,3) Keeping in mind the dental Key Words: evolutionary changes, the subject experts, focus on the use of teeth to resolve anthropological Dental Anthropology, Tooth Weaar Patterns, problems. Teeth exhibit a wide array of variables, ranging from those largely controlled by genes to LEH, Non-Metric Tooth Traits, Forensic those largely dictated by environment. Dental variables under genetic control include crown and root Facial Approximation. morphology and size, along with tooth number (i.e., missing and extra teeth, or hypodontia and hyperdontia). Dental variables that reflect environmental factors include tooth crown wear and chipping, caries, abscesses, periodontal disease, calculus, and linear enamel hypoplasia. -

Oral Surgery TYPES of DENTAL FORCEPS the FORCEPS for UPPER TEETH 1- the Upper Straight Forceps:- the Blades, Joint and Handle Are in One Long Straight Line
Oral surgery TYPES OF DENTAL FORCEPS THE FORCEPS FOR UPPER TEETH 1- The upper straight forceps:- The blades, joint and handle are in one long straight line. We have two types, one with broad blades that is we call heavy blades and this is used for extraction of upper central incisors and upper canines, left and right. The second type of straight forceps has narrow blades or we call it fine blades for extraction of upper lateral incisors (left and right) and upper anterior retained roots. 2- The upper premolar forceps:- Here we have two bends in the design of the forceps, one where the beaks (blades) bend in relation to the joint of the forceps to apply the forceps parallel to long axis of premolar, the 2nd bend or curvature is of the handle to avoid injury to the lower lip and apposing teeth (mandibular). The upper premolars teeth has either one root or two roots (one buccal and one palatal), so there is no difference in the anatomy of the tooth root of the premolar on the buccal and palatal surface so the two blades of the premolars forceps are mirror image to each other. 3- The upper molar forceps (full crown upper molar forceps):- Since upper molar teeth have three roots, two buccal and one palatal, the blade of palatal side is round to conform or fit on palatal root, while blades on buccal has pointed tip or projection so it can enter or fit the bifurcation between the two buccal roots (mesial and distal) on the buccal side of the tooth. -

(Sus Scrofa Domesticus) Fernández Sánchez, J.M 1,3 DVM, Del Campo Velasco, M 1,3 DVM, Marín García,P 2 DVM, Phd and San Román Ascaso, F 3 MD DVM DDS Phd Diplevds
MORPHOLOGY OF THE DENTAL ARCADE IN ADULT PIGS (Sus scrofa domesticus) Fernández Sánchez, J.M 1,3 DVM, del Campo Velasco, M 1,3 DVM, Marín García,P 2 DVM, PhD and San Román Ascaso, F 3 MD DVM DDS PhD DiplEVDS. 1: Veterinary Clinic “ Río Duero”. Móstoles. Madrid.Spain 2: Morphology and Embriology Department. UCM. Madrid. Spain 3: Animal Pathology II Department of the Veterinary Clinical Hospital. UCM. Madrid. Spain INTRODUCTION The study of the dental arcade in adult pigs is very important due to its significance as an experimental animal in human odontology. This is due, among other causes, to the fact that, like humans, it is omnivorous and the premolar and molar teeth show many similar characteristics to human teeth and they suffer from common pathologies like periodontal disease or caries. The present work stands out because of its originality, since when doing a bibliographic search, we have not found any reference to pig species, where all the anatomical references, morphology, classification, descriptive elements and work model for dental arcades in adult pig are described in such a detailed way. MATERIAL AND METHODS In the present work six complete domestic pig crania with mandible were used; three of them corresponding to 3 to 4 year-old boars and three from 7 year-old culling sows. Upon the heads some references were taken in order to define some topographic planes and establish the concept of dental arcade. The aim was to study on all of them the common characteristics of the teeth, such as dentition, dental anatomy, occlusion, number and dental formula, teeth nomenclature and teeth replacement. -

Contents Focus on Dentistry September 18-20, 2011 Albuquerque, New Mexico
Contents Focus on Dentistry September 18-20, 2011 Albuquerque, New Mexico Thanks to sponsors Boehringer Ingelheim Vetmedica, Equine Specialties, Pfizer Animal Health, and Capps Manufacturing, Inc. for supporting the 2011 Focus on Dentistry Meeting. Sunday, September 18 Peridental Anatomy: Sinuses and Mastication Muscles ............................................... 1 Victor S. Cox, DVM, PhD Dental Anatomy .................................................................................................................8 P. M. Dixon, MVB, PhD, MRCVS Equine Periodontal Anatomy..........................................................................................25 Carsten Staszyk, Apl. Prof., Dr. med. vet. Oral and Dental Examination .........................................................................................28 Jack Easley, DVM, MS, Diplomate ABVP (Equine) How to Document a Dental Examination and Procedure Using a Dental Chart .......35 Stephen S. Galloway, DVM, FAVD Equine Dental Radiography............................................................................................50 Robert M. Baratt, DVM, MS, FAVD Beyond Radiographs: Advanced Imaging of Equine Dental Pathology .....................70 Jennifer E. Rawlinson, DVM, Diplomate American Veterinary Dental College Addressing Pain: Regional Nerve Blocks ......................................................................74 Jennifer E. Rawlinson, DVM, Diplomate American Veterinary Dental College Infraorbital Nerve Block Within the Pterygopalatine Fossa - EFBI-Technique -

Uncommon True Isolated Macrodontia of a Maxillary Tooth
JCDP Luciana Pereira et al 10.5005/jp-journals-10024-1499 CASE REPORT Uncommon True Isolated Macrodontia of a Maxillary Tooth 1Luciana Pereira, 2Priscila de Almeida Assunção, 3Sabrina Loren de Almeida Salazar, 4Fábio Ribeiro Guedes 5Aline Corrêa Abrahão, 6Márcia Grillo Cabral, 7Lucianne Cople Maia ABSTRACT The etiology of macrodontia is unknown, and the 4 Macrodontia is a rare dental anomaly which consists on the prevalence varies between 0.5 and 2.5%. It appears as a 3,4 presence of any tooth or teeth larger than the average. In dominant trait in some families. Isolated macrodontia may the present report the case of a child with an uncommon true affect premolars, permanent maxillary, mandibular incisors, isolated macrodontia of a maxillary central incisor is presented. and mandibular third molars in descending order, and there The maxillary left central incisor was considered a macrodontic is a higher prevalence in men than women.1,2 tooth since its mesiodistal crown dimension was 12.41 mm while the mesiodistal crown dimension of the maxillary right Macrodontia of anterior teeth causes problems of central incisor was 10.06 mm. The radiographic examination crowding, esthetics and plaque accumulation because of confirmed an enlarged maxillary left central incisor and a surface notching, and also additional problems of tooth inter- normal developing dentition. The patient did not report esthetic digitation and overjet reduction.2 Treatment is not necessary, complaints, however, due the presence of anterior open bite and crowding, he was referred to orthodontic clinic. Thus, it must unless for esthetic reasons, which requires special restorative 4 be point out the importance of the radiographic diagnosis to and orthodontic treatment planning. -

Maxillary Incisors of the Horse Before and at the Beginning of the Teeth Shedding: Radiographic and CT Study
animals Article Maxillary Incisors of the Horse before and at the Beginning of the Teeth Shedding: Radiographic and CT Study Francisco Miró 1,* , Carla Manso 2, Andrés Diz 1 and Manuel Novales 3 1 Department Comparative Anatomy and Pathology, University of Córdoba, Ctra. de Madrid, 14071 Córdoba Ctra, Spain; [email protected] 2 Veterinaries Specialist in Equine dentistry, Pedro Laín Entralgo 8, Boadilla del Monte, 28660 Madrid, Spain; [email protected] 3 Diagnostic Imaging Service, Veterinary Teaching Hospital, University of Córdoba, Ctra. de Madrid, 14071 Córdoba, Spain; [email protected] * Correspondence: [email protected]; Tel.: +34957218143 Received: 24 August 2020; Accepted: 31 August 2020; Published: 10 September 2020 Simple Summary: Although much is known about equine dentistry, there is a period of the horse’s life, prior to teeth shedding, in which there is lack of knowledge related to the development of deciduous incisors and dental germs of permanent incisors. To gain insight into the radiographic appearance of maxillary deciduous incisors and dental germs of maxillary permanent incisors during this period, a radiographic and computed tomography study of 25 horse skulls was made. Data regarding morphology and development were obtained. The results of the present study indicate that radiographic intraoral images are suitable to identify the grade of development of the dental germs of permanent incisors in horses before dental change. A detailed description of the radiographic appearance of deciduous incisors and dental germs of permanent incisors will help clinicians to expand their knowledge for diagnostic and treatment purposes. Abstract: To gain insight into the radiographic appearance of maxillary deciduous incisors and dental germs of maxillary permanent incisors in the period prior to teeth shedding, radiographs and computed tomography (CT) of 25 horse skulls, with an estimated age of between 12 and 42 months, were studied. -

Copyrighted Material
1 1 Oral Anatomy and Physiology Matthew Lemmons1 and Donald Beebe2 1 MedVet Medical and Cancer Centers for Pets, Indianapolis, IN, USA 2 Apex Dog and Cat Dentistry, Englewood, CO, USA Within this chapter, the dog will be discussed primarily, replacement is generally of a horizontal nature with although some comparative information will be covered. new teeth developing caudally and moving rostrally. Related anatomy and variations for other species will be In reptiles, the replacement is generally of a vertical discussed within chapters covering those. It is intended nature with new teeth developing immediately apical that this chapter serve to provide the foundation knowl to the teeth in current occlusion and replacing them edge for the chapters that follow. when lost. The practice of veterinary dentistry is concerned with Diphyodont. Two sets of teeth, one designated deciduous the conservation, reestablishment and/or treatment of and one permanent. Common to most domesticated dental, paradental, and oral structures. In dealing with animals and man. their associated problems a fundamental awareness of anatomy and physiology is essential for an understanding 1.1.2 Common Terms Used with Diphyodont of the presence or absence of the abnormal or pathologic Tooth Development structure. Anatomy and physiology are acutely interac tive, with anatomy considered the study of structure and Deciduous teeth (Dentes decidui). Considered to be the physiology that of its function. These deal with bones, first set of teeth that are shed at some point and muscles, vasculature, nerves, teeth, periodontium, replaced by permanent teeth. general oral functions, and their development. Primary teeth (Dentes primarui). -

Long Term Facial Alveolar Bone Changes Associated with Endosseous Implants in the Anterior Maxilla
University of Louisville ThinkIR: The University of Louisville's Institutional Repository Electronic Theses and Dissertations 5-2016 Long term facial alveolar bone changes associated with endosseous implants in the anterior maxilla. Deepika Joshi Follow this and additional works at: https://ir.library.louisville.edu/etd Part of the Oral Biology and Oral Pathology Commons Recommended Citation Joshi, Deepika, "Long term facial alveolar bone changes associated with endosseous implants in the anterior maxilla." (2016). Electronic Theses and Dissertations. Paper 2421. https://doi.org/10.18297/etd/2421 This Master's Thesis is brought to you for free and open access by ThinkIR: The University of Louisville's Institutional Repository. It has been accepted for inclusion in Electronic Theses and Dissertations by an authorized administrator of ThinkIR: The University of Louisville's Institutional Repository. This title appears here courtesy of the author, who has retained all other copyrights. For more information, please contact [email protected]. LONG TERM FACIAL ALVEOLAR BONE CHANGES ASSOCIATED WITH ENDOSSEOUS IMPLANTS IN THE ANTERIOR MAXILLA By Deepika Joshi University of Louisville, 2016 A Thesis Submitted to the Faculty of the University of Louisville School of Dentistry In Partial Fulfillment of the Requirements For the Degree of Master of Science in Oral Biology Oral Biology University of Louisville Louisville, Kentucky May 2016 LONG TERM FACIAL ALVEOLAR BONE CHANGES ASSOCIATED WITH ENDOSSEOUS IMPLANTS IN THE ANTERIOR MAXILLA By Deepika Joshi University of Louisville, 2016 A Thesis Approved on April 21, 2016 By the following Thesis Committee: ________________ Dr. William C. Scarfe, Thesis Director Dr.Bruno de Azevedo, Thesis Co-Director Dr. -
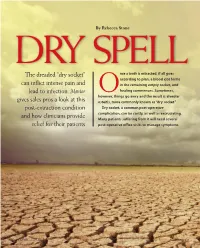
The Dreaded “Dry Socket”
By Rebecca Stone DRY SPELL The dreaded “dry socket” nce a tooth is ex tracted, if all goes according to plan, a blood clot forms can inflict intense pain and in the remaining empty socket, and lead to infection. Mentor Ohealing commences. Sometimes, however, things go awry and the result is alveolar gives sales pros a look at this osteitis, more commonly known as “dry socket.” post-extraction condition Dry socket, a common post-operative and how clinicians provide complication, can be costly, as well as excruciating. Many patients suffering from it will need several relief for their patients post-operative office visits to manage symptoms. 12 MENTOR MentorIsSalesPower.com NOVEMBER 2015 NOVEMBER 2015 MentorIsSalesPower.com MENTOR 13 To understand this condition, account executives might want to There are two kinds of extractions. Simple extraction involves brush up on their tooth anatomy. The socket, in which a tooth’s roots pulling erupted teeth by elevating them from the alveolus. Surgical reside, is more formally known as the dental alveolus. This is lined extraction must be performed with impacted teeth, such as unerupted with the periodontal ligament (PDL), which is composed of fibrous tis - wisdom teeth, or those with complications such as missing crowns and sue that connects to the cementum of the tooth and to the alveolar fractures. This involves the cutting of tissue and the need to dig the bone. The PDL overlays the lamina dura, a thin lining of bone, which tooth out, which can be traumatic. in turn overlays the more cancellous, or spongy, alveolar bone. One reason traumatic surgical extractions are said to have a greater Together, these structures support and retain the tooth. -

GPT-9 the Academy of Prosthodontics the Academy of Prosthodontics Foundation
THE GLOSSARY OF PROSTHODONTIC TERMS Ninth Edition GPT-9 The Academy of Prosthodontics The Academy of Prosthodontics Foundation Editorial Staff Glossary of Prosthodontic Terms Committee of the Academy of Prosthodontics Keith J. Ferro, Editor and Chairman, Glossary of Prosthodontic Terms Committee Steven M. Morgano, Copy Editor Carl F. Driscoll, Martin A. Freilich, Albert D. Guckes, Kent L. Knoernschild and Thomas J. McGarry, Members, Glossary of Prosthodontic Terms Committee PREFACE TO THE NINTH EDITION prosthodontic organizations regardless of geographic location or political affiliations. Acknowledgments are recognized by many of “The difference between the right word and the almost right the Academy fellowship, too many to name individually, with word is the difference between lightning and a lightning bug.” whom we have consulted for expert opinion. Also recognized are dMark Twain Gary Goldstein, Charles Goodacre, Albert Guckes, Steven Mor- I live down the street from Samuel Clemens’ (aka Mark Twain) gano, Stephen Rosenstiel, Clifford VanBlarcom, and Jonathan home in Hartford, Connecticut. I refer to his quotation because he Wiens for their contributions to the Glossary, which have spanned is a notable author who wrote with familiarity about our spoken many decades. We thank them for guiding us in this monumental language. Sometimes these spoken words are objectionable and project and teaching us the objectiveness and the standards for more appropriate words have evolved over time. The editors of the evidence-based dentistry to be passed on to the next generation of ninth edition of the Glossary of Prosthodontic Terms ensured that the dentists. spoken vernacular is represented, although it may be nonstandard in formal circumstances. -

Using CT Scans to Describe an Allosaurus Skull (Dinosauria: Theropoda) Jordan C
Cedarville University DigitalCommons@Cedarville The Research and Scholarship Symposium The 2019 yS mposium Apr 3rd, 11:00 AM - 2:00 PM Using CT Scans to Describe an Allosaurus Skull (Dinosauria: Theropoda) Jordan C. Oldham Cedarville University, [email protected] Follow this and additional works at: https://digitalcommons.cedarville.edu/ research_scholarship_symposium Part of the Animal Structures Commons, Paleobiology Commons, and the Paleontology Commons Oldham, Jordan C., "Using CT Scans to Describe an Allosaurus Skull (Dinosauria: Theropoda)" (2019). The Research and Scholarship Symposium. 7. https://digitalcommons.cedarville.edu/research_scholarship_symposium/2019/poster_presentations/7 This Poster is brought to you for free and open access by DigitalCommons@Cedarville, a service of the Centennial Library. It has been accepted for inclusion in The Research and Scholarship Symposium by an authorized administrator of DigitalCommons@Cedarville. For more information, please contact [email protected]. Using CT Scans to Describe an Allosaurus Skull (Dinosauria: Theropoda) Jordan Oldham: [email protected] Cedarville University Department of Science and Mathematics 251 North Main Street Cedarville, OH 45341 Abstract In 2001, an Allosaurus skull (CMP 279) was discovered in the Skull Creek Basin in Moffat County, Colorado. The skull is one of the most complete for the species and even contains the hyoid bones, which are usually not present. The skull is now permanently mounted, for display purposes, thus making the study of the individual bones difficult for producing a paleo-anatomical description. Computed Tomography (CT) scans of CMP 279 were created in 2017 and then made available for this study in 2019. CT scans are being used to investigate internal anatomy of skulls such as the endocranial cavity, sinuses, or foramina for nerve endings.