Impact of Non-Eligible Person Deliveries in Obstetric Service in Hong Kong
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Autumn Issue, November 2003
Newsletter Autumn Issue, November 2003 Official Publication of Hong Kong College of Radiologists President’s Jottings Dr. Lilian Leong IN THIS ISSUE President’s Some of us had been engaging during the last few weeks and weekends in activities Jottings…………....1 relating to radiology or our College’s events. We had our Fellowship Part II examination, AGM………………3 our Annual Scientific meetings, the Ho Hung Chiu Lecture delivered by Prof. TSUI Lap Chee and our trip to Guangzhou, to participate in the 11th Annual Scientific Congress of ASM………….……3 Chinese Radiological Society (CCR). For our ASM, we had the highest number of Joint Admission registrants this year, reaching almost 500. Some overseas participants got the information Ceremony and H.C. Ho Lecture…….…5 from our website. They gave us the feedback that we should promote our ASM energetically as there could be a lot of overseas Chinese and non-Chinese professionals Exam Result…......7 interested to take a trip to Hong Kong and to attend some professional meetings. We also FRCR Exam had enthusiastic submissions of proffered papers and posters, more than last year. For our Schedule………......8 delegation to CCR, we had supported almost 20 delegates. It was the “largest” delegation Part 2 Fellowship so far, and we had put up scientific posters for the occasion. Course …………....8 CME ……………....9 11th CCR…………10 I had attended the CCR a number of times and I appreciate the rapid evolution of this PET……………....12 annual function of Chinese Radiological Society. This year, the participants reached almost 2000. There were seven parallel sessions, large number of electronic CME CIRSE ……….....13 demonstration and enthusiastic participation in lectures delivered in English. -

New Territories East Cluster Report 2012/13
1 TABLE OF CONTENTS Hospital Authority Vision, Mission and Values ........................................................................ 5 Message from CCE .................................................................................................................... 6 Messages from HCEs & DHCE ............................................................................................... 8 I. Overview of Cluster Performance ................................................................................ 10 II. Cluster Governance & Organization ........................................................................... 12 III. Key Achievements of Targets 2012/13 A. Allay Staff Shortage and High Turnover .................................................................... 16 B. Better Manage Growing Service Demand ................................................................... 16 C. Ensure Service Quality and Safety ............................................................................ 18 D. Enhance Partnership with Patients and Community .................................................. 20 E. Ensure Adequate Resources for Meeting Service Needs ............................................ 20 IV. Key Achievements of Cluster Functions 2012/13 A. Administrative Services ............................................................................................. 22 B. Communications ....................................................................................................... 25 C. Finance ................................................................................................................... -

North District Hospital Announces a Nurse Tested Preliminarily Positive to COVID-19
North District Hospital announces a nurse tested preliminarily positive to COVID-19 The following is issued on behalf of the Hospital Authority: The spokesperson for the North District Hospital made the following announcement today (January 20) regarding a nurse tested preliminarily positive to COVID-19: A nurse in the medical department started experiencing mild malaise on January 18. She attended a community testing centre for COVID-19 viral test yesterday (January 19) and was notified today that she has tested preliminary positive. She is now being treated under isolation at the Prince of Wales Hospital in stable condition. The nurse had worked in the isolation ward recently. Her daily clinical duties included taking care of COVID-19 patients and she had been wearing appropriate personal protective equipment during work. Her last date of duty was January 14. The hospital infection control team is working with the Centre for Health Protection (CHP) on contact tracing. Four nurses in the medical department who have had social gathering with the confirmed nurse in recent days are classified as close contact and quarantine will be arranged. They have all undergone COVID-19 tests and the results are pending. As the nurse has been wearing appropriate personal protective equipment during work, no patient is classified as close contact. As a precautionary measure, viral tests and medical surveillance are being arranged for relevant staff in the isolation ward and the department of medicine. Thorough cleansing and disinfection of the areas where the nurse has worked and rested has been arranged. The hospital will continue to closely monitor the health condition of the concerned staff members and communicate with the CHP on the latest situation. -

HA Go Activation Location
HA Go Activation Location Region Hospital Counter G/F, Block A Grantham Hospital G/F, Kwok Tak Seng Heart Centre G/F, Lo Fong Shiu Po Eye Centre MacLehose Medical 2/F, Specialist Out-Patient Clinic Rehabilitation Centre Registration Office, Department of Clinical Oncology (Out-Patient Clinic), LG1/F, East Block Pamela Youde Nethersole J7, Psychiatric Out-Patient Department, 7/F, East Block Eastern Hospital Central Registration Centre, G/F, Specialist Out-Patient Block J2, Psychiatric Specialist Out-Patient Clinic J5, Child & Adolescent Psychiatric Day Centre 3/F, Block S 4/F, Block S Queen Mary Hospital 5/F, Block S Hong 6/F, Block S Kong 7/F, Block S Island 3/F, South Wing, David Trench Rehabilitation Centre Registration Counter, G/F, Specialist Out-Patient Ruttonjee Hospital Department The Duchess of Kent Children's Hospital at Specialist Out-Patient Clinic, G/F, A Block Sandy Bay Registration Counter, Specalist Out-Patient Clinic, G/F, Tung Wah Eastern Main Block Hospital Counter, Eye Clinic, G/F, TWGHs Lo Ka Chow Memorial Ophthalmic Centre Tung Wah Group of Hospitals Fung Yiu King Geriatric Day Hospital Hospital C5, Day Centre Tung Wah Hospital H3, Specialist Out-Patient Clinic L4, Eye, Nose & Throat Centre Tsan Yuk Hospital G/F, The Specialist Outpatient Clinic (Obstetrics) 1 / 4 HA Go Activation Location Region Hospital Counter Room 37, Ophthalmic Centre, 2/F, Wai Ming Block Caritas Medical Centre Specialist Out-Patient Clinic, 3/F, Wai Ming Block Reception Office, 4/F, Wai Ming Block Hong Kong Buddhist Enquiry counter, Out-Patient -

Survival Analysis of Patients with Breast Cancer
ANTICANCER RESEARCH 37 : 5813-5820 (2017) doi:10.21873/anticanres.12024 Survival Analysis of Patients with Breast Cancer Undergoing a Modified Radical Mastectomy With or Without a Thoracic Paravertebral Block: a 5-Year Follow-up of a Randomized Controlled Trial MANOJ KUMAR KARMAKAR 1, WINNIE SAMY 1, ANNA LEE 1, JIA WEI LI 1, WING CHEONG CHAN 2, PHOON PING CHEN 3 and BAN C.H. TSUI 4 1Department of Anesthesia and Intensive Care, The Chinese University of Hong Kong, Prince of Wales Hospital, Shatin, Hong Kong, P.R. China; 2Department of Surgery, North District Hospital, Sheung Shui, New Territories, Hong Kong, P.R. China; 3Departments of Anesthesiology and Operating Services, North District Hospital, Sheung Shui, New Territories, Hong Kong, P.R. China; 4Department of Anesthesiology, Perioperative and Pain Medicine, Stanford University School of Medicine, Stanford, CA, U.S.A. Abstract. Aim: This 5-year prospective follow-up of women nor from that with GA plus c-TPVB (HR=0.79, 95% CI=0.21- randomized to general anesthesia (GA) with or without a 2.96) (p=0.88). Compared to the GA-only group, the risk of thoracic paravertebral block (TPVB) examined the risk of mortality was similarly not different from that of the two other local recurrence, metastasis and mortality after breast cancer groups (HR=2.57, 95% CI=0.66-9.92; and HR=0.66, 95% surgery. Patients and Methods: A total of 180 patients CI=0.11-3.97, respectively, p=0.15). Conclusion: Although undergoing modified radical mastectomy were randomized to the original study was underpowered to properly address one of three study groups: standardized GA only; GA with a long-term outcomes, the results of this analysis suggest that single-injection TPVB (s-TPVB) and placebo paravertebral TPVB, administered whether as a single-injection or infusion after surgery for 72-h; and GA plus with continuous continuous infusion during the perioperative period, had little TPVB (c-TPVB) for 72-h postoperatively. -

A General Brief About the Hospital Authority
Mission Statement 4. In keeping with its role, the Mission of the Hospital Authority is: · to meet the different needs of patients for public hospital services, and to improve the hospital environment for the benefit of patients; · to serve the public with care, dedication and efficiency, and to encourage community participation in the system, resulting in better care and more direct accountability to the public; · to provide rewarding, fair and challenging employment to all its staff, in an environment conducive to attracting, motivating and retaining well-qualified staff; · to advise the Government of the needs of the community for public hospital services and of the resources required to meet these needs, in order to provide adequate, efficient, effective and value for money public hospital services of the highest standards recognised internationally within the resources obtainable; and · to collaborate with other agencies and bodies in the healthcare and related fields both locally and overseas to provide the greatest benefit to the local community. Corporate Vision and Strategies 5. To realise its mission, the Hospital Authority has developed the following Corporate Vision: “The Hospital Authority will collaborate with other healthcare providers and carers in the community to create a seamless healthcare environment which will maximise healthcare benefits and meet community expectations.” 6. The Authority achieves this corporate vision by formulating a set of strategic directions every year through an extensive annual planning process, taking into account the funding position, societal expectations, Government’s healthcare policy, and the challenges in the internal and external environment. The 2 corporate vision and mission are turned into operational targets to meet the community needs for healthcare services. -

Birth Record
eHR Sharable Data - Birth Record May 2018 © HKSAR Government eHR Sharable Data - Birth Record Form Category 1 Entity Name Entity ID Definition Data Type Data Type Validation Rule Repeated Code Table Remark Data requirement Data requirement Data requirement Example (Certified Example (Certified Example (Certified (code) (description) Data (Certified Level 1) (Certified Level 2) (Certified Level 3) Level 1) Level 2) Level 3) Birth Birth datetime 100310 The birth date or birth datetime of a patient TS Time stamp M M M 11/02/2012 20/12/2011 21:22 09/12/2001 23:59 Record Birth Birth Birth institution code 1003346 [eHR value] of the "Birth institution" code table, to define CE Coded Birth institution NA NA M PMH Record Institution the healthcare institution who reported the birth data to element the Immigration Department Birth Birth Birth institution description 1003107 [eHR description] of the "Birth institution" code table, it ST String Birth institution NA NA M Princess Margaret Record Institution should be the corresponding description of the selected Hospital [Birth institution code]. Birth institution description is to define the healthcare institution who reported the birth data to the Immigration Department. Birth Birth Birth institution local description 1003108 The local description of the healthcare institution who ST String M M M St. Paul Hospital St. Paul Hospital Princess Margaret Record Institution reported the birth data to the Immigration Department. Hospital Birth Birth Birth location code 1003102 [eHR value] of the "Birth location" code table, to define CE Coded Birth location NA NA O BBA Record Location the location where the patient was born element Birth Birth Birth location description 1003103 [eHR description] of the "Birth location" code table, it ST String Birth location NA NA M if [Birth location code] Born before arrival Record Location should be the corresponding description of the selected is given [Birth location code]. -

Prospective Assessment of the Hong Kong Hospital Authority Universal
Prospective assessment of the Hong Kong Hospital ORIGINAL ARTICLE Authority universal Down syndrome screening programme Daljit S Sahota 邵浩達 WC Leung 梁永昌 Objective To evaluate the performance of the locally developed universal WP Chan 陳運鵬 Down syndrome screening programme. William WK To 杜榮基 Elizabeth T Lau 劉嚴德光 Design Population-based cohort study in the period July 2010 to June 2011 inclusive. TY Leung 梁德楊 Setting Four Hong Kong Hospital Authority Departments of Obstetrics and Gynaecology and a central university-based laboratory for maternal serum processing and risk determination. Participants Women were offered either a first-trimester combined test (nuchal translucency, free beta human chorionic gonadotropin, and pregnancy-associated plasma protein-A) or nuchal- translucency-only test, or a second-trimester double test (alpha-fetoprotein and total human chorionic gonadotropin) for detection of Down syndrome according to their gestational age. Those with a trisomy 21 term risk of 1:250 or higher were offered a diagnostic test. Results A total of 16 205 pregnancies were screened of which 13 331 (82.3%) had a first-trimester combined test, 125 (0.8%) had a nuchal-translucency test only, and 2749 (17.0%) had a second- trimester double test. There were 38 pregnancies affected by Down syndrome. The first-trimester screening tests had a 91.2% (31/34) detection rate with a screen-positive rate of 5.1% (690/13 Key words 456). The second-trimester test had a 100% (4/4) detection rate Down syndrome; First trimester with a screen-positive rate of 6.3% (172/2749). There were screening; Second trimester screening; seven (0.9%) pregnancies that miscarried following an invasive Nuchal translucency; Quality control diagnostic test. -
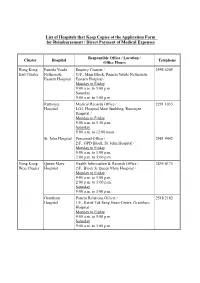
List of Hospitals That Keep Copies of the Application Form for Reimbursement / Direct Payment of Medical Expenses
List of Hospitals that Keep Copies of the Application Form for Reimbursement / Direct Payment of Medical Expenses Responsible Office / Location / Cluster Hospital Telephone Office Hours Hong Kong Pamela Youde Enquiry Counter / 2595 6205 East Cluster Nethersole G/F., Main Block, Pamela Youde Nethersole Eastern Hospital Eastern Hospital / Monday to Friday 9:00 a.m. to 5:00 p.m. Saturday 9:00 a.m. to 1:00 p.m. Ruttonjee Medical Records Office / 2291 1035 Hospital LG1, Hospital Main Building, Ruttonjee Hospital / Monday to Friday 9:00 a.m. to 5:30 p.m. Saturday 9:00 a.m. to 12:00 noon St. John Hospital Personnel Office / 2981 9442 2/F., OPD Block, St. John Hospital / Monday to Friday 9:00 a.m. to 1:00 p.m. 2:00 p.m. to 5:00 p.m. Hong Kong Queen Mary Health Information & Records Office / 2855 4175 West Cluster Hospital 2/F., Block S, Queen Mary Hospital / Monday to Friday 9:00 a.m. to 1:00 p.m. 2:00 p.m. to 5:00 p.m. Saturday 9:00 a.m. to 1:00 p.m. Grantham Patient Relations Officer / 2518 2182 Hospital 1/F., Kwok Tak Seng Heart Centre, Grantham Hospital / Monday to Friday 9:00 a.m. to 5:00 p.m. Saturday 9:00 a.m. to 1:00 p.m. - 2 - Responsible Office / Location / Cluster Hospital Telephone Office Hours Kowloon Kwong Wah Medical Report Office / 3517 5216 West Cluster Hospital 1/F., Central Stack, Kwong Wah Hospital / Monday to Friday 9:00 a.m. -

Department of Anesthesia University of Toronto Annual Report 2005
DEPARTMENT OF ANESTHESIA UNIVERSITY OF TORONTO ANNUAL REPORT 2005 – 2006 http://www.anesthesia.utoronto.ca 150 College Street Room 121 Fitzgerald Building Toronto, Ontario M5S 3E2 UNIVERSITY OF TORONTO – DEPARTMENT OF ANESTHESIA TABLE OF CONTENTS Message from the Chair ..................................................................................................................................................... 1 Anesthesia Fellows (2005-2006) ...................................................................................................................................... 3 Awards and Achievements ................................................................................................................................................ 4 Department Council ........................................................................................................................................................... 7 Undergraduate Education Committee ........................................................................................................................... 8 Postgraduate Education Committee ............................................................................................................................... 12 Anesthesia Residents (2005-2006) .................................................................................................................................. 14 U of T Fellowship Research Seminar Series ................................................................................................................. -

List of Medical Social Services Units Under Social Welfare Department
List of Medical Social Services Units Under Social Welfare Department Hong Kong Name of Hospital/Clinic Tel. No. Email Address 1. Queen Mary Hospital 2255 3762 [email protected] 2255 3764 2. Wong Chuk Hang Hospital 2873 7201 [email protected] 3. Pamela Youde Nethersole Eastern 2595 6262 [email protected] Hospital 4. Pamela Youde Nethersole Eastern 2595 6773 [email protected] Hospital (Psychiatric Department) Kowloon Name of Hospital/Clinic Tel. No. Email Address 5. Tseung Kwan O Hospital 2208 0335 [email protected] 2208 0327 6. United Christian Hospital 3949 5178 [email protected] (Psychiatry) 7. Queen Elizabeth Hospital 3506 7021 [email protected] 3506 7027 3506 5499 3506 4021 8. Hong Kong Eye Hospital 2762 3069 [email protected] 9. Kowloon Hospital Rehabilitation 3129 7857 [email protected] Building 10. Kowloon Hospital 3129 6193 [email protected] 11. Kowloon Hospital 2768 8534 [email protected] (Psychiatric Department) 1 The New Territories Name of Hospital/Clinic Tel. No. Email Address 12. Prince of Wales Hospital 3505 2400 [email protected] 13. Shatin Hospital 3919 7521 [email protected] 14. Tai Po Hospital 2607 6304 [email protected] Sub-office Tai Po Hospital (Child and Adolescent 2689 2486 [email protected] Mental Health Centre) 15. North District Hospital 2683 7750 [email protected] 16. Tin Shui Wai Hospital 3513 5391 [email protected] 17. Castle Peak Hospital 2456 7401 [email protected] 18. Siu Lam Hospital 2456 7186 [email protected] 19. -

Hospital Authority's Planned Projects for 2021-2022
LC Paper No. CB(4)503/20-21(02) Head 708 Subhead 8083MM One-Off Grant to the Hospital Authority for Minor Works Projects 2021-22 Planned Projects Prepared by the Hospital Authority February 2021 Head 708 : Subhead 8083MM One-off Grant to the Hospital Authority for Minor Works Projects for the 2019-20 Financial Year Part A - Previously approved items and other items to commence in 2020-21 with expected expenditure in 2020-21 and/or 2021-22 Actual Approved Cumulative Revised Estimated cash flow in subsequent years Expenditure Estimate Priority / Project Expenditure Estimate Project Title (1.4.2020 to 2021-22 Post Item No. Estimate to 31.3.2020 2020-21 31.10.2020) 2022-23 2023-24 2024-25 2024-25 ($'000) (I) Previously approved items (up to 31.10.2020) with expected expenditure in 2020-21 and/or 2021-22 EMR15-604 Modernisation of lifts in Day Treatment Block and Special Block in Prince of Wales Hospital 16,794 16,540 254 254 - - - - - EMR16-104 Replacement of the local central control and monitoring system for Wong Chuk Hang Hospital 1,280 1,150 39 101 - 30 - - - EMR16-401 Replacement of fire alarm and detection system at Hospital Main Block in Tseung Kwan O 6,500 6,500 (1,371) (1,371) - - - - - Hospital EMR16-504 Replacement of 1 no. main switch board for Block A in Yan Chai Hospital 2,345 2,202 142 142 - - - - - EMR16-505 Replacement of building management system at Multi Services Complex in Yan Chai Hospital 3,500 3,148 55 55 297 - - - - EMR16-506 Replacement of the air handling unit for Department of Central Supporting Services at 1/F, 502 526 (24) (24) - - - - - Block B in Yan Chai Hospital EMR17-102 Replacement of emergency generators for Hospital Block at St.