Amal Chandra Kataki 1 , Malcolm J. Simons 2,3 , Ashok Kumar Das 4
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

2016 03 28 B M.Pdf
file:///C:/Users/Neeraj/Desktop/html/2016_03_28_b_m.htm N O T E ----------------------- ALL ORDINARY MOTION CASES HAVING ADJOURNMENT DATES FROM 23.03.2016 TO 27.03.2016 HAS BEEN SHIFTED TO 28.03.2016 AND FOR THE SAME KINDLY SEE ORDINARY MOTION LIST OF 28.03.2016. ALL CONCERNED TO PLEASE NOTE. ------------------------------------------------------------------------------------------------------ NOTICE ----------------------- It is for the information of all the Advocates/Litigants that as per the decision of Hon'ble Committee, persons belonging to Schedule Castes, Scheduled Tribes, Backward Class (other than Creamy layer), land less labourer, persons holding yellow card, should file a proof along with the affidavit stating therein that he/she belongs to marginalized section of Society. The cases relating to "Crime Against Children, differently abled persons, senior citizens and marginalized sections of Society" will be given priority. The Members of the Bar are requested to provide the information regarding the cases relating to the aforesaid categories which have already been filed by them so that data in the computer can be updated for monitoring of these cases. Sd/- Joint Registrar (Judicial-II) 21.03.2016 ------------------------------------------------------------------------------------------------------- NOTICE ---------------------- Learned members of the Bar are requested to give the list of cases which have to be transferred to the Educational Tribunal, Punjab, in terms of the Jurisdiction conferred under section 7-a(12) of the Punjab affiliated colleges (security of service of employees) Act, 1974, as amended upto late and the Punjab Privately Managed Recognised Schools Employees (security) Act, 1979, in the Registry so that these cases should be listed for hearing. sd/ Registrar Judicial 1 URGENT D.B. -

Romanian Journal of Military Medicine
Founded 1897 • New Series Romanian Journal of Vol. CXXII • No. 3/2019 • December Military Medicine REVISTA DE MEDICINĂ MILITARĂ • About malpraxis, with love • Current therapeutic strategies for erectile function recovery after radical prostatectomy – literature review and meta-analysis • Toxoplasma Gondii infection and the signs of fetal affection during pregnancy as seen on ultrasound • High values of procalcitonin in non-septic patients with thermal and airway burns • Management of war-related vascular injuries. A civilian surgeon experience in the treatment of war casualties at a secondary care hospital • 3D echo in everyday life: Could it reset our threshold for interventions? • Aptamer as a proper alternative instead of monoclonal antibody in diagnosis and neutralization of menacing biological agents • Alteration of levels of thyroid hormones in acute ischemic stroke and its correlation with severity and functional outcome • Characteristics and complications of supernumerary permanent teeth in a sample of patients examined in a university pedodontics clinic • Development of quantitative real-time RT-PCR assay for detection and viral load determination of Crimean-Congo Hemorrhagic Fever (CCHF) virus • Prioritisation In delivering health services – a military health system example • Why cancer/terminal ill diagnosis unsuccessful in India: a qualitative analysis • Simulation and dynamic analysis of military marching using lower limbs anthropometric data • Drug allergies interpretation based on patient’s history alone may have therapeutic -

2017 05 31 O M.Pdf
file:///C:/Users/Niraj/Desktop/html/2017_05_31_o_m.htm N O T I C E ---------------------------- Advocates are requested to supply list of the cases which are covered by judgement of five Judges of this Hon'ble High Court in CWP No. 314 of 2001 titled as Suraj Bhan and others Vs State of Haryana and another decided on 22.07.2016 to the Registrar, (Judicial). ----------------------------------------------------------------------------------------------------------- N O T E ------------------------- It is informed to the Advocates/Parties that 29.05.2017 (Monday) has been declared as holiday in this Hon’ble High Court on account of Martyrdom Day of Sri Guru Arjan Dev Ji instead of 16.06.2017 (Friday) and the Saturday falling on 16.12.2017 will be observed as Court Working day in lieu of holiday declared on 29.05.2017 in this Hon’ble High Court. Cases which are pending for 29.05.2017 will be taken up on 30.05.2017. Similarly, 23.11.2017 (Thursday) has been declared as holiday in this Hon’ble High Court on account of Martyrdom Day of Sri Guru Teg Bahadur Ji instead of 24.11.2017 (Friday) and 24.11.2017 already declared holiday will now be observed as working day in this Hon’ble High Court. Cases which are pending for 23.11.2017 will be taken up on 24.11.2017. B.O. of Hon’ble the Chief Justice sd/- Jt. Registrar (J-II) 18.05.2017 ------------------------------------------------------------------------------------------------------------- N O T I C E -------------------------------- It is for the kind notice of the Advocates/parties that Review Applications should be filed complete in all respects and in case of delay, the same will be listed before the appropriate Hon'ble Benches by recording an office note of such defects. -
![ORDERS (INCOMPLETE MATTERS / Ias / Crlmps)]](https://docslib.b-cdn.net/cover/8138/orders-incomplete-matters-ias-crlmps-1108138.webp)
ORDERS (INCOMPLETE MATTERS / Ias / Crlmps)]
SUPREME COURT OF INDIA [ IT WILL BE APPRECIATED IF THE LEARNED ADVOCATES ON RECORD DO NOT SEEK ADJOURNMENT IN THE MATTERS LISTED BEFORE ALL THE COURTS IN THE CAUSE LIST ] DAILY CAUSE LIST FOR DATED : 06-01-2020 CHIEF JUSTICE'S COURT HON'BLE THE CHIEF JUSTICE HON'BLE MR. JUSTICE B.R. GAVAI HON'BLE MR. JUSTICE SURYA KANT (TIME : 10:30 AM) NOTE :- Request for "Not to delete a matter" and all Circulations (If the matters are not on Board for the day) need not be mentioned before the Bench. Such request be handed over to the concerned Court Masters in advance before 10.30 A.M. MISCELLANEOUS HEARING Petitioner/Respondent SNo. Case No. Petitioner / Respondent Advocate EARLY HEARING APPLICATION IN ADMITTED MATTERS 1 C.A. No. KAMLESHWAR RAJBONGSHI (DEAD) THROUGH LRS. AVIJIT BHATTACHARJEE[P-1] 3541-3542/2018 XIV-A Versus GUNESWAR RAJBONGSHI . AND ANR. AVIJIT ROY[R-1] {Mention Memo} I.A.NO. 123329/2019 (APPLN. FOR RESTORATION OF EARLY HEARING) TO BE LISTED. IA No. 123329/2019 - RESTORATION [ORDERS (INCOMPLETE MATTERS / IAs / CRLMPs)] 2 W.P.(C) No. 274/2009 ASSAM PUBLIC WORKS KAILASH PRASHAD PIL-W PANDEY[P-1] Versus UNION OF INDIA AND ORS. GAURAV DHINGRA[IMPL], B. KRISHNA PRASAD[IMPL], SNEHASISH MUKHERJEE[R-1], SHUVODEEP ROY[R-1], SHIBASHISH MISRA[R-1], SHADAN FARASAT[R-1], MOHIT D. a RAM[R-1], MOHAN PANDEY[R-1], MADHUMITA BHATTACHARJEE[R-1][IMPL] , GUNTUR PRABHAKAR[R-1], FUZAIL AHMAD AYYUBI[R-1], [INT], [IMPL], B. V. BALARAM a DAS[R-1], ABHIJIT SENGUPTA[R-1] SNEHA KALITA[IMPL], SANAND RAMAKRISHNAN[IMPL], MOHIT CHAUDHARY[IMPL], AVIJIT ROY[IMPL], CORPORATE LAW DAILY CAUSE LIST FOR DATED : 06-01-2020 CHIEF JUSTICE'S COURT a GROUP[IMPL] T. -
Daily I D.B. Motion Petition for the Wednesday Dated 14/09/2016 Cr No 1
file:///C:/Users/CRC/Desktop/html/2016_09_14_o_m.htm NOTICE Hon’ble The Chief Justice has been pleased to order that in Tax matter where bunch of appeals are decided by the Tribunal and the department is in appeal before this Hon’ble High Court, status of other cases also be mentioned in the grounds of appeal by the appellant and relied upon para i.e. where earlier order of the Tribunal is relied upon by the Tribunal while deciding the appeal, status thereof be also mentioned in grounds of appeal by the appellant. sd/- Registrar Judicial DAILY I D.B. MOTION PETITION FOR THE WEDNESDAY DATED 14/09/2016 CR NO 1 HON'BLE THE CHIEF JUSTICE HON'BLE MR. JUSTICE DEEPAK SIBAL 201 OTHER-DISTRICT CAPP-21-2016 M/S HETERO DRUGS LTD V/S M/S NECTAR RANJIT CHAWLA [ 09-SEP-16 ] LIFESCIENCES LTD M/S HETERO DRUGS LTD V/S M/S NECTAR WITH CMA-61-2016 RANJIT CHAWLA LIFESCIENCES LTD 202 HISSAR CWP-9419-2016 VED PAL TANWAR V/S STATE OF HARYANA AND VINOD S. BHARDWAJ [ 09-SEP-16 ] (MINES) OTHERS 203 MAHENDERGARH CWP-15617-2016 RAKESH KUMAR AND ANR. V/S STATE OF VIKRAM SINGH [ 09-SEP-16 ] (MINES) HARYANA AND ORS. 204 GURGAON CWP-18074-2016 YASIN @ AASIN V/S STATE OF HARYANA AND ABHIMANYU SINGH TANWAR [ 09-SEP-16 ] (MINES) OTHERS 205 UT-CHANDIGARH ITA-94-2011 (SAIT) COMMISSIONER OFD INCOME-TAX, PATIALA V/S TAJENDER K. JOSHI , AMAN BANSAL IN [ 09-SEP-16 ] BABA BANDA SINGH BAHADUR EDUCATION ITA 21 OF 2011, PANKAJ JAIN, SANGEETA TRUST, F.S. -
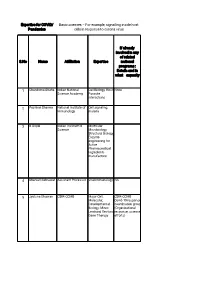
Basic Sciences – for Example, Signalling Inside Host Pandemics Cells in Response to Corona Virus
Expertise for COVID/ Basic sciences – For example, signalling inside host Pandemics cells in response to corona virus If already involved in any of related S.No Name Affiliation Expertise national programs : Details and in what capacity 1 Chandrima Shaha Indian National Cell Biology, Host None Science Academy Parasite interactions 2 Pushkar Sharma National Institute of Cell signaling, Immunology malaria 3 B Gopal Indian Institute of Molecular Science Microbiology, Structural Biology, Enzyme engineering for Active Pharmaceutical Ingredients manufacture 4 Sharvan Sehrawat Assistant Professor Viral immunology NA 5 Jyotsna Dhawan CSIR-CCMB Major-Cell, CSIR-CCMB Molecular, Covid-19 response Developmental coordination group Biology; Minor: (Organizational Lentiviral Vectors, response, science Gene Therapy efforts) 6 G. Baskaran The Institute of Theoretical Mathematical Physics. Sciences, Chennai Curious about 600 113 and biological IITMadras processes for decades. 7 Pradip Kumar Jamia Hamdard, NewMolecular NA Chakraborti Delhi 110062 Microbiology, Infectious disease, prokaryotic signalling 8 Nahid Ali CSIR Indian institute Parasitology, of chemical biology immunology 9 Raj Kumar Roy IISER Mohali Polymer and No Material Chemistry 10 Narinder K. Mehra All India Institute of COVID-19 and Medical Sciences immunity, Laboratory diagnosis 11 V. Ramanathan IIT(BHU) Varanasi Raman imaging Have been helping for disease the administrative diagnosis authorities of my city and my institute in making and distributing hand sanitizers. Till date have made around -

Zone Wise List of NASI Fellows
The National Academy of Sciences, India (The Oldest Science Academy of India) Zone wise list of Fellows & Honorary Fellows (2021) 5, Lajpatrai Road, Prayagraj – 211002, UP, India 1 The list has been divided into six zones; and each zone is further having the list of scientists of Physical Sciences and Biological Sciences, separately. 2 The National Academy of Sciences, India 5, Lajpatrai Road, Prayagraj – 211002, UP, India Zone wise list of Fellows Zone 1 (Bihar, Jharkhand, Odisha, West Bengal, Meghalaya, Assam, Mizoram, Nagaland, Arunachal Pradesh, Tripura, Manipur and Sikkim) (Section A – Physical Sciences) ACHARYA, Damodar, Chairman, Advisory Board, SOA Deemed to be University, Khandagiri Squre, Bhubanesware - 751030; ACHARYYA, Subhrangsu Kanta, Emeritus Scientist (CSIR), 15, Dr. Sarat Banerjee Road, Kolkata - 700029; ADHIKARI, Satrajit, Sr. Professor of Theoretical Chemistry, School of Chemical Sciences, Indian Association for the Cultivation of Science, 2A & 2B Raja SC Mullick Road, Jadavpur, Kolkata - 700032; ADHIKARI, Sukumar Das, Formerly Professor I, HRI,Ald; Professor & Head, Department of Mathematics, Ramakrishna Mission Vivekananda University, Belur Math, Dist Howrah - 711202; BAISNAB, Abhoy Pada, Formerly Professor of Mathematics, Burdwan Univ.; K-3/6, Karunamayee Estate, Salt Lake, Sector II, Kolkata - 700091; BANDYOPADHYAY, Sanghamitra, Professor & Director, Indian Statistical Institute, 203, BT Road, Kolkata - 700108; BANERJEA, Debabrata, Formerly Sir Rashbehary Ghose Professor of Chemistry,CU; Flat A-4/6,Iswar Chandra Nibas 68/1, Bagmari Road, Kolkata - 700054; BANERJEE, Rabin, Emeritus Professor, SN Bose National Centre for Basic Sciences, Block - JD, Sector - III, Salt Lake, Kolkata - 700098; BANERJEE, Soumitro, Professor, Department of Physical Sciences, Indian Institute of Science Education & Research, Mohanpur Campus, WB 741246; BANERJI, Krishna Dulal, Formerly Professor & Head, Chemistry Department, Flat No.C-2,Ramoni Apartments, A/6, P.G. -
19 June 2020
The Home of Solid Games www.greystonegames.com Vol. 19 Issue 16 Friday 19 June to 25 June 2020 $1 www.thesouthasianinsider.com Clash between India and China Decoding China’s Planned Aggression (Story on Page 12-13, 36-37) r Don't Cave In. China Has To Be Defeated In Its Own Game Page No. 8 Also r After Galwan, what next for India-China ties? Page No. 11 Read r China’s Reason For Clash With India Despite Saying Otherwise Page No. 12 r Are You Immune from Covid-19 ? Page No. 34 Home Business Auto NLIGHT INSURANCE Insurance (A Division of Nlight Financial LLC) (See Full Page Advt. on Page 20) Call : 917-612-3158 Friday 19 June to 25 June 2020 COMMUNITY 2 Being a police officer can be a dangerous job Working as an undercover officer in the units that deal with gangs, guns or drug dealers takes the “can be” out of the equation. It’s just dangerous. (News Agencies) As other way but Mike Stoney systems that my detectives with the POST Act is it also our undercover officers. The City Council can fix Chief of Detectives of the my partner walked ahead to use in investigations Every requires the NYPD to give Granted since the days I the Post Act with one NYPD I have the honor, but distract them from me. The day. That’s why we support a description of any and all was undercover and simple sentence. Give the also the great responsibility group challenged Mike and 99% of what the Post Act devices that are “used or buying drugs with a tape Police Commissioner the for deploying the undercover one of them, unprovoked, requires. -

Charda Suraj
www.preetnama.com BD ‹±È, B@B@ ÂØ∫ C@ ‹±È, B@B@ 1 1 On our Hindi language ؘ≈È≈ ÁΔ¡ª Reader Demand we are adding two Â≈˜Δ¡ª ıϪ, Hindi language Ò∂÷ ¡Â∂ ’≈«Ú pages Now ’«ÚÂ≈Úª Ò¬Δ Á∂÷Ø PREETNAMA «È¿±Ô≈’ √≈‚Δ ÚÀÏ√≈¬Δ‡ welcome All Hindi Writers and Readers Óπæ÷ √ßÍ≈Á’ : «ÍzÂÍ≈Ò ’Ω ÍzΔ +1 201-312-4180 www.preetnama.com √≈Ò A, ¡ß’ EI, «ÓÂΔ : BD ‹±È, B@B@ ÂØ∫ C@ ‹±È, B@B@ ÚÀÏ√≈¬Δ‡ : www.preetnama.com ¬ΔÓ∂Ò [email protected] Ì≈ ¡Â∂ ⁄ΔÈ «Ú⁄’≈ ◊ßÌΔ ±Í È≈Ò ÚËÁ∂ ¯Ω‹Δ «Úμ⁄ Î≈Ó≈, ÓØÏ≈«¬Ò ÎØÈ ¡Â∂ √Ω ¿±‹≈ Ú◊∂ ÷∂Â≈∫ ¡Â∂ ¿∞√Á∂ ’∞fi √«‘ÔØ◊Δ ⁄ΔÈ ¡Â∂ Ì≈Â È±ß «¬μ’ Á±‹∂ ¡Â∂ ≈‹ÈΔÂ’ ‰≈¡ Á∂ Ó≈‘ΩÒ «Úμ⁄ Á∞ÈΔ¡≈∫ ÁΔ Á±‹Δ «Úμ⁄ ∞’≈Ú‡≈∫ ÍÀÁ≈ ‘Ø √’ÁΔ¡≈∫ ‘È¢““ ’¬Δ Ó≈«‘ ÓßÈÁ∂ «ıÒ≈¯ ’È ¡Â∂ Ì≈ ÂØ∫ Á±Δ Á∂÷ ’∂ ÷∞Ù ‘؉◊∂¢ ¡≈«Ê’ “Ò≈¬ΔÈ ¡≈Î ¡À’⁄±¡Ò ’߇ØÒ” ¡Â∂ Íß‹ÚΔ∫ √Ì ÂØ∫ Úμ‚Δ¡≈∫ ¡Ê«ÚÚ√Ê≈Ú≈∫ «Ú⁄’≈ ‘È «’ ¡≈Í√Δ Á∞ÙÓ‰Δ ¡Â∂ ‡’≈¡ «Úμ⁄ ÁØÚ∂∫ Á∂Ù≈∫ 鱧 ±Í È≈Ò ¡≈√Δ¡≈È ¡Â∂ «Ú’√ Á∂Ù≈∫ Á∂ ¿∞ÂÍ≈Á’ Ì≈ÂΔ “Ò≈¬ΔÈ ¡≈Î ¡À’⁄±¡Ò ’߇ØÒ“ “Â∂ ‘Ø¬Δ «‘ß√≈ ¡Â∂ ¡Ò«‘Á◊Δ ÁΔ¡≈∫ ◊μÒ≈∫ ’ΔÂΔ¡≈∫ ‹≈‰ Òμ◊Δ¡≈∫ ‘È¢ Î≈«¬Á≈ ÿμ‡, È∞’√≈È «˜¡≈Á≈ ‘À, ı≈√ ÂΩ “Â∂ Ì≈Â È±ß Ï≈˜≈ «Úμ⁄ ⁄ΔÈΔ Ú√±¡≈∫ ÁΔ Ï‹≈¬∂ ¡≈͉∂ √≈Ó≈È «¬√ «Úμ⁄ B@ Ì≈ÂΔ √À«È’≈∫ ÁΔ ÓΩ ’≈È ÓØÁΔ √’≈ Ì≈ Á∂ ’¬Δ «ÚÙÒ∂Ù’ ⁄ΔÈ È≈Ò ÚÍ≈’ «ÙÂ∂ ÂØÛÈ «˜¡≈Á≈ È∞’√≈È ‘Ø √’Á≈ ‘À¢ ⁄ΔÈ «Úμ⁄ «√⁄∞¡≈È Ú∂⁄‰ «Úμ⁄ ∞⁄Δ «Á÷≈ √’Á∂ ‘È, Í Ù≈«¬Á ÿμ‡ ’∞ÙÒÂ≈ ⁄ΔÈ «÷Ò≈¯ ’∞fi ’È Á∂ ˜ÏÁ√ ÁÏ≈¡ «Úμ⁄ ‘È¢ ÁΔ¡≈∫ ◊μÒ≈∫ ’ ‘∂ ‘È ¡Â∂ ’ÀÓ∂ Á∂ √≈‘Ó‰∂ ’∞fi Ì≈Ú∞’ Ô±ÈΔÚ«√‡Δ Á∂ ⁄≈¬ΔÈ≈ √À∫‡ Î≈ √≈¿±Ê ¬∂ÙΔ¡È √‡μ‚Δ˜ ‹≈∫ ¿∞μ⁄ Ò≈◊ “Â∂¢ ‚≈’‡ ¡ÒÀ’‹À∫‚ ÒÀ∫χ ÁΔ Ì≈ √’≈Δ ¡Â∂ ˆÀ √’≈Δ ÍμË “Â∂ ’∞fi ¡«‹‘∂ ’ÁÓ È≈◊«’ ⁄ΔÈ «Úμ⁄ ω∂ ¡≈͉∂ √≈Ó≈È È±ß ÂØÛÁ∂ ‘ج∂ «Á÷‰ Á∂ ’Ø¡≈‚ΔÈ∂‡ ÍzØÎÀ√ ‘Ú≈∫◊ Ô∞ß◊√≈∫◊ ÁΔ ÁÒΔÒ ‘À «’ 鱧 √Ò≈‘ -
![Departmental Directory [AHB 2021]](https://docslib.b-cdn.net/cover/2198/departmental-directory-ahb-2021-8812198.webp)
Departmental Directory [AHB 2021]
1 2021 2 e-AHB will be getting updated regularly. Any discrepancy / update, may kindly be intimated at the below given e-mail id. DIRECTORATE OF INCOME TAX (PR, P&P) 6th Floor, Mayur Bhawan, Connaught Circus New Delhi-110001 Ph: 011-23413403, 23413317, 23411280, 23411267 E-mail: [email protected] "Aaykar Kutumb" app is now available in Google Play Store (Andriod) & App store (iOS device). Follow us on : https://www.incometaxindia.gov.in/ 3 Calendars 07 DGIT(Investigation) Conti.. Yearly Planner 2021 08 Lucknow 73 List of Holidays 09 Mumbai 76 Personal Information 11 New Delhi 77 Patna 79 Ministry of Finance 13 Pune 80 Central Board of Direct Taxes 18 Pr. CCIT(Exemptions) 85 Pr. DGIT (I&CI) 87 Pr. CCIT (International Taxation) 90 26 PCCIT Regions on Map of India Pr. CCIT (NaFAC) 96 Pr. CCIT (NFAC) 109 Alphabetical list 27 Pr.CCIT/CCIT/Pr.DGIT/DGIT Field Stations Directorates of Income Tax Pr. CCsIT (CCA) at a Glance 128 Administration & Tax Payer 35 Ahmedabad 129 Services (Admn. & TPS) Bengaluru 131 Systems 37 Bhopal 132 Human Resource Development (HRD) 43 Bhubaneswar 133 Legal & Research (L&R) 44 Chandigarh 133 Vigilance 44 Chennai 133 Delhi 135 Guwahati 137 Hyderabad 138 Training Institutes (NADT) Jaipur 139 DGIT (NADT) 48 Kanpur 140 Regional Training Institute 49 Kochi 140 WB, Sikkim & NER 141 DGIT(Investigation) Lucknow 143 Mumbai 144 Ahmedabad 52 Nagpur 146 Bengaluru 54 Patna 147 Bhopal 56 Pune 148 Chandigarh 58 Chennai 61 Hyderabad 63 Jaipur 66 Kochi 68 Official Language 153 WB, Sikkim & NER 69 Valuation Wing 164 4 CONTENT Conti.. -
Results of the Macro-Level Analysis of the Ip-Uni Link Project
Trends in R&D Cooperation among EU and BRIC countries’ Higher Education Institutions RESULTS OF THE MACRO-LEVEL ANALYSIS OF THE IP-UNI LINK PROJECT Final Version , 11 /2009 DEVELOPED BY THE IP-UNILINK PROJECT CONSORTIUM. University of Alicante, Spain Mayr, Alexandra Barluenga, Maria C. State University of Campinas, Brazil Reydon, Bastiaan Pereira, Andréia Mara Electrotechnical University, Russia Afanasjev, Petr Chalmers Technology Foundation - CIT, Sweden Scheinberg, Sari Norgren, Andreas Jagiellonian University, IP Law Institute, Poland Kasprzycki, Dariusz Ożegalska-Trybalska, Justyna Felchner, Krzysztof Kunming University of Science and Technology, China CHEN Xinghua LI Xin LI Na Wang Taining JIA Miao Indian Institute of Technology Roorkee, IPR Cell, India Ghosh, P. K. Sinha, Babita Himanshu, Joshi Meenakshi, Rode CO-FINANCED BY : Erasmus Mundus Programme of the European Union EDITED BY: University of Alicante, International Project Management Office Edificio Germán Bernácer, Apartado de correos 99, E-03080 Alicante, Spain © IP-Unilink Consotrium, 2009 This publication reflects the views only of the authors, and the European Commission cannot be held responsible for any use which may be made of the information contained therein. 2 TABLE OF CONTENTS 1. Introduction ............................................................................................. 7 1.1. Preamble .................................................................................................................... 7 1.2. Objectives and Methodology ................................................................................... -

Toxin-Antitoxin
201 9 Biofilms: A Phenotypic Mechanism of Bacteria Conferring Tolerance Against 18 Stress and Antibiotics Anwar Alam, Ashutosh Kumar, Prajna Tripathi, Nasreen Z. Ehtesham, and Seyed E. Hasnain Abstract Biofilm, as a heterogenous congregation of microbial cells enclosed within a pellicle, has largely gained attention due to their historical importance in environ- ment as sludges, flocs, slimes, etc. Biofilms in medical research have been an active area of research in periodontics, in wounds, and in surgical implants. With the availability of whole genome sequences, it is now evident that the mechanisms that control biofilm formation have largely remained conserved during the course of evolution, pointing to the fact that biofilm formation is an Anwar Alam, Ashutosh Kumar and Prajna Tripathi have contributed equally to this chapter. A. Alam JH Institute of Molecular Medicine, Jamia Hamdard, New Delhi, Delhi, India Inflammation Biology and Cell Signaling Laboratory, ICMR-National Institute of Pathology, Safdarjung Hospital Campus, New Delhi, Delhi, India A. Kumar Department of Microbiology, Tripura University (A Central University), Agartala, Tripura, India P. Tripathi National Institute of Immunology, New Delhi, Delhi, India JH Institute of Molecular Medicine, Jamia Hamdard, New Delhi, Delhi, India N. Z. Ehtesham Inflammation Biology and Cell Signaling Laboratory, ICMR-National Institute of Pathology, Safdarjung Hospital Campus, New Delhi, Delhi, India e-mail: [email protected] S. E. Hasnain (*) JH Institute of Molecular Medicine, Jamia Hamdard, New Delhi, Delhi, India Dr Reddy’s Institute of Life Sciences, University of Hyderabad Campus, Hyderabad, India e-mail: [email protected] # Springer Nature Singapore Pte Ltd. 2019 315 S. E.