Barium, Inorganic Water-Soluble Compounds
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Barium Acetate
Barium acetate sc-202968 Material Safety Data Sheet Hazard Alert Code Key: EXTREME HIGH MODERATE LOW Section 1 - CHEMICAL PRODUCT AND COMPANY IDENTIFICATION PRODUCT NAME Barium acetate STATEMENT OF HAZARDOUS NATURE CONSIDERED A HAZARDOUS SUBSTANCE ACCORDING TO OSHA 29 CFR 1910.1200. NFPA FLAMMABILITY1 HEALTH2 HAZARD INSTABILITY0 SUPPLIER Company: Santa Cruz Biotechnology, Inc. Address: 2145 Delaware Ave Santa Cruz, CA 95060 Telephone: 800.457.3801 or 831.457.3800 Emergency Tel: CHEMWATCH: From within the US and Canada: 877-715-9305 Emergency Tel: From outside the US and Canada: +800 2436 2255 (1-800-CHEMCALL) or call +613 9573 3112 PRODUCT USE Chemical reagent, acetates, mordant for printing fabrics, catalyst manufacturing, paint and varnish dryers, lubricating oil and grease additive. SYNONYMS C4-H6-O4-Ba, Ba(C2H3O2)2, "barium diacetate", "acetic acid barium salt", "octan barnaty" Section 2 - HAZARDS IDENTIFICATION CHEMWATCH HAZARD RATINGS Min Max Flammability: 1 Toxicity: 2 Body Contact: 2 Min/Nil=0 Low=1 Reactivity: 1 Moderate=2 High=3 Chronic: 2 Extreme=4 CANADIAN WHMIS SYMBOLS 1 of 12 EMERGENCY OVERVIEW RISK Harmful by inhalation and if swallowed. POTENTIAL HEALTH EFFECTS ACUTE HEALTH EFFECTS SWALLOWED ! Accidental ingestion of the material may be harmful; animal experiments indicate that ingestion of less than 150 gram may be fatal or may produce serious damage to the health of the individual. ! Ingestion of soluble barium compounds may result in ulceration of the mucous membranes of the gastrointestinal tract, tightness in the muscles of the face and neck, gastroenteritis, vomiting, diarrhea, muscular tremors and paralysis, anxiety, weakness, labored breathing, cardiac irregularity due to contractions of smooth striated and cardiac muscles (often violent and painful), slow irregular pulse, hypertension, convulsions and respiratory failure. -

Toxicological Profile for Barium and Barium Compounds
TOXICOLOGICAL PROFILE FOR BARIUM AND BARIUM COMPOUNDS U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Public Health Service Agency for Toxic Substances and Disease Registry August 2007 BARIUM AND BARIUM COMPOUNDS ii DISCLAIMER The use of company or product name(s) is for identification only and does not imply endorsement by the Agency for Toxic Substances and Disease Registry. BARIUM AND BARIUM COMPOUNDS iii UPDATE STATEMENT A Toxicological Profile for Barium and Barium Compounds, Draft for Public Comment was released in September 2005. This edition supersedes any previously released draft or final profile. Toxicological profiles are revised and republished as necessary. For information regarding the update status of previously released profiles, contact ATSDR at: Agency for Toxic Substances and Disease Registry Division of Toxicology and Environmental Medicine/Applied Toxicology Branch 1600 Clifton Road NE Mailstop F-32 Atlanta, Georgia 30333 BARIUM AND BARIUM COMPOUNDS iv This page is intentionally blank. v FOREWORD This toxicological profile is prepared in accordance with guidelines developed by the Agency for Toxic Substances and Disease Registry (ATSDR) and the Environmental Protection Agency (EPA). The original guidelines were published in the Federal Register on April 17, 1987. Each profile will be revised and republished as necessary. The ATSDR toxicological profile succinctly characterizes the toxicologic and adverse health effects information for the hazardous substance described therein. Each peer-reviewed profile identifies and reviews the key literature that describes a hazardous substance's toxicologic properties. Other pertinent literature is also presented, but is described in less detail than the key studies. The profile is not intended to be an exhaustive document; however, more comprehensive sources of specialty information are referenced. -
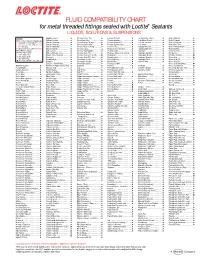
FLUID COMPATIBILITY CHART for Metal Threaded Fittings Sealed with Loctite¨ Sealants LIQUIDS, SOLUTIONS & SUSPENSIONS
FLUID COMPATIBILITY CHART for metal threaded fittings sealed with Loctite® Sealants LIQUIDS, SOLUTIONS & SUSPENSIONS LEGEND: Bagasse Fibers.......................... Chlorobenzene Dry ................... Ferrous Chloride ...................... Ion Exclusion Glycol ................. Nickel Chloride.......................... All Loctite® Anaerobic Sealants are Barium Acetate ........................ Chloroform Dry......................... Ferrous Oxalate......................... Irish Moss Slurry...................... Nickel Cyanide ......................... Compatible Including #242®, 243, Barium Carbonate..................... Chloroformate Methyl............... Ferrous Sulfate10%.................. Iron Ore Taconite ..................... Nickel Fluoborate ..................... 542, 545, 565, 567, 569, 571, 572, Barium Chloride........................ Chlorosulfonic Acid .................. Ferrous Sulfate (Sat)................. Iron Oxide ................................ Nickel Ore Fines ....................... 577, 580, 592 Barium Hydroxide..................... Chrome Acid Cleaning .............. Fertilizer Sol ............................. Isobutyl Alcohol ....................... Nickel Plating Bright ................. † Use Loctite® #270, 271™, 277, 554 Barium Sulfate.......................... Chrome Liquor.......................... Flotation Concentrates.............. Isobutyraldehyde ..................... Nickel Sulfate ........................... Not Recommended Battery Acid .............................. Chrome Plating -

Chemical Names and CAS Numbers Final
Chemical Abstract Chemical Formula Chemical Name Service (CAS) Number C3H8O 1‐propanol C4H7BrO2 2‐bromobutyric acid 80‐58‐0 GeH3COOH 2‐germaacetic acid C4H10 2‐methylpropane 75‐28‐5 C3H8O 2‐propanol 67‐63‐0 C6H10O3 4‐acetylbutyric acid 448671 C4H7BrO2 4‐bromobutyric acid 2623‐87‐2 CH3CHO acetaldehyde CH3CONH2 acetamide C8H9NO2 acetaminophen 103‐90‐2 − C2H3O2 acetate ion − CH3COO acetate ion C2H4O2 acetic acid 64‐19‐7 CH3COOH acetic acid (CH3)2CO acetone CH3COCl acetyl chloride C2H2 acetylene 74‐86‐2 HCCH acetylene C9H8O4 acetylsalicylic acid 50‐78‐2 H2C(CH)CN acrylonitrile C3H7NO2 Ala C3H7NO2 alanine 56‐41‐7 NaAlSi3O3 albite AlSb aluminium antimonide 25152‐52‐7 AlAs aluminium arsenide 22831‐42‐1 AlBO2 aluminium borate 61279‐70‐7 AlBO aluminium boron oxide 12041‐48‐4 AlBr3 aluminium bromide 7727‐15‐3 AlBr3•6H2O aluminium bromide hexahydrate 2149397 AlCl4Cs aluminium caesium tetrachloride 17992‐03‐9 AlCl3 aluminium chloride (anhydrous) 7446‐70‐0 AlCl3•6H2O aluminium chloride hexahydrate 7784‐13‐6 AlClO aluminium chloride oxide 13596‐11‐7 AlB2 aluminium diboride 12041‐50‐8 AlF2 aluminium difluoride 13569‐23‐8 AlF2O aluminium difluoride oxide 38344‐66‐0 AlB12 aluminium dodecaboride 12041‐54‐2 Al2F6 aluminium fluoride 17949‐86‐9 AlF3 aluminium fluoride 7784‐18‐1 Al(CHO2)3 aluminium formate 7360‐53‐4 1 of 75 Chemical Abstract Chemical Formula Chemical Name Service (CAS) Number Al(OH)3 aluminium hydroxide 21645‐51‐2 Al2I6 aluminium iodide 18898‐35‐6 AlI3 aluminium iodide 7784‐23‐8 AlBr aluminium monobromide 22359‐97‐3 AlCl aluminium monochloride -

Toxicological Profile for Barium and Barium
BARIUM AND BARIUM COMPOUNDS 1 1. PUBLIC HEALTH STATEMENT This public health statement tells you about barium and barium compounds and the effects of exposure to these chemicals. The Environmental Protection Agency (EPA) identifies the most serious hazardous waste sites in the nation. These sites are then placed on the National Priorities List (NPL) and are targeted for long-term federal clean-up activities. Barium and barium compounds have been found in at least 798 of the 1,684 current or former NPL sites; however, the total number of NPL sites evaluated for these substances is not known. This information is important because these sites may be sources of exposure and exposure to this substance may harm you. When a substance is released either from a large area, such as an industrial plant, or from a container, such as a drum or bottle, it enters the environment. Such a release does not always lead to exposure. You can be exposed to a substance only when you come in contact with it. You may be exposed by breathing, eating, or drinking the substance, or by skin contact. If you are exposed to barium and barium compounds, many factors will determine whether you will be harmed. These factors include the dose (how much), the duration (how long), and how you come in contact with them. You must also consider any other chemicals you are exposed to and your age, sex, diet, family traits, lifestyle, and state of health. 1.1 WHAT IS BARIUM? Barium is a silvery-white metal that takes on a silver-yellow color when exposed to air. -

Safety Data Sheet: Barium Acetate
safety data sheet Safe Work Australia - Code of Practice Barium acetate ≥ 99%, p.a., ACS article number: 2553 date of compilation: 2016-12-06 Version: GHS 1.0 en SECTION 1: Identification of the substance/mixture and of the company/undertaking 1.1 Product identifier Identification of the substance Barium acetate Article number 2553 Registration number (REACH) This information is not available. Index No 056-002-00-7 EC number 208-849-0 CAS number 543-80-6 1.2 Relevant identified uses of the substance or mixture and uses advised against Identified uses: laboratory chemical 1.3 Details of the supplier of the safety data sheet Carl Roth GmbH + Co KG Schoemperlenstr. 3-5 D-76185 Karlsruhe Germany Telephone: +49 (0) 721 - 56 06 0 Telefax: +49 (0) 721 - 56 06 149 e-mail: [email protected] Website: www.carlroth.de Competent person responsible for the safety data : Department Health, Safety and Environment sheet e-mail (competent person) : [email protected] 1.4 Emergency telephone number Emergency information service Poison Centre Munich: +49/(0)89 19240 SECTION 2: Hazards identification 2.1 Classification of the substance or mixture Classification according to Regulation (EC) No 1272/2008 (CLP) Classification acc. to GHS Section Hazard class Hazard class and cat- Hazard egory state- ment 3.1O acute toxicity (oral) (Acute Tox. 4) H302 3.1I acute toxicity (inhal.) (Acute Tox. 4) H332 3.8 specific target organ toxicity - single exposure (STOT SE 1) H370 Australia (en) Page 1 / 11 safety data sheet according to Regulation (EC) No. 1907/2006 (REACH), amended by 2015/830/EU Barium acetate ≥ 99%, p.a., ACS article number: 2553 Remarks For full text of Hazard- and EU Hazard-statements: see SECTION 16. -

Supporting Information
Electronic Supplementary Material (ESI) for Journal of Materials Chemistry A This journal is © The Royal Society of Chemistry 2013 Supporting Information Barium oxide promoted Ni/YSZ solid-oxide fuel cells for direct utilization of methane By Shamiul Islam,a and Josephine M. Hill *a Department of Chemical and Petroleum Engineering, University of Calgary, 2500 University Dr. NW, Calgary, Alberta, T2N 1N4, (Canada) E-mail: ([email protected]) Electronic Supplementary Material (ESI) for Journal of Materials Chemistry A This journal is © The Royal Society of Chemistry 2013 -1 TGA analysis of Ba(NO3)2 powder was carried out at (a) 773 K and (b) 873 K in flowing N2 with a ramp rate of 10 K min and a holding time of 5 h at the respective temperatures. At 773 K, Ba(NO3)2 barely decomposed to its oxide and the weight loss corresponds to only 4 %. However, when the temperature was increased to 873 K, a weight loss of 43% is observed, which was close to the theoretical loss of 41% for the decomposition of Ba(NO3)2 to its oxide (BaO). Thus a calcination temperature of 873 K was chosen for the thermal decomposition of impregnated Ba(NO3)2 particles to BaO in the sintered NiO/YSZ anodes. Supplementary Fig. S1. Thermogravimetric analysis of Ba(NO3)2 powder. (a) 773 K and (b) 873 K. Electronic Supplementary Material (ESI) for Journal of Materials Chemistry A This journal is © The Royal Society of Chemistry 2013 Supplementary Fig. S2. In-situ measurement of the temperature and power during microwave experiments. Electronic Supplementary Material (ESI) for Journal of Materials Chemistry A This journal is © The Royal Society of Chemistry 2013 (a) (b) BaCO3 Supplementary Fig. -

Toxicological Review of Barium and Compounds (Cas No. 7440-39-3)
EPA/635/R-05/001 www.epa.gov/iris TOXICOLOGICAL REVIEW OF BARIUM AND COMPOUNDS (CAS No. 7440-39-3) In Support of Summary Information on the Integrated Risk Information System (IRIS) March 1998 Minor revisions January 1999 Reference dose revised June 2005 U.S. Environmental Protection Agency Washington, DC DISCLAIMER This document has been reviewed in accordance with U.S. Environmental Protection Agency policy and approved for publication. Mention of trade names or commercial products does not constitute endorsement or recommendation for use. ii CONTENTS—TOXICOLOGICAL REVIEW OF BARIUM AND COMPOUNDS (CAS NO. 7440-39-3) LIST OF TABLES .............................................................v LIST OF FIGURES ............................................................v FOREWORD ................................................................ vi AUTHORS, CONTRIBUTORS, AND REVIEWERS ............................... vii 1. INTRODUCTION ..........................................................1 2. CHEMICAL AND PHYSICAL INFORMATION .................................3 3. TOXICOKINETICS ........................................................6 3.1. ABSORPTION ........................................................6 3.1.1. Gastrointestinal Absorption .........................................6 3.1.2. Respiratory Tract Absorption .......................................7 3.1.3. Dermal Absorption................................................7 3.2. DISTRIBUTION.......................................................8 3.3. ELIMINATION AND EXCRETION -

Barium Acetate Material Safety Data Sheet
BARIUM ACETATE MATERIAL SAFETY DATA SHEET SECTION 1: IDENTIFICATION OF THE SUBSTANCE/MIXTURE AND OF THE COMPANY/UNDERTAKING 1.1. Product identifier Product form : Substance CAS No : 543-80-6 Product code : 30282, 38158 Formula : (CH3.COO)2Ba 1.2. Relevant identified uses of the substance or mixture and uses advised against 1.2.1.Relevant identified uses Industrial/professional use spec : Industrial For professional use only Use of the substance/mixture : Laboratory Reagent 1.2.2. Uses advised against No additional information available 1.3. Details of the manufacturer of the safety data sheet Techno Pharmchem Plot No.1022, Modern Industrial Estate, Bahadurgarh-124507, India T +91 11 23646422 [email protected] 1.4. Emergency telephone number Emergency number: +91 11 23646422 (9:30am – 5.30pm) SECTION 2: HAZARDS IDENTIFICATION 2.1. Classification of the substance or mixture Classification according to regulation (EC) No. 1272/2008[CLP] Acute toxicity (inhal.), H332 Category 4 Acute toxicity (oral), H302 Category 4 Full text of hazard classes and H- statements : see section 16 Classification according to directive 67/548/EEC [DSD] or 1999/45/EC [DPD] Xn; R20 Xn; R22 Full text of R-phrases: see section16 Adverse physicochemical, human health and environmental effects No additional information available The information contained herein in good faith but makes no representations as to its comprehensiveness or accuracy. This document is intended only as a guide to the appropriate precautionary handling of the material by a properly trained person using this product. The conditions or methods of handling, storage, use or disposal of the product are beyond our control and may be beyond our knowledge. -

Production and Characterization of Barium-Titanate Nanofibers
Vol. 137 (2020) ACTA PHYSICA POLONICA A No. 4 Special issue: ICCESEN-2019 Production and Characterization of Barium-Titanate Nanofibers N. Çiçek Bezira;∗, A. Evcinb, A. İnceoğlua, O. Ceylanc and B. Özcana aSüleyman Demirel University, Department of Physics, Faculty of Art and Science, Isparta, Turkey bAfyon Kocatepe University, Department of Materials Science and Engineering, Afyonkarahisar, Turkey cAkdeniz University, ElmalıVocational School, Antalya, Turkey This paper reports production of nanofibers with voltage value of 20 kV, different fluid velocities (0.1 ml/h, 0.5 ml/h), different durations (2 min, 5 min), and distance of 7 cm in the electrospin assembly. The mor- phology of the produced nanofibers was observed before and after heat treatment by scanning electron microscope. The crystal structure of the nanofibers was examined by X-ray diffraction. In addition, thermal analysis/thermal gravimetric analysis of nanofibers was performed. X-ray diffraction measurements showed that the samples were crystalline in barium titanate. It was observed that the diameters of the nanofibers increased when the flow rate and time increased, while the diameters of the nanofibers decreased when the flow rate and time decreased. Scanning electron microscope images showed how the morphology of the samples changed by heat treatment. As a result, characterization results were found to be consistent with the literature. DOI: 10.12693/APhysPolA.137.542 PACS/topics: barium-titanate, electrospinning, nanofibers, XRD, SEM 1. Introduction 2. Materials and method Nanotechnology refers to the control and reconstruc- The fabrication of the barium-titanate nanofibers tion of material, which is smaller than 100 nm or at least was the results of the following steps: polyvinylpyrroli- one dimension [1]. -

Barium in Drinking-Water
WHO/SDE/WSH/03.04/76 English only Barium in Drinking-water Background document for development of WHO Guidelines for Drinking-water Quality © World Health Organization 2004 Requests for permission to reproduce or translate WHO publications - whether for sale of for non- commercial distribution - should be addressed to Publications (Fax: +41 22 791 4806; e-mail: [email protected]. The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. The mention of specific companies or of certain manufacturers' products does not imply that they are endorsed or recommended by the World Health Organization in preference to others of a similar nature that are not mentioned. Errors and omissions excepted, the names of proprietary products are distinguished by initial capital letters. The World Health Organization does not warrant that the information contained in this publication is complete and correct and shall not be liable for any damage incurred as a results of its use. Preface One of the primary goals of WHO and its member states is that “all people, whatever their stage of development and their social and economic conditions, have the right to have access to an adequate supply of safe drinking water.” A major WHO function to achieve such goals is the responsibility “to propose ... regulations, and to make recommendations with respect to international health matters ....” The first WHO document dealing specifically with public drinking-water quality was published in 1958 as International Standards for Drinking-water. -
![United Statespatent [191 [11] 4,335,109 Hill [45] Jun](https://docslib.b-cdn.net/cover/3757/united-statespatent-191-11-4-335-109-hill-45-jun-4653757.webp)
United Statespatent [191 [11] 4,335,109 Hill [45] Jun
SR 6/15/82 XR 4933591019 United StatesPatent [191 [11] 4,335,109 Hill [45] Jun. 15, 1982 [54] WATER REPELLENT AQUEOUS WOOD [5 6] References Cited TREATING SOLUTIONS U.S. PATENT DOCUMENTS Inventor: Robert E. Hill, Webster Groves, Mo. 2,571,030 10/1951 Govett et a1. ..................... 424/68 [75] 2,876,163 3/1959 Garizio et al. .................. .. 424/68 [73] Assignee: Koppers Company, Inc., Pittsburgh, Primary Examiner—-Lorenzo B. Hayes Pa. Attorney, Agent, or Firm-Donald M. MacKay [57] ABSTRACT [21] Appl. No.: 216,123 An increased water repellency is imparted to wood and [22] Filed: Dec. 15, 1930 other cellulosic materials with an aqueous solution con taining a mixture of an aluminum ~halohydrate and a water soluble salt of a mono, di or trivalent cation se Related US. Application Data lected from zinc, manganese, barium, calcium, cobalt, [63] Continuation of Ser. No. 96,333, Nov. 21, 1979, aban magnesium, nickel, copper, cadmium, strontium, beryl doned. lium, lead, mercury, chromium, sodium, lithium, and potassium and- a monovalent anion selected from for [51] 1m. (:1.3 .................... .. A01N 59/20;A01N 59/06 mate acetate, haloacetate, acrylate, methacrylate, propi [52] us. (:1. ..; ................................... .. 424/140; 106/2; onate, chloro and bromo-propionate, butyrate, isobu 106/1505; 424/145; 424/146; 424/150; tyrate, nitrate, sulfamate, iodide, bromide, and chloride, 424/153; 424/154; 424/289; 424/291; 424/293; said water soluble salt excluding the nitrates, sulfamates, I 424/294; 424/295; 427/440 chlorides and bromides of sodium, potassium and lith Field Of Search I. ............... .. 106/2, 1505; 424/68,.