Lack of Empathy in Patients with Narcissistic Personality Disorder
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Subtypes, Dimensions, Levels, and Mental States in Narcissism and Narcissistic Personality Disorder
Subtypes, Dimensions, Levels, and Mental States in Narcissism and Narcissistic Personality Disorder Kenneth N. Levy Pennsylvania State University Various conceptualizations of subtypes, levels, and dimensions of narcissism and narcissistic person- ality disorder (NPD) are considered with a particular focus on overt grandiose presentations and covert vulnerable presentations. Evidence supporting this distinction and clinical vignettes to illustrate it are presented as well as their implications for clinical work with NPD patients. The research and clinical evidence points to the conclusion that these broad categorical subtypes are better conceptualized as dimensions on which individual patients vary on relative levels, thus suggesting that grandiose and vul- nerable presentations represent two sides of the same coin. A case example and clinical implications are provided and discussed. C 2012 Wiley Periodicals, Inc. J. Clin. Psychol: In Session 00:1–12, 2012. Keywords: narcissism; narcissistic personality disorder; grandiose subtype; vulnerable subtype Beginning with its inclusion in the Diagnostic and Statistical Manual (DSM; 1968, 1980, 1994, 2000), narcissistic personality disorder (NPD) has been conceptualized predominately by its overt grandiose features. However, the definition of NPD articulated in the DSM-III and its successors, DSM-III-R and DSM-IV, has been criticized for failing to fully capture the intended clinical phenomena (Cooper & Ronningstam, 1992; Gabbard, 1989; Gunderson et al., 1991). These authors have noted that the DSM criteria have focused narrowly on aspects of the conceptual approaches of Kernberg and Millon, emphasizing the more overt form of narcissism. However, theoretical and empirical work is now converging to suggest that NPD is not a homogenous disorder and subtypes likely exist within this group. -

Differences in Narcissistic Presentation in Abused and Non- Abused Children and Adolescents
The University of Southern Mississippi The Aquila Digital Community Dissertations Summer 8-2014 Differences in Narcissistic Presentation in Abused and Non- Abused Children and Adolescents Mallory Laine Malkin University of Southern Mississippi Follow this and additional works at: https://aquila.usm.edu/dissertations Part of the Applied Behavior Analysis Commons, Child Psychology Commons, Clinical Psychology Commons, School Psychology Commons, and the Social Psychology Commons Recommended Citation Malkin, Mallory Laine, "Differences in Narcissistic Presentation in Abused and Non-Abused Children and Adolescents" (2014). Dissertations. 274. https://aquila.usm.edu/dissertations/274 This Dissertation is brought to you for free and open access by The Aquila Digital Community. It has been accepted for inclusion in Dissertations by an authorized administrator of The Aquila Digital Community. For more information, please contact [email protected]. The University of Southern Mississippi DIFFERENCES IN NARCISSISTIC PRESENTATION IN ABUSED AND NON-ABUSED CHILDREN AND ADOLESCENTS by Mallory Laine Malkin Abstract of a Dissertation Submitted to the Graduate School of the University of Southern Mississippi in Partial Fulfillment of the Requirements for the Degree of Doctor of Philosophy August 2014 ABSTRACT DIFFERENCES IN NARCISSISTIC PRESENTATION IN ABUSED AND NON-ABUSED CHILDREN AND ADOLESCENTS by Mallory Laine Malkin August 2014 The present study examined whether children and adolescents who have been victims of sexual or physical abuse report higher levels of narcissistic tendencies than children and adolescents who have not been victims of abuse. Inaddition to narcissism, internalizing symptoms, externalizing behaviors, and risky behaviors were evaluated, as such issues have been associated with both maltreatment (Baer & Maschi, 2003) and narcissism (Barry & Malkin, 2010; Bushman & Baumeister, 1998). -

Narcissism, Confidence, and Risk Attitude
Journal of Behavioral Decision Making J. Behav. Dec. Making, 17: 297–311 (2004) DOI: 10.1002/bdm.475 Narcissism, Confidence, and Risk Attitude W. KEITH CAMPBELL*, ADAM S. GOODIE and JOSHUA D. FOSTER University of Georgia, USA ABSTRACT The present research addresses whether narcissists are more overconfident than others and whether this overconfidence leads to deficits in decision making. In Study 1, nar- cissism predicted overconfidence. This was attributable to narcissists’ greater confi- dence despite no greater accuracy. In Study 2, participants were offered fair bets on their answers. Narcissists lost significantly more points in this betting task than non- narcissists, due both to their greater overconfidence and greater willingness to bet. Finally, in Study 3, narcissists’ predictions of future performance were based on per- formance expectations rather than actual performance. This research extends the litera- ture on betting on knowledge to the important personality dimension of narcissism. Copyright # 2004 John Wiley & Sons, Ltd. key words risk taking; overconfidence; decision making; narcissism; personality; adults Individual differences matter in decision making. Gigerenzer and Hoffrage (1995), among many others, have pointed out that average decision strategies can be misleading, as they may reflect decision strategies that no single decision-maker employs. It is often better to explore the decisions that individuals reach. Furthermore, reliable differences in which kinds of people make which kind of decisions are important. Stanovich and West (2000), for example, have defended the reality of various cognitive illusions by demonstrating that people who violate conventionally defined norms tend to be those who perform less well in other domains. Looking at the same base of data, Funder (2000) argued that the observed correlation constitutes standard validation of the test items, and that the ability of some people to solve the problems correctly indicates an absence of systematic irrationality. -

Emotional Intelligence Is Used by Dark Personalities to Emotionally Manipulate Others ⇑ ⇑ Ursa K.J
Personality and Individual Differences xxx (2014) xxx–xxx Contents lists available at ScienceDirect Personality and Individual Differences journal homepage: www.elsevier.com/locate/paid Is there a ‘‘dark intelligence’’? Emotional intelligence is used by dark personalities to emotionally manipulate others ⇑ ⇑ Ursa K.J. Nagler a, ,1, Katharina J. Reiter a, ,1, Marco R. Furtner a, John F. Rauthmann b a Institute of Psychology, Leopold-Franzens Universität Innsbruck, Austria b Institute of Psychology, Humboldt-Universität zu Berlin, Germany article info abstract Article history: Potential ‘‘darker sides’’ of socio-emotional intelligence (SEI) have been repeatedly noted. We examine Available online xxxx whether SEI is associated with emotional manipulation of others when used by dark personalities (Dark Triad: narcissism, Machiavellianism, psychopathy). In N = 594 participants, narcissism was positively, Keywords: Machiavellianism negatively, and psychopathy positively and negatively associated with SEI. Moreover, Emotional manipulation narcissism and psychopathy moderated links between facets of emotional intelligence and emotional Dark Triad manipulation. Findings are discussed in context of a ‘‘dark intelligence’’ used for malicious intents. Narcissism Ó 2014 Elsevier Ltd. All rights reserved. Machiavellianism Psychopathy Emotional intelligence Social intelligence 1. Introduction & Sachse, 2010), including communication competence (e.g., Diez, 1984), social intelligence (e.g., Cantor & Kihlstrom, 1987; Gardner, Are social and emotional skills always used for good intentions? 1993; Guilford, 1967; Thorndike, 1920), and emotional intelligence Potential ‘‘dark sides’’ of socio-emotional intelligence (SEI), such as (e.g., Mayer & Salovey, 1997; Salovey & Mayer, 1990). Not only the emotional manipulation of others (Austin, Farrelly, Black, & interpersonal (e.g., encoding and decoding social information) Moore, 2007), have garnered interest during the last years. -

Narcissistic Personality Disorder – Has It Become an Epidemic? 3 CE Hours
Chapter 7: Narcissistic Personality Disorder – Has It Become an Epidemic? 3 CE Hours By: Kathryn Brohl, MA, LMFT Learning objectives Upon completion of this course, the learner should be able to: Describe at least three relationship characteristics of individuals Define narcissistic personality disorder (NPD) as it relates to the with NPD. Diagnostic and Statistical Manual of Mental Health Disorders, Identify at least five diagnostic criteria for NPD as they relate to Fifth Edition (DSM-5) (2013). the DSM-5. Identify personality disorder as it relates to the DSM-5. Recognize challenges to treating individuals with NPD. Compare NPD to other Cluster B Personality Disorders, outlined Describe treatment for individuals with NPD. in the Statistical Manual of Mental Health Disorders, Fifth Edition, Compare and describe ICD Revision 10 personality disorder (2013). criteria to DSM-5 personality disorder criteria. Explain the male and female prevalence of NPD. Explain how NPD affects relationships. Introduction Narcissism has been examined by mental health professionals for years, society is more accepting of persons with NPD, or does the trend in and yet something has occurred recently within our society that seems to cultivating entitlement as it relates to expressing one’s opinions and have blurred narcissism traits with the clinical diagnosis of narcissistic behaviors more loudly simply mean that people are feeling more personality disorder (NPD) and accepted societal behavior. Recently, a empowered? And as a result, are people becoming desensitized to the shift has occurred in shared cultural values toward narcissism and self- feelings of others? Furthermore, are mental health professionals seeing admiration and some of these traits have become social norms. -

Fluctuations in Grandiose and Vulnerable Narcissistic States: a Momentary Perspective
1 Fluctuations in grandiose and vulnerable narcissistic states: A momentary perspective Elizabeth A. Edershile Aidan G.C. Wright University of Pittsburgh This manuscript reflects a portion of the first author’s Master’s thesis. Aidan Wright’s effort on this project was supported by the National Institute of Mental Health (L30 MH101760). Participant recruitment was supported by the University of Pittsburgh’s Clinical and Translational Science Institute, which is funded by the National Institutes of Health (NIH) Clinical and Translational Science Award (CTSA) program (UL1 TR001857). The CTSA program is led by the NIH's National Center for Advancing Translational Sciences (NCATS). The opinions expressed are solely those of the authors and not those of the funding source. This manuscript and supporting data and analyses has been posted on Open Science Framework and can be accessed at https://osf.io/c9uea/ Correspondence concerning this article should be addressed to Elizabeth Edershile, Department of Psychology, University of Pittsburgh, 3137 Sennott Square, 210 S. Bouquet St., Pittsburgh, PA, 15260. E-mail: [email protected] 2 Abstract Theories of narcissism emphasize the dynamic processes within and between grandiosity and vulnerability. Research seeking to address this has either not studied grandiosity and vulnerability together or has used dispositional measures to assess what are considered to be momentary states. Emerging models of narcissism suggest grandiosity and vulnerability can further be differentiated into a three-factor structure – Exhibitionistic Grandiosity, Entitlement, and Vulnerability. Research in other areas of maladaptive personality (e.g., borderline personality disorder) has made headway in engaging data collection and analytic methods that are specifically meant to examine such questions. -

Origins of Narcissism in Children
Origins of narcissism in children Eddie Brummelmana,b,1, Sander Thomaesb,c, Stefanie A. Nelemansd, Bram Orobio de Castrob, Geertjan Overbeeka, and Brad J. Bushmane,f aResearch Institute of Child Development and Education, Department of Educational Sciences, University of Amsterdam, Amsterdam 1001 NG, The Netherlands; bDepartment of Developmental Psychology, Utrecht University, Utrecht 3584 CS, The Netherlands; cCenter for Research on Self and Identity, Department of Psychology, University of Southampton, Southampton SO17 1BJ, England; dResearch Centre Adolescent Development, Department of Youth and Family, Utrecht University, Utrecht 3584 CS, The Netherlands; eDepartment of Communication and Psychology, The Ohio State University, Columbus, OH 43210-1339; and fDepartment of Communication Science, VU University Amsterdam, Amsterdam 1081 HV, The Netherlands Edited by Susan T. Fiske, Princeton University, Princeton, NJ, and approved February 12, 2015 (received for review November 7, 2014) Narcissism levels have been increasing among Western youth, and (9) and “are under a compulsion to ascribe every perfection to contribute to societal problems such as aggression and violence. the child—which sober observation would find no occasion to The origins of narcissism, however, are not well understood. Here, do” (10). Consequently, children might internalize the belief that we report, to our knowledge, the first prospective longitudinal they are special individuals who are entitled to privileges. In evidence on the origins of narcissism in children. We compared contrast, psychoanalytic theory holds that children are likely to two perspectives: social learning theory (positing that narcissism is grow up to be narcissistic when their parents lack warmth toward cultivated by parental overvaluation) and psychoanalytic theory them (11, 12). -

Two Faces of Narcissism
Two Faces of Narcissism Paul Wink Institute of Personality Assessment and Research University of California, Berkeley The present study examines the lack of strong correlations among existing self-report measures of narcissism. A principal-components analysis of 6 MMPI narcissism scales resulted in 2 orthogonal factors, 1 implying Vulnerability-Sensitivity and the other Grandiosity-Exhibitionism. Although unrelated to each other, these 2 factors were associated with such core features of narcissism as conceit, self-indulgence, and disregard of others. Despite this common core, however, Vulnerabil- ity-Sensitivity was associated with introversion, defensiveness, anxiety, and vulnerability to life's traumas, whereas Grandiosity-Exhibitionism was related to extraversion, self-assurance, exhibi- tionism, and aggression. Three alternative interpretations of these results are considered, and an argument for the distinction between covert and overt narcissism is made. The recent resurgence of interest in narcissism has led to the The NPDS (Ashby et al., 1979) is the only narcissism scale proliferation of self-report measures of the construct. Several of developed empirically by contrasting item endorsement rates the newly developed narcissism scales, including the most of diagnosed narcissists in treatment with control groups of widely researched Narcissistic Personality Inventory (NPI; other patients and individuals not in treatment. Wink and Raskin & Hall, 1979, 1981), have shown high intercorrelations. Gough (1990) have shown that the NPDS correlates positively Surprisingly, however, the NPI does not correlate with the Nar- with Serkownek's (1975) narcissism-hypersensitivity and with cissistic Personality Disorder Scale (NPDS; Ashby, Lee, & Pepper and Strong's (1958) ego-sensitivity scales, two measures Duke, 1979), another widely used measure of the construct of narcissism derived from MMPI's (Hathaway & McKinley, (Emmons, 1987; Watson, Grisham, Trotter, & Biderman, 1940) Masculinity-Femininity scale. -
How Narcissism Destroys
Rune Fardal, studerer psykologi Personlighetsforstyrrelser med hovedvekt på narsissistisk problematikk i relasjon til barn http://www.sakkyndig.com mail: [email protected] How narcissism destroys 10 Desember, 2001, Oppdatert 10.02.2014 The development of the relation between the child and the parent is extremely important. This relationship is what forms the child’s personality. In order for this development be successful for the child, some important criteria must be met. Lets look at 10 of these traits. First Aggressive impulses from the infant child, must be neutralized by the adult, so that they don’t upset the child. The adult must be able to be a “container” for the child’s frustration and needs. At this stage the child’s communication can be described as projective identification! The child try to make the adult act in a preferable way. The child project its own frustration over in the adult, and identifies with this frustration in the adults processed expression of these traits. If the outcome of this processing is, in a form the child can not handle, then the adult has failed its role as container for the child’s aggression and frustration. An example would be fear projected in an adult, the adult reaction to this projected fear decides the child’s developmental brain structure. If the adult’s reaction to the projected fear is comfort, the child develop security in the relation with the adult and others. If the adult’s reaction is insecurity and frustration, then that’s what the child will experience. That’s what is mirrored back at the child. -

Co-Narcissism Article
Co-Narcissism: How We Accommodate to Narcissistic Parents Alan Rappoport, Ph.D. Abstract dangerously inadequate and vulnerable to blame and rejection. The common use of the This article introduces the term “co- term refers to some of the ways people narcissism” to refer to the way that people defend themselves against this narcissistic accommodate to narcissistic parents. I use dynamic: a concern with one’s own physical the term narcissism here to refer to people and social image, a preoccupation with with very low self-esteem who attempt to one’s own thoughts and feelings, and a sense control others’ views of them for defensive of grandiosity. There are, however, many purposes. They are interpersonally rigid, other behaviors that can stem from easily offended, self-absorbed, blaming, and narcissistic concerns, such as immersion in find it difficult to empathize with others. Co- one’s own affairs to the exclusion of others, narcissistic people, as a result of their an inability to empathize with other’s attempts to get along with their narcissistic experience, interpersonal rigidity, an parents, work hard to please others, defer to insistence that one’s opinions and values are other’s opinions, worry about how others “right,” and a tendency to be easily offended think and feel about them, are often and take things personally. depressed or anxious, find it hard to know their own views and experience, and take the A high proportion of people in blame for interpersonal problems. They fear psychotherapy have adapted to life with being considered selfish if they act narcissistic people and, as a result, have not assertively. -

How to Deal with Co-Dependency & Control Freaks
COLORADO LAWYER ASSISTANCE PROGRAM How to Deal with Co-Dependency & “Control Freaks” “When a person attempts to control someone else’s life, it only reflects the lack of control they have on their own.” ~Daniel Chidiac The definition of co-dependency is simple enough: having emotional or psychological reliance on others. Recognizing co-dependency, however, can be far more difficult, despite the fact that it is all around us. We physically, emotionally, and mentally need relationships in order to survive. The importance of relationships is what drove us to develop language around 100,000 years ago. Healthy inter-dependence is what keeps our existence as humans going. Often times, when something is that important, we subconsciously fear losing it. It’s no surprise that for some, the importance of relationships with others triggers a fear of loss. That fear, unfortunately, can drive the belief that we have to control those relationships. When we are in situations that trigger anxiety or low self- esteem, we are particularly vulnerable to feel the need to control the people or circumstances around us. Those of us who feel anxious or fearful usually have painful, incessant mental chatter that we want to sooth. When our inner critic is constantly torturing us, and we worry about everything “under the sun” (What will people think? How is this going to work? Will it be good enough?), we look outside ourselves to find a scapegoat for our discomfort. That scapegoat takes the form of the people around us and the circumstances we find ourselves in. Rather than confronting what is going on “within” us, such as the mental chatter, we look outside ourselves and blame whatever is going on around us for our discomfort, making ourselves believe that the temper tantrum our child is throwing or the unprofessional behavior of opposing counsel is the cause of our discomfort. -
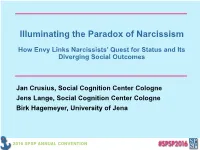
Illuminating the Paradox of Narcissism
Illuminating the Paradox of Narcissism How Envy Links Narcissists’ Quest for Status and Its Diverging Social Outcomes Jan Crusius, Social Cognition Center Cologne Jens Lange, Social Cognition Center Cologne Birk Hagemeyer, University of Jena One day when the queen asked her mirror: Mirror, mirror, on the wall, who in this land is fairest of all? It answered: You, my queen, are fair; it is true. But Snow-White is a [evil queen picture] thousand times fairer than you. The queen took fright and turned yellow and green with envy. (Grimm & Grimm, 1857/2002) Paradox of Narcissism Social Outcomes Social Potency [Jekyll & Hyde picture] Social Conflict Narcissismsimultaneously popular and unpopular at zero acquaintance (Back et al., 2013; Küfner, Nestler, & Back, 2013) Paradox of Narcissism Behavioral Patterns Social Outcomes Narcissistic Admiration Social Potency [Jekyll & Hyde picture] Narcissistic Rivalry Social Conflict Back et al. (2013) Paradox of Narcissism NARQ Behavioral Patterns Social Outcomes Grandiosity “I am great.“ Uniqueness “I show others how special I am.“ Narcissistic Admiration Social Potency Charmingness “I am very adept at dealing with other people.” Devaluation “Other people are worth nothing.“ Supremacy “I enjoy it when another person is Narcissistic Rivalry Social Conflict inferior to me.” Aggressiveness “…get annoyed when criticized.” Back et al. (2013) Paradox of Narcissism Motivation Behavioral Patterns Social Outcomes Hope for Success Narcissistic Admiration Social Potency Maintenance of a grandiose self Fear of Failure