Improving the New Mexico Indian Health Care System: Pueblo Core Values and Federal Policy by Kenneth Brian Lucero a Dissertation
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Area 11 Newsletter September 2017
Volume 10 Newsletter Issue 5 From the Chair: September 2017 Happy Fall, Everyone! Rehearsals have started Area 11 Website for most everyone, the evenings are starting to area11.handbellmusicians.org feel cooler and pumpkin spice items are every National Office Website where you look! I love this time of year! It is also the time of year that the Area 11 board Handbellmusicians.org has its only in person board meeting of the year. We will be doing that in Albuquerque Inside this issue: this coming weekend(9/15-9/17). We will be Area 11 Festival/Conference 2018 pg. 2 working on everything from making sure that the Rules of Procedure are up to date, finalizing Handbell Certification Level 1 Workshop pg. 3 the events that will be happening this year (see page 6 for a preview) Offered In Area 11 This Fall and working to get everything finalized for our Area 11 Festival Handchime Loan Placement 2017-2018 pg. 3 Conference on June 21-24, 2018. Please see info on the next page about our lead clinician and class teachers! There is also a great Membership Article by Lorrie Hart pg. 4 informational article about the Festival/Conference logo. Thoughts from a First Time Attendee We have a bunch of events coming up in Area 11 before the Festival at National Seminar pg. 5 conference. There are a few Back to Bells sessions scheduled in the area over the next few weeks. We are also hosting a Level 1 Upcoming Events pg. 6 Handbell Certification Workshop this fall and the deadline to register is Back to Bells Workshops in Area 11 pg. -
Atlas of Historic NM Maps Online at Atlas.Nmhum.Org
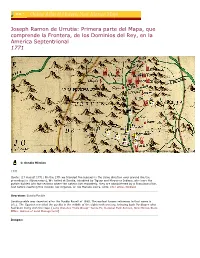
Joseph Ramon de Urrutia: Primera parte del Mapa, que comprende la Frontera, de los Dominios del Rey, en la America Septentrional 1771 9 8 7 5 6 4 2 3 1 Library of Congress Geography and Map Division - Terms of Use 1: Sandia Mission 1771 Quote: (17 August 1771) On the 17th we traveled five leagues in the same direction over ground like the preceding [to Albuquerque]. We halted at Sandia, inhabited by Tiguas and Moquinos Indians, who have the pueblo divided into two sections where the nations live separately. they are administered by a Franciscan friar. Just before reaching this mission Los Organos, or Los Mansos sierra, ends. [de Lafora, Nicolás] Overview: Sandia Pueblo Sandia pueblo was deserted after the Pueblo Revolt of 1680. The earliest known reference to that name is 1611. The Spanish resettled the pueblo in the middle of the eighteenth century, bringing back Puebloans who had been living with the Hopi. [Long Distance Trails Group--Santa Fe, National Park Service, New Mexico State Office, Bureau of Land Management] Images: Sandia Mountains, the Rio Grande near Bernalillo, foreground, ruins of Tur-jui-ai 2: Bernalillo Lafora describes Bernalillo as a group of ranches, but Urrutia draws it as a city or town. Quote: (18 August 1771) On the 18th we traveled eight leagues inthe same direction over ground like the preceding. On both side of the river there are several small ranches called Bernalillo. [de Lafora, Nicolás] Overview: Bernalillo Bernalillo was a heavily populated district when visited by sixteenth-century Spaniards. It continued that tradition as a Spanish community, though it was not generally visited by the bulk of travelers who were across the river on the east bank. -

Ethnographic Assessment
Santa Fe Ski Basin Proposed Expansion Ethnographic Assessment Item Type Report Authors Evans, Michael; Stoffle, Richard W.; Krause, Elizabeth Publisher Bureau of Applied Research in Anthropology University of Arizona Download date 28/09/2021 13:20:12 Link to Item http://hdl.handle.net/10150/271443 -OFFICE COPY - DO NOT REMOVE Santa Fe Ski Basin ProposedExpansion Ethnographic Assessment Final Draft Report Submitted by Michael J. Evans Richard W. Stoffie Elizabeth L. Krause Bureau of Applied Research in Anthropology University of Arizona Tucson, Arizona Submitted to Sno- Engineering Bellevue, Washington June 1, 1993 Santa Fe Ski Basin Proposed Expansion Ethnographic Assessment Final Draft Report Submitted by Michael J. Evans Richard W. Stoffle Elizabeth L. Krause Bureau of Applied Research in Anthropology University of Arizona Tucson, Arizona Submitted to Sno- Engineering Bellevue, Washington June 1, 1993 Table of Contents Chapter I: Introduction 1 Purpose of Study 1 Project Participants 1 Relevant Federal Legislation and Regulatory Policies 2 National Environmental Policy Act 3 Early Historic Preservation Legislation 3 Archaeological Resources Protection Act 3 American Indian Religious Freedom Act 4 National Historic Preservation Act 4 Methodology 6 Native American Participation 6 Site Visits 7 Chapter II: Pueblo Cultural Resources 9 Pueblo Prehistory and History in the Study Area 9 Nambe and Tesuque Pueblos 11 Pueblo Cultural Resource Use in the Study Area 11 Contemporary Pueblo Cultural Resource Concerns 13 Types of Cultural Resource -

1779 Miera Domãnguez Galisteo
Plano de la Provincia Interna de el Nuebo Mexico 1779 1 3 7 2 4 6 5 11 8 10 9 Library of Congress Geography and Map Division - Terms of Use 1: Nuestra Señora de los Angeles de Pecos 1776 Father Domínguez paints a portrait of Pecos towards the end of its long decline. Biship Tamarón had counted twice as many inhabitants not 20 years before, and the drop in population may have had as much to do with drought and hunger as with the raiding Comanches. Disease also played a part at decimating Pecos, with the smallpox carrying off hundreds of residents. Quote: (1776) The parish books date from the year 1727. Their writs record 200 leaves, but this number does not exist now. There is little missing from the book of Baptisms and the entries seem to be complete. The others have scarcely twenty leaves each, and their entries have been visited frequently by the mice. I remitted these to the archive, which is at the mission of Our Father Santo Domingo (as has been said before.) Three new ones from the supply that came from teh Province remain in Santa Fe so that the mission father there may keep the records in the interval until there is a missionary at Pecos, whose Indians are baptized and married in said villa. With regard to burials, if an Indian dies, the others perform the offices, etc.. Although there is no father [priest], they still know that the children must go to the church daily to recite the catechism with the fiscal. -

Fort Union National Monument Ethnographic Overview and Assessment
Fort Union National Monument Ethnographic Overview and Assessment Report Prepared By: Dr. Joseph P. Sánchez Dr. Jerry L. Gurulé Larry V. Larrichio Larry D. Miller March 2006 TABLE OF CONTENTS LIST OF ILLUSTRATIONS .............................................................................................................i FORT UNION NATIONAL MONUMENT....................................................................................1 INTRODUCTION........................................................................................................................... 1 METHODOLOGY.......................................................................................................................... 1 PART I..................................................................................................................................................4 INTRODUCTION........................................................................................................................... 4 HISPANIC CONTRIBUTIONS TO THE NEW POLITICAL, SOCIAL AND CULTURAL ORDER ......... 7 AUXILIARY SERVICES: HISPANICS AS GUIDES, SPIES, TRAILERS, AND PACKERS ................. 12 HISPANICS AS COMANCHEROS AND CIBOLEROS..................................................................... 14 LABOR AT FORT UNION: HISPANICS CONTRIBUTIONS TO THE TRADES ................................ 17 HISPANIC AGRICULTURAL PRACTICES AND THE NEEDS AT FORT UNION ............................. 18 HISPANICS AND OTHERS AS COMMERCIAL SUPPLIERS ......................................................... -

ZIA PUEBLO and the Sacred Sun Symbol in the Public Domain
ZIA PUEBLO and the Sacred Sun Symbol in the Public Domain June L. Lorenzo, J.D. & PhD Indigenous World Association and International Indian Treaty Council WIPO/IGC 38, Geneva, Switzerland December 10, 2018 Presentation by Gov. Anthony Delgarito Historical Facts about Zia CONTINUOUSLY INHABITED SINCE 1200 AD 1583 – First Contact with Spain 1680 – Pueblo Revolt 1689 - Battle with Gov. Cruzate- 600 killed, 70 enslaved Population: est. 700 at contact to 120 in 1892 disease and warfare Land base: 27.3 square miles (7.070 hectares) Survived Spanish, Mexican and American colonialism ZIA SUN SYMBOL TAKEN FROM ZIA Late 1800’s – Sacred pot/ water jar stolen from Zia. (Matilda Stevenson?) Reappeared in 1920 in Santa Fe for state sym Repatriated to Zia in 2000- 02 Violation of Zia Indigenous Law Symbol widely dispursed 1925- DAR Contest for state flag design Dr. Harry Mera - had seen pottery, used sun symbol for his entry Won contest; became N.M. state flag Without permission of Zia people GAPS IN DOMESTIC LAW • State of N.M .(appropriator) use of Zia sun symbol protected but Pueblo of Zia’s use of their own symbol is not • Section 2(b) of the Lanham Act: the USPTO must refuse registration of a mark if it “[c]onsists of or comprises the flag or coat of arms or other insignia of the United States, or of any State or municipality, or of any foreign nation.” • 15 U.S.C. § 1052(b) (2006). • Theory:discourage commercial uses of insignia that represent any nation or state, because such insignia are considered “culturally sacred.” • But many loopholes– -

1758 Miera Rio Abajo
Map which Don Francisco Antonio Marín del Valle, Governor and Captain General of this kingdom of New Mexico, ordered drawn 1758 8 10 11 7 9 12 6 5 4 15 13 3 14 2 1 National Park Service, Washington, D.C. - Terms of Use 1: Bethem 1760 Quote: (19 May 1760) On the nineteenth we passed the house they call Colorada, also in ruins, and from that point on we began to see pens of ewes, corrals, and small houses, for there is good pasturage. On this same day the houses of the settlement of Belen on the other side of the river came into view, and from there on great poplar groves begin to cover the countryside. Here we were received by the alcade of Tome with the citizens of his town, of Belen, and of Isleta. The last two are on the other side of the river. We reached Tome at ten and made a stop there. [Tamarón y Romeral, Pedro] Overview: Belén Belén was constructed on the west bank of the Río Grande. Colonial travelers saw it from their camps across the river while later users of the west bank road stopped within the town. Given that most colonial traffic passed along the east bank of the Río Grande, the most used caravan paraje would have been opposite the town of Belén. [Long Distance Trails Group--Santa Fe, National Park Service, New Mexico State Office, Bureau of Land Management] 2: Fonclara 1760 During this period, the village of Tomé was renamed Fuenclara (or Fonclara) on the maps, in honor of the Marquis de Fuenclara, the current Viceroy of New Spain. -

State Legislature Primer
New Mexico Legislature Welcome to the New Mexico State Capitol! I am excited about your interest in the New Mexico Legislature and our State Capitol! Please take this opportunity to tour the buildings and grounds, and if you are here during a legislative session, I encourage you to observe floor sessions or committee meetings. Enjoy the architecture and art of the Capitol, which reflect New Mexico's unique culture. The vast art collection is managed by the Capitol Art Foundation and includes works displayed in the Capitol, the Capitol North, the walkway that connects the two and the surrounding grounds. The 112 members of the New Mexico Legislature occupy the building during annual legislative sessions and during the interim to attend committee meetings. The Capitol, also known as the Roundhouse, and the Capitol North are also home to the Office of the Governor, the Office of the Lieutenant Governor, the Office of the Secretary of State, the House of Representatives and the Senate. Understanding the legislative process is important, and this booklet is an effort to make your visit more enjoyable. Sincerely, YOUR STATE LEGISLATOR The Roundhouse New Mexico has the oldest, as well as one of the newest, state capitols in the United States. The oldest is the Palace of the Governors in Santa Fe, built in 1610. The newest is the current Capitol, which was dedicated in December 1966 and underwent extensive remodeling in 1991. Built in traditional Territorial Style and resembling the Zia symbol, the building consists of four levels. The House and Senate chambers, legislative leadership offices and some staff offices are located on the first level. -

THE CASE of the ZIA: LOOKING BEYOND TRADEMARK LAW to PROTECT SACRED SYMBOLS Stephanie B
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Yale Law School Legal Scholarship Repository THE CASE OF THE ZIA: LOOKING BEYOND TRADEMARK LAW TO PROTECT SACRED SYMBOLS Stephanie B. Turner* Abstract This Article tells the story of a tribe’s fight, over the past two decades, to reclaim its sacred symbol. Members of the Zia tribe, a Native American group located near Albuquerque, New Mexico, have been using their sacred sun symbol in religious ceremonies since 1200 C.E. Today, the symbol appears on the New Mexico state flag, letterhead, and license plate, and on numerous commercial products, including motorcycles and portable toilets. The tribe claims that the state appropriated the symbol without permission in 1925, and that the continued use of the symbol by various parties dilutes its sacred meaning and disparages the Zia people. This Article considers the harms the tribe faces when outsiders appropriate its symbol and the possible solutions within current trademark law. Ultimately, this Article illustrates that, for the Zia, non-legal measures have been more effective than legal ones. The case of the Zia thus suggests that indigenous groups should look beyond trademark law in the fight to protect their sacred symbols. *Yale Law School, J.D. expected 2012; Barnard College, Columbia University, B.A. 2009. Thank you to Professor Carol Rose for supervising this project; to the editors of the Chicago-Kent Journal of Intellectual Property for their feedback throughout the editorial process; and to Patrick Moroney and my family for their enduring support. -

1745 Menchero Rio Arriba
Menchero: Mapa del Reino de Nuevo Mexico 1745 10 3 11 9 12 8 20 13 7 6 14 5 18 19 2 4 1 22 21 17 15 16 Library of Congress, Geography and Maps Division - Terms of Use 1: Villa de Santa Fee la Capital 1744 Quote: (1744) The capital villa of Santa Fé was reëstablished in the year 1682[sic, should be 1692] by the religious and the governor. It is more than six hundred leagues from this court of Mexico, the distance for which his Majesty pays the couriers. It lies toward the north, and is situated on a slope of high land, from which rises a crystalline river full of trout, which although small, are very savory and as good as those of our Spain. This river has its origin in a lake that lies on the summit, or crown, of this land, and its course runs through the said villa, which is located in 37 degrees. It has the same climate as our Spain (that is, in New Castile) and rains at the same times; the spring is mild and the summer extremely hot, so much so that cotton is sown and gathered the same as in tropical lands; it produces in abundance savory melons, watermelons, cucumbers, and all the fruits of the trees of Spain; the autumn is cold and the winter severe with cold, droughts, and snow. It has now about one hundred and twenty-seven Spanish families, among whom its holy title of Santa Fé is preserved and augmented. It has but few Indians because they do not like to live with the Spaniards. -

Fort Union National Monument Ethnographic Overview and Assessment
Fort Union National Monument Ethnographic Overview and Assessment Report Prepared By: Dr. Joseph P. Sánchez Dr. Jerry L. Gurulé Larry V. Larrichio Larry D. Miller March 2006 TABLE OF CONTENTS LIST OF ILLUSTRATIONS .............................................................................................................i FORT UNION NATIONAL MONUMENT....................................................................................1 INTRODUCTION........................................................................................................................... 1 METHODOLOGY.......................................................................................................................... 1 PART I..................................................................................................................................................4 INTRODUCTION........................................................................................................................... 4 HISPANIC CONTRIBUTIONS TO THE NEW POLITICAL, SOCIAL AND CULTURAL ORDER ......... 7 AUXILIARY SERVICES: HISPANICS AS GUIDES, SPIES, TRAILERS, AND PACKERS ................. 12 HISPANICS AS COMANCHEROS AND CIBOLEROS..................................................................... 14 LABOR AT FORT UNION: HISPANICS CONTRIBUTIONS TO THE TRADES ................................ 17 HISPANIC AGRICULTURAL PRACTICES AND THE NEEDS AT FORT UNION ............................. 18 HISPANICS AND OTHERS AS COMMERCIAL SUPPLIERS ......................................................... -

1844 Gregg Rio Arriba
Josiah Gregg: Map of the Indian Territory, Northern Texas and New Mexico, Showing the Great Western Prairies 1844 1 5 2 6 7 4 3 9 12 8 11 10 Rumsey Collection Image No. 2351001 - Terms of Use 13 1: Josiah Gregg 1831-1840 Josiah Gregg was one of the first Americans to paint a comprehensive picture both of the details of trading to Mexico on the Santa Fe Trail, and of the exotic natural history, customs, and cultures of New Mexico. He traded between 1831-1840, and in 1844 published Commerce of the Prairies, including this map. Images: Josiah Gregg 2: Rabbit Ear Mounds 1821-1844 Quote: (05 July 1838) The next day's march brought us in front of the Rabbit-Ear Mounds, which might now be seen at a distance of eight or ten miles south of us, and which before the present track was established, served as a guide to travellers. The first caravan of wagons that crossed these plains, passed on the south side of these mounds, having abandoned our present route at the ' Cold Spring,' where we encamped on the night of the 1st of July. Although the route we were travelling swerves somewhat too much to the north, that pursued by the early caravans as stated above, made still a greater circuit to the south, and was by far the most inconvenient. As we were proceeding on our march, we observed a horseman approaching, who excited at first considerable curiosity. His picturesque costume, and peculiarity of deportment, however, soon showed him to be a Mexican Cibolero or buffalo-hunter.