The Emotional Projection Test As an Instrument to Differentiate Affective
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Personality Assessment Techniques Any Psychological Tests Is Useful in That It Achieves Two Basic Goals 1. It Accurately (Validi
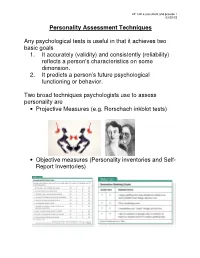
LP 13D assessment and pseudo 1 03/29/15 Personality Assessment Techniques Any psychological tests is useful in that it achieves two basic goals 1. It accurately (validity) and consistently (reliability) reflects a person’s characteristics on some dimension. 2. It predicts a person’s future psychological functioning or behavior. Two broad techniques psychologists use to assess personality are • Projective Measures (e.g. Rorschach inkblot tests) • Objective measures (Personality inventories and Self- Report Inventories) LP 13D assessment and pseudo 2 03/29/15 Personality Assessment Projective measures: Personality tests that examine unconscious processes by having people interpret ambiguous stimuli ( page 580 ). Examples: Rorschach Inkblot Test Thematic Apperception Test Projective tests strengths: • Provides a wealth of qualitative information that can be followed up if used for psychotherapy Projective test weaknesses: • The testing situation and examiner’s behavior affects the response • The scoring on the test is subjective and inconsistent among scorers • Test-retest inconsistencies are common • Poor predictors of future behavior. LP 13D assessment and pseudo 3 03/29/15 Personality Assessment: Objective Measures Objective Measures: Relatively direct assessments of personality, usually based on information gathered though self-report questionnaires or observer ratings. (page 581 ). Examples: Sensation-seeking, MMPI, CPI, 16PF, Just World Belief Scale, Optimism-Pessimism Scale LP 13D assessment and pseudo 4 03/29/15 Personality Assessment: Objective Measures Objective measures strengths: • Objectively scored and compared to standardized norms collected on large groups of people (they receive the same instructions). • Validity of self-report inventories is greater than projective tests. Objective measures weaknesses • People are able to fake socially desirable responses • Some people are prone to pick “the first answer” • Some personality inventories are long and tedious which lends to the problem listed above. -

Projective Tests in Human Resource Management and Hiring Process: a Challenge and a Boon
The International Journal of Indian Psychology ISSN 2348-5396 (e) | ISSN: 2349-3429 (p) Volume 7, Issue 4,DIP: 18.01.027/20190704 DOI: 10.25215/0704.027 http://www.ijip.in | October- December, 2019 Research Paper Projective tests in human resource management and hiring process: a challenge and a boon Janetius S.T1*, Pooja Varma2, Shilpa S3 ABSTRACT Industrial and organizational psychology plays a major role in human resource management (HRM). From the selection of a candidate to promotion, psychology is applied, mainly in the form of testing and assessment. Even though a lot of care has been taken in selecting the right candidate for the right job, many organizations realize hiring mistakes after some time. This is mainly because psychological measurement tools can be easily manipulated by candidates; also, social desirability affects the responses. Personal interviews fail to gauge the right intention of candidates and the inner dynamics remains hidden, making the selection process hard. The objective of this paper is to propose projective tests as a tool to overcome some of the common problems faced by human resource personnel in the hiring process. Keywords: Projective Tests, Psychological Tests, Selection and Hiring Process, Psychology and HRM, Organizational psychology. People are fundamental to any organization. Psychology, to be specific, industrial and organizational psychology, has the potency to add the efficiency and effectiveness of any business, whether it is simple or complex, local or professional, by increasing the ability to understand human persons at workplaces in a much better way; thus, it attempts towards satisfaction and fulfillment to both the employer and employee. -

Content Analysis of the Holtzman Inkblot Test with Regard to the Projection of Hostility
Fort Hays State University FHSU Scholars Repository Master's Theses Graduate School Spring 1962 Content Analysis of the Holtzman Inkblot Test with Regard to the Projection of Hostility Roberta B. Harkness Fort Hays Kansas State College Follow this and additional works at: https://scholars.fhsu.edu/theses Part of the Psychology Commons Recommended Citation Harkness, Roberta B., "Content Analysis of the Holtzman Inkblot Test with Regard to the Projection of Hostility" (1962). Master's Theses. 750. https://scholars.fhsu.edu/theses/750 This Thesis is brought to you for free and open access by the Graduate School at FHSU Scholars Repository. It has been accepted for inclusion in Master's Theses by an authorized administrator of FHSU Scholars Repository. CONTENT ANALYSIS OF THE HOLTZMAN INKBLOT TEST WITH REGARD TO THE PROJECTION OF HOSTILITY being A Thesis Presented to the Graduate Faculty of the Fort Hays Kansas State College in Partial Fulfillment of the Requirements for the Degree of Master of Science by Roberta B. Harkness, A. B. Fort Hays Kansas State College Approved tJ-~·~/ f: /'.?,c;cZc Major Profe ssor Approved~ . Cha· an, Graduate Council ACKNOWLEDGMENT Appreciation is expressed to Dr. David Proctor for his patient guidance during the months that were spent in com- pleting this thesis. A sense of obligation and gratitude is further felt toward Dr. Stanley Mahoney , Dr . William Gwynn , and Dr. Joel Moss who served on my graduate corrnni t tee . The family of a student whose thesis has been a long-time project deserves recognition. My husband and daughters ig- nored the inconveniences while they encouraged and hect or ed me into completing it. -

The Thematic Apperception Test: the Relationship Between
THE THEMATIC APPERCEPTION TEST: THE RELATIONSHIP BETWEEN SCORED FANTASY AGGRESSION AND AGGRESSIVE BEHAVIOR Joanne Madeline Fabrick, BA Thesis Prepared for the Degree of MASTER OF ARTS UNIVERSITY OF NORTH TEXAS December 2000 APPROVED: Sharon Rae Jenkins, Major Professor Vicki Campbell, Committee Member C. Edward Watkins, Committee Member Ernest Harrell, Chair of the Department of Psychology C. Neal Tate, Dean of the Robert B. Toulouse School of Graduate Studies Fabrick, Joanne Madeline, The Thematic Apperception Test: The relationship between scored fanasy aggression and aggressive behavior. Master of Arts (Counseling Psychology), December 2000. 61 pp., 10 tables, 31 references. This study attempted to determine the relationship between fantasy aggression and behavioral aggression, and whether fantasy aggression measured by the Thematic Apperception Test is related to behavioral aggression. Participant TAT protocols from psychology clinic files were scored for fantasy aggression, and these scores were correlated with self-reported presence or absence of behavioral aggression. The scoring system used was a blend of popular aggression scales used in the 1960s and newer theory. Other variables that were examined were story length and gender in relation to the measured amount of fantasy and behavioral aggression. Copyright 2000 By Joanne Madeline Fabrick ii ACKNOWLEDGMENTS I would like to acknowledge the work of the clinic research team in collecting and preparing the archival data used in this study. Joe Davis, Kitty Roberts, Amy Butterfield, Shaneka Morris, Amanda Phillips, Lisa Black, and Veronica Navarette-Vivero put forth time and energy to make this information accessible for research. iii TABLE OF CONTENTS Page ACKNOWLEDGMENTS............................................................................................... iii LIST OF TABLES .......................................................................................................... v Chapter 1. -

Running Head: a COMPARISON of PERSONALITY TESTS 1 A
Running head: A COMPARISON OF PERSONALITY TESTS 1 A Comparison of TAT and NEO-FFI Personality Tests: TAT and NEO-FFI Commented [CE1]: Please add all the relevant details to this title page, including your name, the subject name and date of submission. If you are required to submit and abstract, it should be presented on a separate page before the body of your paper, in one unindented paragraph. Commented [CE2]: Please check the changes I made to this title, as TAT Personality Test does not make sense. A COMPARISON OF PERSONALITY TESTS 2 A Comparison of TAT and NEO-FFI Personality Tests: TAT and NEO-FFI Personality tests have long been used in psychology in order to determine particular traits in individuals and to assigning personality types for the purpose ofto predicting their behaviour and temperament of those individuals. There are two main types Commented [CE3]: Please note that you only need one space after a full stop, as you are submitting this paper to an Australian university. You only need two spaces if you are submitting a paper of personality tests that may be administered, the projective test and the structured test, with to a journal that follows APA Style guidelines strictly. many individual tests that fall under either of the two categories. This paper will definediscusses the two main types of the personality tests—projective and structured— and examines their differences., Specifically, based on a comparison ofcompare and contrast the relative merits and demerits of the tThematic aApperception tTest (TAT) and the Neo F– Five- Factor Inventory (NEO-FFI), using positive and negative factors, as well as validity and reliability, this paper aims to determine which test is more which will lead to the recommendation of useful, valid and reliablea test based on these merits. -

Chapter 2 Teachers 1) Which of the Following Is Not a Method of Assessment? A) Structured Clinical Interview B) Personality
Chapter 2 Teachers 1) Which of the following is not a method of assessment? a) Structured clinical interview b) Personality inventories c) Projective tests d) Thalamic tests (A) 2) Which of the following are not neural imaging technique? a) ECG (A) b) FMRI c) MRI d) PET 3) Rorschach’s projective tests are designed to measure: a) Unconcious intentions (A) b) Dreams c) Conscious desires d) Brain size 4) Which of the following are not measured by psychological tests? a) Intelligence b) Cognitive deficits c) Neurological deficits d) Unconscious intentions (A) 5) Which of the following is not a projective test? a) Rorschach’s ink blot test b) Thematic apperception test c) Sentence completion test d) Word association test (A) 6) Which of the following is not true of IQ tests? a) High test re-test reliability b) High internal consistency c) Good validity d) Good predictor of behaviour (A) 7) Validity scales in the MMPI profile are particularly useful because they: a) Allow measurement of false information (A) b) Allow the clinician to know what the patient is thinking c) Insures the clinician will get the same test result again d) Allows the clinician to predict clients future behaviour 8) Specific trait inventories assess: a) Characteristics across a range of different traits and domains b) Functioning in one specific area c) Functioning in a specific psychopathology d) All of the above (A) 9) The popularity of projective tests has declined over the years because: a) They reveal information that is relevant to psychodynamic approaches b) Test -
Reliability and Validity of the Thematic Apperception Test Scored by the Discomfort-Relief Quotient
Central Washington University ScholarWorks@CWU All Master's Theses Master's Theses 1960 Reliability and Validity of the Thematic Apperception Test Scored by the Discomfort-Relief Quotient Donald W. Culbertson Central Washington University Follow this and additional works at: https://digitalcommons.cwu.edu/etd Part of the Educational Methods Commons, and the Educational Psychology Commons Recommended Citation Culbertson, Donald W., "Reliability and Validity of the Thematic Apperception Test Scored by the Discomfort-Relief Quotient" (1960). All Master's Theses. 242. https://digitalcommons.cwu.edu/etd/242 This Thesis is brought to you for free and open access by the Master's Theses at ScholarWorks@CWU. It has been accepted for inclusion in All Master's Theses by an authorized administrator of ScholarWorks@CWU. For more information, please contact [email protected]. RELIABILITY AND VALIDITY OF THE THEMATIC APPERCEPTION TEST SCORED BY THE DISCOMFORT-RELIEF QUOTIENT .' A Thesis Presented to the Graduate Faculty Central Washington College of Education In Partial Fulfillment of the Requirements for the Degree Master of Education by Donald W. Culbertson December, 1960 LD 5771.I C 9 G ?r- SPS"Cll\'!: GIJl.il.Cll.Cli 106973 APPROVED FOR THE GRADUATE FACULTY Eldon E. Jacobsen, COMMITTEE CHAIRMAN Dean Stinson Maurice L. Pettit ACKNOWLEDGMENTS Grateful acknowledgment is extended to Dr. Eldon E. Jacobsen for his advice and encouragement in directing the writing of this paper, and to Dr, Maurice L, Pettit and to Dr, Dean Stinson for their helpful suggestions, Further acknowledgment is extended to Dr, E, E. Samuelson, Dean of Students; Dr, Roy F. Ruebel, Dean of Graduate Studies; Dr, Ralph Gustafson, Director of Student Teaching; and Mr. -

Rorschach Inkblot Test: an Overview on Current Status
The International Journal of Indian Psychology ISSN 2348-5396 (Online) | ISSN: 2349-3429 (Print) Volume 8, Issue 4, Oct- Dec, 2020 DIP: 18.01.075/20200804, DOI: 10.25215/0804.075 http://www.ijip.in Research Paper Rorschach Inkblot Test: an overview on current status Anwesha Mondal1*, Manish Kumar2 ABSTRACT The Rorschach Inkblot Test has the dubious distinction of being simultaneously the most cherished and the most criticized of all psychological assessment tools. Till date on one hand it is held in great esteem by many for its ability to access intrapsychic material, whereas others consider it to be a prime example of unscientific psychological assessment. However, the Rorschach Inkblot Test is extensively used since it is found to be a tool to unearth the deep-rooted emotional conflicts. Despite limitations and various drawbacks Rorschach Inkblot Test is widely and rigorously used in different clinical settings and has considerable potential to contribute in the field of psychology in the future years. Hence, an attempt has been made to understand the current status of Rorschach Inkblot Test. Keywords: Rorschach, current, status ersonality refers to the patterns of thoughts, feelings, social adjustments and behaviours consistently exhibited by an individual over time that strongly influence an individual’s P expectations, self-perceptions, values, attitudes, and predicts reactions to people, problems and stress. Personality is referred to as the complexity of psychological systems that contribute to unity and continuity in the individual’s conduct and experience, both as it is expressed and as it is perceived by that individual and others. In the 1930s personality psychology emerged as a discrete field of study where personality assessment received its important impetus. -

Projective Assessment and School Psychology: Contemporary Validity Issues and Implications for Practice
The California School Psychologist, Vol. 11, pp. 73-84, 2006 Copyright 2006 California Association of School Psychologists 73 Projective Assessment and School Psychology: Contemporary Validity Issues and Implications for Practice David N. Miller and Amanda B. Nickerson University at Albany, State University of New York Projective techniques continue to be widely used by school psychologists despite frequent criti- cisms of their use. This article reviews contemporary validity issues in the use of projective techniques with children and adolescents, including incremental validity, treatment validity, and problems associated with professional judgment and experience. A discussion of these issues and their implications for school-based projective assessment is provided, along with recommenda- tions for the appropriate use of projective techniques with children and youth within a problem- solving framework. A central component of contemporary school psychology training and practice is data-based deci- sion making and accountability (Ysseldyke et al., 2006). Consistently recommended practices for con- ducting reliable, valid, and comprehensive assessments of child and adolescent emotional and behav- ioral problems involve gathering various sources of assessment data from multiple informants (e.g., parents, teachers, students) across different settings (McConaughy & Ritter, 2002). In addition, assess- ments should not only estimate current student functioning by defining problems, needs, and assets, but should also be linked directly to the development and evaluation of interventions (Ysseldyke et al.). Behavioral assessment methods (e.g., interviews, observations, informant-report measures) are generally viewed by school psychologists as more useful (Cheramie, Griffin, & Morgan, 2000) and acceptable (Eckert, Hintze, & Shapiro, 1997) than traditional assessment procedures such as projec- tive techniques for assessing students with suspected emotional and/or behavioral problems. -

Unit 3 Psychological Assessment
UNIT 3 PSYCHOLOGICAL ASSESSMENT Structure 3.1 Introduction 3.2 Learning Objectives 3.3 Objectives of Psychological Assessment 3.4 Types of Psychological Test 3.4.1 Neuro-cognitive Assessment 3.4.2 Assessment of Personality and Psychopathology 3.4.2.1 Rating Scales 3.4.2.2 Questionnaires 3.4.2.3 Projective Tests 3.4.2.4 Semi-projective Tests 3.4.2.5 Innovative Approaches to Assessment 3.5 Psychological Assessment of Children 3.6 Ethics Aspects in Psychological Testing 3.7 Problems in Administration of Psychological Tests 3.8 Let Us Sum Up 3.9 Answers to Check Your Progress Exercises 3.10 Unit End Questions 3.11 References and Suggested Readings 3.1 INTRODUCTION Psychological tests help to identify mental disorders in a standardized, reliable and valid manner. With the use of variety of tests, a diagnosis can be formulated. Psychological assessment refers to the process involved in collecting information about persons and using it to make important predictions and inferences about his cognition and personality. Psychological tests are means of assessing psychological characteristics. A psychological test is essentially an objective and standardized measure of a sample of behaviour. Psychological tests are like tests in any other science, as observations are made on a small but carefully chosen sample of an individual’s behaviour. In this respect, the psychologist proceeds in much the same way as the biochemist that tests a patient’s blood. The diagnostic or predictive value of psychological tests depends on the degree to which it serves as an indicator of a relatively broad and significant area of behaviour. -
An Exploration of the Use of Projective Techniques by Educational Psychologists in the UK
An exploration of the use of projective techniques by educational psychologists in the UK A thesis submitted to The University of Manchester for the degree of Doctorate in Educational and Child Psychology in the Faculty of Humanities 2017 RACHAEL KING School of Environment, Education and Development 1 List of Contents List of Tables ...........................................................................................................5 List of Figures ..........................................................................................................6 List of Appendices ..................................................................................................7 List of Acronyms .....................................................................................................8 2 Abstract ....................................................................................................................9 Declaration .............................................................................................................10 Copyright Statement .............................................................................................11 Chapter 1: Introduction ....................................................................................12-15 Chapter 2: Literature Review ...........................................................................16-37 2.1 Chapter overview ............................................................................................16 2.2 Literature search ........................................................................................16-18 -

Holtzman Inkblot Technique
VII Objective Scoring of Projective Tests WAYNE H. HOLTZMAN The University of Texas _CVER SINCE L. K. Frank's first use of the term "projective method" in 1939 (15), there has been a rapid mushrooming of techniques for encouraging an individual to reveal aspects of his personality by the way in which he perceives, organ- izes, or relates to potentially affect-laden, ambiguous stimuli. Stem- ming largely from psychoanalytic theory, such projective techniques range all the way from free association in relatively unstructured situations to rather highly structured, formalized devices such as the Thematic Apperception Test. Before considering the problems of quantification and objective scoring, it might be instructive to examine closely the assumptions implicit in the projective method as contrasted to those underlying psychometric tests and measure- ment theory. PROJECTIVE COMPARED WITH PSYCHOMETRIC METHODS Unlike the standardized aptitude test, the projective approach deals with the idiomatic expression of the individual as revealed in the context of his needs, fears, strivings, and ego-defensive behavior. As Frank has so aptly stated, "The essential feature of a projective technique is that it evokes from the subject what is, in various ways, expressive of his private world and personality process." (16, p. 47). 119 120 OBJECTIVE APPROACHES TO PERSONALITY ASSESSMENT Given any projective technique where the subject is offered a wide latitude in which to reveal himself, the particular sample of re- sponses obtained is assumed to reflect