Market Failure in Kidney Exchange†
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Adam Smith 1723 – 1790 He Describes the General Harmony Of
Adam Smith 1723 – 1790 He describes the general harmony of human motives and activities under a beneficent Providence, and the general theme of “the invisible hand” promoting the harmony of interests. The invisible hand: There are two important features of Smith’s concept of the “invisible hand”. First, Smith was not advocating a social policy (that people should act in their own self interest), but rather was describing an observed economic reality (that people do act in their own interest). Second, Smith was not claiming that all self-interest has beneficial effects on the community. He did not argue that self-interest is always good; he merely argued against the view that self- interest is necessarily bad. It is worth noting that, upon his death, Smith left much of his personal wealth to churches and charities. On another level, though, the “invisible hand” refers to the ability of the market to correct for seemingly disastrous situations with no intervention on the part of government or other organizations (although Smith did not, himself, use the term with this meaning in mind). For example, Smith says, if a product shortage were to occur, that product’s price in the market would rise, creating incentive for its production and a reduction in its consumption, eventually curing the shortage. The increased competition among manufacturers and increased supply would also lower the price of the product to its production cost plus a small profit, the “natural price.” Smith believed that while human motives are often selfish and greedy, the competition in the free market would tend to benefit society as a whole anyway. -
1 Three Essential Questions of Production
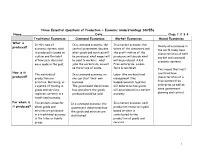
Three Essential Questions of Production ~ Economic Understandings SS7E5a Name_______________________________________Date__________________________________ Class 1 2 3 4 Traditional Economies Command Economies Market Economies Mixed Economies What is In this type of In a command economy, the In a market economy, the Nearly all economies in produced? economic system, what central government decides wants of the consumers and the world today have is produced is based on what goods and services will the profit motive of the characteristics of both custom and the habit be produced, what wages will producers will decide what market and command of how such decisions be paid to workers, what will be produced. A.K.A. economic systems. were made in the past. jobs the workers do, as well Free-enterprise, Laisse- as the prices of goods. faire & capitalism. This means that most How is it The methods of In a command economy, no Labor (the workers) and countries have produced? production are one can start their own management (the characteristics of a primitive. Bartering, or business. bosses/owners) together free market/free a system of trading in The government determines will determine how goods enterprise as well as goods and services, how and where the goods will be produced in a market some government replaces currency in a produced would be sold. economy. planning and control. traditional economy. For whom is The primary group for In a command economy, the In a market economy, each it produced? whom goods and government determines how production resource is paid services are produced the goods and services are based on what is in a traditional economy distributed. -

The Stock Market and the Economy
BARRY BOSWORTH Brookings Institution The Stock Market and the Economy THE STOCKMARKET decline of 1973-74 marked the longest and steepest fall in corporate-stockprices since the depressionof the 1930s.The loss of stockholderwealth in marketprices amounted to $525 billion, or 43 per- cent.'The magnitudeof this declinein stockvalues, in conjunctionwith the subsequentcollapse of aggregatedemand in 1974-75, has sparkeda re- newed discussionof the role of the stock marketin businesscycles. The debate-as is so frequentlythe case-is not new to economics.Several sig- nificantcontributions recently made at both the conceptualand empirical levels seem, however,to justify a reexaminationof the issues. The disputeabout the import of changesin the stock marketrevolves around their causal role in economicfluctuation: Are they a source of variationin aggregatedemand? Does the causationrun solely in the op- posite direction?Or do the levels of economicactivity and of stock prices simplyrespond similarly to other,more basic, economic forces, with no di- rect causal link betweenthe two? This third interpretationis consistent with a view that the stock marketreflects investors' attempts to forecast economictrends. The fact that movementsin stock prices foretellmajor Note: I am gratefulto LeonardHerk for researchaid in writingthis article.Members of the Brookingspanel offeredvaluable comments and suggestionsin the preparationof the draft. David A. Wyss of the Federal Reserve Board staff provided the computer simulationsof the MPS model and answerednumerous questions. 1. Derived as the change between December 1972 and December 1974, as shown in Board of Governorsof the FederalReserve System, unpublisheddetail accounts, from the flow of funds (July 1975). 257 258 BrookingsPapers on EconomicActivity, 2:1975 cyclesin businessactivity is, thus, only evidencethat investors'forecasts are betterthan randomguesses. -

Vanguard Economic and Market Outlook 2021: Approaching the Dawn
Vanguard economic and market outlook for 2021: Approaching the dawn Vanguard Research December 2020 ■ While the global economy continues to recover as we head into 2021, the battle between the virus and humanity’s efforts to stanch it continues. Our outlook for the global economy hinges critically on health outcomes. The recovery’s path is likely to prove uneven and varied across industries and countries, even with an effective vaccine in sight. ■ In China, we see the robust recovery extending in 2021 with growth of 9%. Elsewhere, we expect growth of 5% in the U.S. and 5% in the euro area, with those economies making meaningful progress toward full employment levels in 2021. In emerging markets, we expect a more uneven and challenging recovery, with growth of 6%. ■ When we peek beyond the long shadow of COVID-19, we see the pandemic irreversibly accelerating trends such as work automation and digitization of economies. However, other more profound setbacks brought about by the lockdowns and recession will ultimately prove temporary. Assuming a reasonable path for health outcomes, the scarring effect of permanent job losses is likely to be limited. ■ Our fair-value stock projections continue to reveal a global equity market that is neither grossly overvalued nor likely to produce outsized returns going forward. This suggests, however, that there may be opportunities to invest broadly around the world and across the value spectrum. Given a lower-for-longer rate outlook, we find it hard to see a material uptick in fixed income returns in the foreseeable future. Lead authors Vanguard Investment Strategy Group Vanguard Global Economics and Capital Markets Outlook Team Joseph Davis, Ph.D., Global Chief Economist Joseph Davis, Ph.D. -

Power Market Economics LLC Evolving Capacity Markets in A
Power Market Economics LLC Evolving Capacity Markets in a Modern Grid By Robert Stoddard State policies in New England mandate substantial shifts in the generation resources serving their citizen’s electrical needs. Maine, for example, has a statutory requirement to shift to 80 percent renewables by 2030, with a goal of reaching 100 percent by 2050. Massachusetts’ Clean Energy Standard sets a minimum percentage of renewables at 16 percent in 2018, increasing 2 percentage points annually to 80 percent in 2050. Facing these sharp departures from business-as-usual, policymakers raise a core question: are today’s wholesale market designs able to help the states achieve these goals? Can they even accommodate these state policy resources? In particular, are today’s capacity markets—which are supposed to guide the long-term investment in electricity generation resources—up to the job? Capacity markets serve a central role in New England’s electricity market. They serve a critical role in helping to ensure that the system operator, ISO New England (ISO-NE), will have enough resources, located strategically on the grid, to meet expected peak loads with a sufficient reserve margin. How capacity markets are designed and operate has evolved relatively little since the New York Independent System Operator (NYISO) launched the first full-fledged capacity market in 1999, the primary innovations being a longer lead-time in procurement of resources, better to support the orderly exit and construction of resources, and higher performance requirements, better to ensure that resources being paid to be available are in fact operating when needed. Are capacity markets now irrelevant? No. -

Principles of Microeconomics
PRINCIPLES OF MICROECONOMICS A. Competition The basic motivation to produce in a market economy is the expectation of income, which will generate profits. • The returns to the efforts of a business - the difference between its total revenues and its total costs - are profits. Thus, questions of revenues and costs are key in an analysis of the profit motive. • Other motivations include nonprofit incentives such as social status, the need to feel important, the desire for recognition, and the retaining of one's job. Economists' calculations of profits are different from those used by businesses in their accounting systems. Economic profit = total revenue - total economic cost • Total economic cost includes the value of all inputs used in production. • Normal profit is an economic cost since it occurs when economic profit is zero. It represents the opportunity cost of labor and capital contributed to the production process by the producer. • Accounting profits are computed only on the basis of explicit costs, including labor and capital. Since they do not take "normal profits" into consideration, they overstate true profits. Economic profits reward entrepreneurship. They are a payment to discovering new and better methods of production, taking above-average risks, and producing something that society desires. The ability of each firm to generate profits is limited by the structure of the industry in which the firm is engaged. The firms in a competitive market are price takers. • None has any market power - the ability to control the market price of the product it sells. • A firm's individual supply curve is a very small - and inconsequential - part of market supply. -

Retail Money Market Funds
Prospectus June 1, 2021 Retail Money Market Funds Fund Service Class Wells Fargo Money Market Fund WMOXX Wells Fargo National Tax-Free Money Market Fund MMIXX The U.S. Securities and Exchange Commission (“SEC”) has not approved or disapproved these securities or passed upon the accuracy or adequacy of this Prospectus. Anyone who tells you otherwise is committing a crime. Fund shares are NOT deposits or other obligations of, or guaranteed by, Wells Fargo Bank, N.A., its affiliates or any other depository institution. Fund shares are not insured or guaranteed by the U.S. Government, the Federal Deposit Insurance Corporation or any other government agency and may lose value. SUPPLEMENT TO THE PROSPECTUSES, SUMMARY PROSPECTUSES AND STATEMENT OF ADDITIONAL INFORMATION OF WELLS FARGO ALTERNATIVE FUNDS WELLS FARGO COREBUILDER SHARES WELLS FARGO FIXED INCOME FUNDS WELLS FARGO INTERNATIONAL AND GLOBAL EQUITY FUNDS WELLS FARGO MONEY MARKET FUNDS WELLS FARGO MULTI-ASSET FUNDS WELLS FARGO MUNICIPAL FIXED INCOME FUNDS WELLS FARGO SPECIALTY FUNDS WELLS FARGO TARGET DATE RETIREMENT FUNDS WELLS FARGO U.S. EQUITY FUNDS WELLS FARGO VARIABLE TRUST FUNDS (Each a “Fund”, together the “Funds”) At a meeting held July 15, 2021, the Board of Trustees of the Wells Fargo Funds approved a change in the Funds’ names to remove “Wells Fargo” from each Fund’s name and replace with “Allspring”. The change is expected to go into effect on Oct. 11, 2021. Wells Fargo Asset Management (WFAM) today announced that it will be changing its company name to Allspring Global Investments upon the closing of the previously announced sale transaction of WFAM by Wells Fargo & Company to GTCR LLC and Reverence Capital Partners, L.P. -
Key Areas of Economic Analysis of Projects: an Overview
KEY AREAS OF EcoNOMIC ANALYSIS OF PROJECTS An Overview ECONOMIC ANALYSIS AND OPERATIONS SUPPORT DIVISION (EREA) ECONOMICS AND RESEARCH DEPARTMENT (ERD) June 2004 CONTENTS INTRODUCTION PART I: SCOPE OF PROJECT ECONOMIC ANALYSIS 2 PART II: THE 10 AREAS OF ANALYSIS 10 1. Assess Macroeconomic Context 10 2. Assess Sector Context 11 3. Assess Demand 12 4. Identify Economic Rationale 13 5. Identify Project Alternatives 13 6. Identify and Compare Benefits and Costs 14 7. Assess Financial and Institutional Sustainability 15 8. Undertake Distribution Analysis 16 9. Undertake Sensitivity and Risk Analyses 16 10. Establish a Project Performance Monitoring System (PPMS) 17 PART Ill: AREAS OF ANALYSIS IN ADB's PROJECT PROCESSING CYCLE 18 6. Identification of Costs and Benefits 7. Fiscal/Financial Sustainability 8. Distribution Analysis 9. Sensitivity and Risk Analyses 10. Project Performance Monitoring System INTRODUCTION conomic analysis of projects helps identify and Eselect public investments that will sustainably improve the welfare of beneficiaries and a country as a whole. This 2"d edition pamphlet1 outlines key areas of economic analysis of projects. It stresses that analysis begins during country strategy studies and programming, when projects are identified, and continues iteratively throughout the project cycle. Economic analysis is coordinated with institutional, financial, environmental, social, and poverty analyses, forming an integral part of investment appraisal. Part I of the pamphlet summarizes the principles and key areas of analysis needed to appraise the economic feasibility of every project. The detailed assessment methods are outlined in ADB's Guidelines for the Economic Analysis of Projects (1997). Part II summarizes the main issues to be addressed in each of the 10 key areas of analysis (AAs). -

JA Economics® Course Overview and Outline
JA Economics® | Course Overview and Outline Initial JA Economics® Course Release Overview and Outline Spring 2019 Market for Goods JA Economics is a one-semester course that connects high and Services school students to the economic principles that influence their daily lives as well as their futures. It addresses each BANK of the economics standards identified by the Council for Production of Goods and Household Economic Education as being essential to complete a high Services + + Consumer school economics course. Course components equip students to: Market for Labor • Learn the necessary concepts applicable to state and national educational standards • Apply economic reasoning and skills in the world around them • Synthesize elective concepts through a cumulative, tangible deliverable (optional case studies and/or projects) • Demonstrate the skills necessary for future financial literacy pathway success • Integrate College and Career Readiness anchor standards in Reading, Informational Text, Speaking and Listening, and Vocabulary Volunteers engage with students through a variety of activities that includes subject matter guest speaking and coaching or advising for case study and project course work. Volunteer activities help students better understand the relationship between what they learn in school, their future career, and their successful participation in today’s global economy. Through a variety of experiential activities presented by the teacher and volunteer, students better understand the relationship between what they learn -

Financial Stability Oversight Council Statement on Money Market Fund
FINANCIAL STABILITY OVERSIGHT COUNCIL STATEMENT ON MONEY MARKET FUND REFORM Short-term funding markets provide a key source of funding for businesses, local governments, and other market entities in support of the U.S. economy. Stresses in the short-term funding markets can impact other financial market participants and the broader economy. Disruptions experienced during the early stages of the COVID-19 pandemic highlighted the importance of resilient short-term funding markets to the stability of the U.S. financial system. Money market funds (MMFs) are significant participants in these markets. The pandemic-induced market volatility demonstrated that disruptions in short-term funding markets, including at MMFs, have the potential to create or amplify financial instability. COVID-19 Market Stress and Potential Vulnerabilities In March 2020, in response to escalating concerns about the economic impact of the pandemic, market participants shifted their risk preferences toward cash and other highly liquid assets. This “dash for cash” created stress in both the secured and unsecured components of short-term funding markets. Liquidity pressures experienced by MMFs from rapid redemptions were affected by and subsequently contributed to dislocations in the short-term funding markets during the flight to liquidity and quality among investors. On March 18, 2020, the Federal Reserve, with Treasury approval, established the Money Market Mutual Fund Liquidity Facility with $10 billion of credit protection from the Treasury Department’s Exchange Stabilization Fund. Outflows from prime and tax-exempt MMFs subsided and conditions in short-term funding markets improved, supporting access to credit and the recovery in market conditions and economic activity. -

Foundations of Economics Chapter #2: the Organization of Economies
Unit #1: Foundations of Economics Chapter #2: The Organization of Economies In order to solve the problem of scarcity, societies must make choices. The basic economic questions are the main or basic choices that all societies must answer. These choices are influenced or guided by the rules or parameters set by each society. These rules or parameters compose the economic system. The Basic Economic Questions Because of scarcity every society or economic system must answer these three (3) basic questions: 1. What to produce? What should be produced in a world with limited resources? Exs) Using limited resources, should a local government build a new school or improve roads? Using limited resources, should a farmer grow wheat, cotton, or corn? Using limited resources, should an automobile manufacturer produce driverless cars? 2. How to produce? What resources should be used? Exs) How should we obtain oil? How much pollution should be allowed? How should we produce steel – using union or nonunion workers? Using recycled steel or iron ore? 3. Who consumes what is produced? Who acquires the product? How is it distributed? Exs) Who gets a flu vaccine? Where are new schools built? Who should clothes be produced for (what demographic group / generation)? The goal in answering these questions is both productive and allocative efficiency. Efficiency is the goal of all economic decisions to solve the problem of scarcity. Thus, the aim of each society is to answer the above questions efficiently. There are two types of efficiency: Productive efficiency: a situation in which the economy could not produce any more of one good without sacrificing production of another good. -

Historically Illustrating the Shift to Neoliberalism in the U.S. Home Mortgage Market
societies Essay Historically Illustrating the Shift to Neoliberalism in the U.S. Home Mortgage Market Ivis García City and Metropolitan Planning Department, University of Utah, Salt Lake City, UT 60608, USA; [email protected] Received: 8 October 2018; Accepted: 12 January 2019; Published: 18 January 2019 Abstract: This article takes a long view of the U.S. housing market; from its inception as locally owned and operated Building Societies, through one of the first major U.S. housing crises in the early 1930s, as well as through the prosperous and surprisingly stable post-WWII era the so-called “Long Boom” during Keynesianism. As labor shortages became more severe, accompanied by stagflation and the simultaneous urban, fiscal, and oil crises of the late 60s and early 70s, key sectors of the U.S. economy rallied to dismantle established Keynesian policies. While the new policies associated with laissez–faire economic liberalism certainly aided in the mobility of capital, the overall economy as a result of this neoliberal turn became increasingly unstable and inequitable. This article seeks to add knowledge to the neoliberalism theory. The author concludes, based on a historical case study of the Savings and Loans industry, that neoliberalism was not a deterministic overthrow of neoliberal ideologues but a haphazard response to the contradictions of Keynesian logic. It is only from a historical approach that we may be able to understand the current housing crisis, foster policy innovation, and allow for institutional change within the U.S. mortgage market sector. Keywords: banking; financial institutions; industry; mortgages 1. Introduction The effect of neoliberalism in the field of housing studies has gained considerable attention among scholars [1–4].