Approach to the Pelvic Examination: Preparation
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Chapter 28 *Lecture Powepoint
Chapter 28 *Lecture PowePoint The Female Reproductive System *See separate FlexArt PowerPoint slides for all figures and tables preinserted into PowerPoint without notes. Copyright © The McGraw-Hill Companies, Inc. Permission required for reproduction or display. Introduction • The female reproductive system is more complex than the male system because it serves more purposes – Produces and delivers gametes – Provides nutrition and safe harbor for fetal development – Gives birth – Nourishes infant • Female system is more cyclic, and the hormones are secreted in a more complex sequence than the relatively steady secretion in the male 28-2 Sexual Differentiation • The two sexes indistinguishable for first 8 to 10 weeks of development • Female reproductive tract develops from the paramesonephric ducts – Not because of the positive action of any hormone – Because of the absence of testosterone and müllerian-inhibiting factor (MIF) 28-3 Reproductive Anatomy • Expected Learning Outcomes – Describe the structure of the ovary – Trace the female reproductive tract and describe the gross anatomy and histology of each organ – Identify the ligaments that support the female reproductive organs – Describe the blood supply to the female reproductive tract – Identify the external genitalia of the female – Describe the structure of the nonlactating breast 28-4 Sexual Differentiation • Without testosterone: – Causes mesonephric ducts to degenerate – Genital tubercle becomes the glans clitoris – Urogenital folds become the labia minora – Labioscrotal folds -

The Cyclist's Vulva
The Cyclist’s Vulva Dr. Chimsom T. Oleka, MD FACOG Board Certified OBGYN Fellowship Trained Pediatric and Adolescent Gynecologist National Medical Network –USOPC Houston, TX DEPARTMENT NAME DISCLOSURES None [email protected] DEPARTMENT NAME PRONOUNS The use of “female” and “woman” in this talk, as well as in the highlighted studies refer to cis gender females with vulvas DEPARTMENT NAME GOALS To highlight an issue To discuss why this issue matters To inspire future research and exploration To normalize the conversation DEPARTMENT NAME The consensus is that when you first start cycling on your good‐as‐new, unbruised foof, it is going to hurt. After a “breaking‐in” period, the pain‐to‐numbness ratio becomes favourable. As long as you protect against infection, wear padded shorts with a generous layer of chamois cream, no underwear and make regular offerings to the ingrown hair goddess, things are manageable. This is wrong. Hannah Dines British T2 trike rider who competed at the 2016 Summer Paralympics DEPARTMENT NAME MY INTRODUCTION TO CYCLING Childhood Adolescence Adult Life DEPARTMENT NAME THE CYCLIST’S VULVA The Issue Vulva Anatomy Vulva Trauma Prevention DEPARTMENT NAME CYCLING HAS POSITIVE BENEFITS Popular Means of Exercise Has gained popularity among Ideal nonimpact women in the past aerobic exercise decade Increases Lowers all cause cardiorespiratory mortality risks fitness DEPARTMENT NAME Hermans TJN, Wijn RPWF, Winkens B, et al. Urogenital and Sexual complaints in female club cyclists‐a cross‐sectional study. J Sex Med 2016 CYCLING ALSO PREDISPOSES TO VULVAR TRAUMA • Significant decreases in pudendal nerve sensory function in women cyclists • Similar to men, women cyclists suffer from compression injuries that compromise normal function of the main neurovascular bundle of the vulva • Buller et al. -

Bates' Pocket Guide to Physical Examination and History Taking
Lynn S. Bickley, MD, FACP Clinical Professor of Internal Medicine School of Medicine University of New Mexico Albuquerque, New Mexico Peter G. Szilagyi, MD, MPH Professor of Pediatrics Chief, Division of General Pediatrics University of Rochester School of Medicine and Dentistry Rochester, New York Acquisitions Editor: Elizabeth Nieginski/Susan Rhyner Product Manager: Annette Ferran Editorial Assistant: Ashley Fischer Design Coordinator: Joan Wendt Art Director, Illustration: Brett MacNaughton Manufacturing Coordinator: Karin Duffield Indexer: Angie Allen Prepress Vendor: Aptara, Inc. 7th Edition Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins. Copyright © 2009 by Wolters Kluwer Health | Lippincott Williams & Wilkins. Copyright © 2007, 2004, 2000 by Lippincott Williams & Wilkins. Copyright © 1995, 1991 by J. B. Lippincott Company. All rights reserved. This book is protected by copyright. No part of this book may be reproduced or transmitted in any form or by any means, including as photocopies or scanned-in or other electronic copies, or utilized by any information storage and retrieval system without written permission from the copyright owner, except for brief quotations embodied in critical articles and reviews. Materials appear- ing in this book prepared by individuals as part of their official duties as U.S. government employees are not covered by the above-mentioned copyright. To request permission, please contact Lippincott Williams & Wilkins at Two Commerce Square, 2001 Market Street, Philadelphia PA 19103, via email at [email protected] or via website at lww.com (products and services). 9 8 7 6 5 4 3 2 1 Printed in China Library of Congress Cataloging-in-Publication Data Bickley, Lynn S. Bates’ pocket guide to physical examination and history taking / Lynn S. -

Signs to Help the Deaf Included in This Packet
Signs to help the Deaf Included in this packet: Medical Signs Color Signs People Signs This is made by: Deanna Zander, I am a parent of a deaf son. Here is my email address: [email protected], if you have any questions, please email your question, Please put in the Subject box- RE: Medical Signs. For more information, or to obtain a hospital kit for Deaf or Hard of Hearing, please contact Pam Smith, Adult Outreach Coordinator @ 701-665-4401 Medical Signs (Medicine) Medical Medicine- Tip of bent middle finger rubs circle on left palm Sign- Palm-out indexes circle Signs alternately Made By: Deanna Zander Hi, Hello, Howdy Good-Bye, Yes, Yep Bye Right “S” hand & head nods (both head & hand nod) No, Nope Flat hand, Touch forehead, Just wave First two fingers close onto move forward slightly right thumb, & shake your head Appointment Schedule Fingertips of the right palm- out “5” draws down left palm; then turn palm-in & draws across palm The right “S” hand palm down, is postitioned above the left “S” hand, also palm- down. The right hand circels above the left in a clockwise manner & is brought on the back of left hand. Your Name, My Name Birthday My, Mine- Your- The right middle finger touches the chin, Palm of flat Vertical flat palm moves then moves down to touch the chest hand on chest toward person Fingerspell- The right hand, palm- out, is move left to right, fingers wiggling up & Name- Right “H” touches left “H” at right angles MM/DD/YYYY down Call, phone Left “Y” hand, thumb near ear, little finger near mouth The upturned thumbs -

Birth Cont R Ol Fact Sheet
VAGINAL RING FACT SHEET What is the Vaginal Ring (Nuvaring®)? The Vaginal Ring is a clear, flexible, thin, plastic ring that you place in the vagina where it stays for one cycle providing a continuous low dose of 2 hormones (estrogen and progestin). It prevents pregnancy by stopping the release of an egg (ovulation), thickening the cervical fluid, and changing the lining of the uterus. How effective is the Vaginal Ring? The ring is a very effective method of birth control. The ring is about 93% effective at preventing pregnancy in typical use, which means that around 7 out of 100 people who use it as their only form of birth control will get pregnant in one year. With consistent and correct use as described in this fact sheet, it can be over 99% effective. How can I get the Vaginal Ring? You can visit a clinic to get the ring or a prescription for it and talk with a healthcare provider about whether the ring is right for you. Advantages of the Vaginal Ring Disadvantages of the Vaginal Ring Periods may be more predictable/regular and lighter Must remember to remove and replace the ring once a Less period cramping month Decreased symptoms of Premenstrual Syndrome Some users may experience mild side effects such as: (PMS) and perimenopause spotting, nausea, breast tenderness, headaches, or Can be used to skip or shorten your periods dizziness (usually these improve in the first few months Less anemia/iron deficiency caused by heavy periods of use) Does not affect your ability to get pregnant in the Possibility of high blood pressure -

Hand Gestures
L2/16-308 More hand gestures To: UTC From: Peter Edberg, Emoji Subcommittee Date: 2016-10-31 Proposed characters Tier 1: Two often-requested signs (ILY, Shaka, ILY), and three to complete the finger-counting sets for 1-3 (North American and European system). None of these are known to have offensive connotations. HAND SIGN SHAKA ● Shaka sign ● ASL sign for letter ‘Y’ ● Can signify “Aloha spirit”, surfing, “hang loose” ● On Emojipedia top requests list, but requests have dropped off ● 90°-rotated version of CALL ME HAND, but EmojiXpress has received requests for SHAKA specifically, noting that CALL ME HAND does not fulfill need HAND SIGN ILY ● ASL sign for “I love you” (combines signs for I, L, Y), has moved into mainstream use ● On Emojipedia top requests list HAND WITH THUMB AND INDEX FINGER EXTENDED ● Finger-counting 2, European style ● ASL sign for letter ‘L’ ● Sign for “loser” ● In Montenegro, sign for the Liberal party ● In Philippines, sign used by supporters of Corazon Aquino ● See Wikipedia entry HAND WITH THUMB AND FIRST TWO FINGERS EXTENDED ● Finger-counting 3, European style ● UAE: Win, victory, love = work ethic, success, love of nation (see separate proposal L2/16-071, which is the source of the information below about this gesture, and also the source of the images at left) ● Representation for Ctrl-Alt-Del on Windows systems ● Serbian “три прста” (tri prsta), symbol of Serbian identity ● Germanic “Schwurhand”, sign for swearing an oath ● Indication in sports of successful 3-point shot (basketball), 3 successive goals (soccer), etc. HAND WITH FIRST THREE FINGERS EXTENDED ● Finger-counting 3, North American style ● ASL sign for letter ‘W’ ● Scout sign (Boy/Girl Scouts) is similar, has fingers together Tier 2: Complete the finger-counting sets for 4-5, plus some less-requested hand signs. -
Understanding Cancer of the Vulva
Understanding Cancer of the Vulva An information sheet for women with cancer, their families and friends. This information has been prepared to help you If something goes wrong with the genes that understand more about cancer of the vulva control a cell, that cell may start behaving (vulvar cancer). It is an introduction to the strangely. Instead of growing normally, it may diagnosis, treatment and effects of this cancer. grow and divide in an uncontrolled way, forming a mass of cells. The mass of cells looks We cannot advise you about the best treatment and feels like a lump, and is called a tumour. for you. You need to discuss this with your doctors. However, we hope this information A tumour can be benign (not cancer) or it can will answer some of your questions and help be malignant (cancer). The difference is that you think about the questions you want to ask benign tumours do not spread to other parts of your doctors. the body, while malignant tumours can. For more detailed information on cancer of the A malignant tumour is made up of cancer cells. vulva, you may wish to contact the Cancer When it first develops, the tumour stays in one Council Helpline on 13 11 20 or refer to the place. This is called the primary tumour. list of recommended websites under the heading Information on the Internet on the If the cancer cells that make up the primary back page of this booklet. tumour are not treated, they may start to spread to other areas of the body and form new tumours. -

Consonants Name of Sound Verbal Cue Other Cues
CONSONANTS NAME OF SOUND VERBAL CUE OTHER CUES “p” sound Popping sound “Where’s your pop?” Fill cheeks up with air “You forgot your and blow out with the pop.” sound, feeling wind on hand “b” sound Popping sound “Where’s your pop?” Fill cheeks up with air “You forgot your and blow out with the pop.” sound “m” sound Humming sound “Close you mouth and Lips together and hum hummmm.:” Touch to feel vibration “n “ sound Buzzing teeth or “Teeth together and Finger on clenched buzzing tongue sound buzz.” teeth to feel vibration “t” sound Tippy sound “Use your tippy.” Index finger to center of spot above upper lip “d” sound Tippy sound “Use your tippy.” Index finger to center of spot above upper lip “h” sound Open mouth windy “Where’s your wind?” Open palm of hand up sound “I didn’t feel your just in front of your wind.” mouth to feel wind “k” sound Throaty sound “Where’s your Index finger pointed throaty?” to throat “g” sound Throaty sound “Where’s your Index finger pointed throaty?” to throat “f” sound Biting lip windy “You forgot to bite Bite lower lip with sound your lip.” “You upper teeth and blow forgot your wind.” wind “v” sound Biting lip windy “You forgot to bite Bite lower lip with sound your lip.” “You upper teeth and blow forgot your wind.” wind Initial “s” sound Smiley windy sound “Smile and make Smile with teeth some wind.” “Keep together and blow those teeth together.” wind Final sounds Sticky sounds “Where’s your Same as above for sticky?” most but for “s” move forearm form left to right starting with an open hand and moving to a closed hand “z” sound Buzzing windy sound “Use your buzz.” Teeth together and blow wind “sh”sound Fat and fluffy sound “Make it fat and Lips out and puckered fluffy.” while blowing out Copyright David W Hammer, MA CCC-SLP Special thanks to Mary Ann Migitsch for her contribution to this chart. -

Palm Reading
Palm Reading Also known as palmistry or chiromancy, palm reading is practiced all over the world with roots in Indian astrology and gypsy fortune-telling. The objective is to evaluate a person’s character and aspects of their life by studying the palm of their hand. There is no substantiate evidence of correlation between palm features and psychological traits; palm reading is for entertainment purposes. Getting Started Which hand to read? There are two main practices: For males, the left hand is what you’re born with, and the right is what you’ve accumulated throughout your life. For females, it’s the opposite. Your dominant hand (the hand you use most often) determines your future and your other, non-dominant hand, is used to determine the past or hidden traits Take these into consideration when choosing which hand to read. Reading the Primary Lines of your Hand 1. Interpret the Heart Line This line is believed to indicate emotional stability, romantic perspectives, depression, and cardiac health. Begins below the index finger = content with love life Begins below the middle finger = selfish when it comes to love Begins in-between the middle and index fingers = caring and understanding Is straight and short = less interest in romance Touches life line = heart is broken easily Is long and curvy = freely expresses emotions and feelings Is straight and parallel to the head line = good handle on emotions Is wavy = many relationships, absence of serious relationships Circle on the line = sad or depressed Broken line = emotional trauma 2. Examine the Head Line This line represents learning style, communication style, intellectualism, and thirst for knowledge. -

Clinical Pelvic Anatomy
SECTION ONE • Fundamentals 1 Clinical pelvic anatomy Introduction 1 Anatomical points for obstetric analgesia 3 Obstetric anatomy 1 Gynaecological anatomy 5 The pelvic organs during pregnancy 1 Anatomy of the lower urinary tract 13 the necks of the femora tends to compress the pelvis Introduction from the sides, reducing the transverse diameters of this part of the pelvis (Fig. 1.1). At an intermediate level, opposite A thorough understanding of pelvic anatomy is essential for the third segment of the sacrum, the canal retains a circular clinical practice. Not only does it facilitate an understanding cross-section. With this picture in mind, the ‘average’ of the process of labour, it also allows an appreciation of diameters of the pelvis at brim, cavity, and outlet levels can the mechanisms of sexual function and reproduction, and be readily understood (Table 1.1). establishes a background to the understanding of gynae- The distortions from a circular cross-section, however, cological pathology. Congenital abnormalities are discussed are very modest. If, in circumstances of malnutrition or in Chapter 3. metabolic bone disease, the consolidation of bone is impaired, more gross distortion of the pelvic shape is liable to occur, and labour is likely to involve mechanical difficulty. Obstetric anatomy This is termed cephalopelvic disproportion. The changing cross-sectional shape of the true pelvis at different levels The bony pelvis – transverse oval at the brim and anteroposterior oval at the outlet – usually determines a fundamental feature of The girdle of bones formed by the sacrum and the two labour, i.e. that the ovoid fetal head enters the brim with its innominate bones has several important functions (Fig. -
ASL) Visual Reference Library
American Sign Language (ASL) Visual Reference Library Important, everyday Swagelok terms and phrases, and how to sign them. Swagelok Visual Reference Library 2 About the Swagelok American Sign Language (ASL) Visual Reference Library At Swagelok, we believe in providing a work environment rooted in the values of continuous improvement and mutual respect among every supervisor and associate. We believe that clear communication and teamwork are critical to meeting those goals. And we are committed to ensuring that all associates, across our sites, have the tools they need to converse and work together successfully. The Swagelok American Sign Language (ASL) Visual Reference Library is one of those tools. Swagelok employs associates with hearing loss or who are hearing impaired whose primary means of communication is through American Sign Language. This document exists to record signs of a variety of important, Swagelok-specific terms and phrases that have been identified by the associates and team members who use them the most: our hearing impaired associates, their peers, and supervisors. Each definition includes written and visual signing instructions, as well as a link to a video of the sign being performed by our own associate, Alvin Waggy. We hope you will use this tool to foster clear, consistent communication among all Swagelok associates, now and in the future. Table of Contents Click to view entry. Actuator ______________ 3 First Aid ______________ 12 Moving Negative ______ 20 Staking ______________ 29 Assembly _____________ 3 First -
CMC Stabilization Exercises the Purpose of These Exercises Is to Strengthen Your Muscles Around Your Arthritic Thumb Joint Making It More Stable and Less Painful
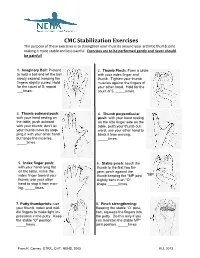
CMC Stabilization Exercises The purpose of these exercises is to strengthen your muscles around your arthritic thumb joint making it more stable and less painful. Exercises are to be performed gently and never should be painful! 1. Imaginary Ball: Pretend 2. Thumb Pinch: Form a circle to hold a ball and let the ball with your index finger and slowly expand, keeping the thumb. Tighten your thumb fingers slightly curled. Hold muscles against the fingers of for the count of 5, repeat your other hand. Hold for the ___times. count of 5, _____times. 3. Thumb outward push: 4. Thumb perpendicular with your hand resting on push: with your hand resting the table, push outward on the little finger side on the with your thumb; don’t let table, push your thumb out- your thumb move by stop- ward; use your other hand to ping it with your other hand block it from moving. but tense the muscles. _____times. _____times. 5. Index finger push: 6. Stable pinch: touch the with your hand lying flat thumb to the first two fin- on the table, move the gers; pinch against the index finger toward your thumb keeping the *MP joint *MP thumb; use your other slightly bent in an “O” hand to stop it from mov- shape. _____times. ing. _____times. 7. Putty thumbprints: use 8. Pinch strengthening: your thumb, index and mid- Keeping the stable “O” posi- dle fingers to make light im- tion, squeeze the fingers into pressions in the putty. Keep the putty. Do this only if you the stable “O” position.