Medical Innovation: Statins (Pharmaceutical: Small Molecule)
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Statins: in the Beginning
J R Coll Physicians Edinb 2009; 39:362–4 Paper doi:10.4997/JRCPE.2009.425 © 2009 Royal College of Physicians of Edinburgh Statins: in the beginning 1KS Lyons; 2M Harbinson 1Research Fellow, Department of Therapeutics and Pharmacology, Queen’s University, Belfast; 2Senior Lecturer, Department of Therapeutics and Pharmacology, Queen’s University, Belfast, and Consultant Cardiologist, Belfast Health and Social Care Trust, UK ABSTRACT Since the first human trial of a hydroxymethylglutaryl-coenzyme A Published online December 2009 (HMG CoA) reductase inhibitor in 1978, the growth in importance of this drug class, both financially and medically, has been staggering. The aim of this paper is to Correspondence to KS Lyons, Department of Therapeutics and summarise how this drug class was developed, highlighting the role of Akira Endo. Pharmacology, Whitla Medical Building, 97 Lisburn Road, KEYWORDS Compactin, Akira Endo, lovastatin, statins Belfast BT9 7BL DECLARATION OF INTERESTS No conflict of interests declared. tel.+44 (0)2890 975772 e-mail [email protected] Hydroxymethylglutaryl-coenzyme A (HMG CoA) two years at the Albert Einstein College of Medicine reductase inhibitors (statins) are now one of the most working on cell wall biosynthetic enzymes.6 widely prescribed medications worldwide, with an estimated 2 million people in the UK1 and more than 18 When Endo returned to Sankyo in 1968 he began work million people in the USA currently taking a statin.2 on the quest to find an effective cholesterol-lowering From their development in the 1970s the impact of drug. He worked on the premise that some microbes statins on the treatment of cardiovascular disease been might produce inhibitors of enzymes necessary for staggering. -

Pjapan PRIZE NEWS=No.35=Ł\
THE SCIENCE AND TECHNOLOGY No. 35 FOUNDATION OF JAPAN (JSTF) January 2006 Akasaka Twin Tower East, 13th Floor, 17-22 Akasaka 2-chome, Minato-ku, Tokyo, 107-0052, JAPAN Tel. +81-3-5545-0551 Fax. +81-3-5545-0554 E-mail [email protected] URL http://www.japanprize.jp U.K. and Japanese Scientists Named as Laureates of the 2006(22nd)Japan Prize The Science and Technology Foundation of Japan (Chairman: Hiroyuki Yoshikawa) announced that British and Japanese scientists have been named as laureates of the 2006 (22nd) Japan Prize. Sir John Houghton (74), Formerly Chief Executive, Hadley Centre for Climate Prediction and Research, Meteorological Office, U.K., will receive the Japan Prize in this year's category of "Global Change." He contributed to the Atmospheric structure and composition based on his satel- ite observation technology and for promotion of international assessments of climate change. Dr. Akira Endo (72), Director, Biopharm Research Laboratories, Inc., Japan, will receive the Ja- pan Prize in the category of "The Development of Novel Therapeutic Concepts and Technolo- gies." He contributed to the Discovery of the Statins. The Development of Novel Global Change Therapeutic Concepts and Technologies Sir John Houghton CBE FRS Dr. Akira Endo Japan Prize The Japan Prize is awarded to world-class scientists and technolo- Fields of study for the prize encompass all categories of science gists who were credited with original and outstanding achievements and technology, with two categories designated for the prize each and contributed to the advancement of science and technology, year in consideration of developments in science and technology. -

Exploitation of Aspergillus Terreus for the Production of Natural Statins
Journal of Fungi Review Exploitation of Aspergillus terreus for the Production of Natural Statins Mishal Subhan 1, Rani Faryal 1 and Ian Macreadie 2,* 1 Department of Microbiology, Faculty of Biological Sciences, Quaid-i-Azam University, Islamabad 45320, Pakistan; [email protected] (M.S.); [email protected] (R.F.) 2 School of Science, RMIT University, Bundoora, Victoria 3083, Australia * Correspondence: [email protected]; Tel.: +61-3-9925-6627 Academic Editor: David S. Perlin Received: 19 April 2016; Accepted: 26 April 2016; Published: 30 April 2016 Abstract: The fungus Aspergillus (A.) terreus has dominated the biological production of the “blockbuster” drugs known as statins. The statins are a class of drugs that inhibit HMG-CoA reductase and lead to lower cholesterol production. The statins were initially discovered in fungi and for many years fungi were the sole source for the statins. At present, novel chemically synthesised statins are produced as inspired by the naturally occurring statin molecules. The isolation of the natural statins, compactin, mevastatin and lovastatin from A. terreus represents one of the great achievements of industrial microbiology. Here we review the discovery of statins, along with strategies that have been applied to scale up their production by A. terreus strains. The strategies encompass many of the techniques available in industrial microbiology and include the optimization of media and fermentation conditions, the improvement of strains through classical mutagenesis, induced genetic manipulation and the use of statistical design. Keywords: Aspergillus terreus; compactin; fermentation; industrial microbiology; lovastatin; mevastatin; mutagenesis; optimization; polyketide 1. Introduction Statins are polyketide compounds that are produced by some fungi during their secondary metabolism [1]. -

Chronicles Booklet.Indd
Page 1 UCSD Emeriti Association 214 University Center, UCSD La Jolla, California 92093-0002 Chronicles Newsletter of the UCSD Emeriti Association Volume V, No. 1 September 2005 RETURN SERVICE REQUESTED Frontiers of Medicine “The Cholesterol Wars:” How the Statins Won anyway, why bother your head? So the met with great skepticism. What the discovery of the statin drugs, drugs that skeptics failed to consider is that no SEPTEMBER 2005 lower cholesterol levels dramatically one was proposing to block cholesterol and safely (by inhibiting the body’s own synthesis completely; that very well synthesis of cholesterol), played a major might be bad. But if you could titrate the role in ending “The Great Cholesterol dose of the inhibitor so as to achieve a Controversy.” lowering of blood cholesterol without First, it was necessary to overcome reducing the amount of intracellular concerns about the feasibility and safety cholesterol needed for optimal health, —by Daniel Steinberg, of inhibiting the natural synthesis of you might have a novel way to correct M.D., Ph.D. cholesterol. The human body can hypercholesterolemia. Emeritus Professor of Medicine Chronicles make all the cholesterol it needs by That was the gist of the proposal breaking down other foodstuffs (fats put forward in the early 1950s by Jean Mark Your Calendar! n an earlier issue of this newsletter, Newsletter of the UCSD Emeriti Association and carbohydrates) and converting Cottet and his collaborators in France I briefl y chronicled the uphill battle I the fragments into cholesterol. In fact, and by Steinberg and Fredrickson here. waged through the 20th century to Wednesday, October 19 most people make as much cholesterol However, neither group came up with a convince the medical profession that every day as they consume in their diet. -
Red Yeast Rice COMMON NAME: Red Yeast Rice
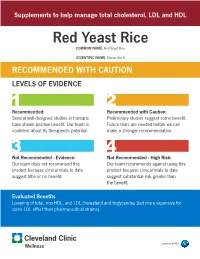
Supplements to help manage total cholesterol, LDL and HDL Red Yeast Rice COMMON NAME: Red Yeast Rice SCIENTIFIC NAME: Monacolin K RECOMMENDED WITH CAUTION LEVELS OF EVIDENCE 1 2 Recommended: Recommended with Caution: Several well-designed studies in humans Preliminary studies suggest some benefit. have shown positive benefit. Our team is Future trials are needed before we can confident about its therapeutic potential. make a stronger recommendation. 3 4 Not Recommended - Evidence: Not Recommended - High Risk: Our team does not recommend this Our team recommends against using this product because clinical trials to date product because clinical trials to date suggest little or no benefit. suggest substantial risk greater than the benefit. Evaluated Benefits Lowering of total, non-HDL, and LDL cholesterol and triglycerides (but more expensive for some LDL effect than pharmaceutical strains). Supported by P&G HeartHealth-RecommendedWithCaution.indd 1 6/27/2017 10:56:50 AM Source Powdered fermented product of Monascus purpureus (red yeast) grown on white polished rice Indications/Population Patients with hypercholesterolemia Patients intolerant of prescription statins Mechanism of Action Red yeast rice (RYR) contains small amounts of monacolin K. This is the same substance isolated from the fungus Monascus ruber by Akira Endo in 1979 and from Aspergillus terreus by Hoffmann and coworkers the same year, and later commercialized as the drug lovastatin, a 3-hydroxy-3- methylglutaryl coenzyme (HMG-CoA) reductase inhibitor. It has been suggested that the cholesterol-lowering effect of RYR products in general may not be accounted for by its monacolin K content alone. The other monacolins present in RYR — including monacolins J, L, and X and dihydromonacolin L, monacolin M, and dihydromevinolin (known as secondary metabolites) — may play a synergistic inhibitory effect on HMG-CoA reductase. -
Controlling Methane at ERD and ISCR Applications
REMEDIATION Controlling Methane at ERD and ISCR Applications Active measures to control the production of methane can offer multiple advantages in terms of cost, treatment effi ciency and safety. >> JIM MUELLER, PH.D., ANTONIS KARACHALIOS, PH.D., AND TROY FOWLER n-situ chemical reduction (ISCR) and enhanced Many readers will know from their own experiences that reductive dehalogenation (ERD) have demonstrated these amendments have been widely used with varying success in the remediation of numerous recalcitrant degrees of success in terms of overall remedial perfor- and toxic compounds, including chlorinated ethenes mance. One seemingly universal phenomenon has been and hexavalent chromium. ISCR describes the the biological production of methane, especially during Icombined effect of stimulated biological oxygen consump- the early phases of remedial actions (look for it and you tion (via fermentation of an organic carbon source), direct will find it). Active measures to control the production of chemical reduction with zero-valent iron (ZVI) or other methane can offer multiple advantages in terms of cost, reduced metals. As described by Brown et al (2009)[1], the treatment efficiency and safety. corresponding enhanced thermodynamic decomposition reactions that are realized at the lowered redox (Eh) condi- What Is a Methanogen? tions allow for more effective mineralization of many con- In the 1970s, Dr. Carl Woese and his colleagues at the Uni- stituents of interest (COIs). A growing number of ERD versity of Illinois at Urbana-Champaign studied prokary- substrates and other accelerated anaerobic bioremediation otic relationships using DNA sequences, and they found technologies (e.g., emulsified oils, non-emulsified oils, car- that microbes that produce methane[2] – or methanogens bon-based hydrogen release compounds, vegetable matter – are Archaea. -
History of Statins Scott M
History of Statins Scott M. Grundy, MD, PhD University of Texas Southwestern Medical Center Dallas, Texas COI: Consultant: Merck, Janssen Akira Endo discovered Compactin in 1977 Penicillium citrinum Pen-51, the fungus that produces compactin Kaneko , Endo, et al. Eur J Biochem. 1978: 87: 313-321. Hypolipidemic effects of compactin in dogs. Tsujita, Endo, et al. Atherosclerosis 1979: 21:307-313 Akira Yamamoto's patient with familial hypercholesterolemia first received compactin in 1978. Effect of Compactin in a Patient with Heterozygous Familial Hypercholesterolemia Yamamoto et al. Atherosclerosis 1980; 35: 259-266 Compactin Treatment in Heterozygous Familial Hypercholesterolemia Mabuchi et al. NEJM 1981: 305: 478-482 Discovery of Lovastatin • At the end of the 1970s other pharmaceutical companies to begin searching for another statin. • In July 1976, Merck Research Laboratories, signed a confidentiality agreement with Sankyo and obtained samples of compactin and confidential experimental data. • Under the direction of Alfred Albert, Merck set out to find its own statins . • In February 1979 Albert isolated a statin very similar to compactin, called mevinolin (lovastatin) Alfred W. Albert Discontinuation of Compactin Development • In August 1980 Sankyo discontinued the clinical development of compactin. • The drug apparently caused lymphoma in dogs when given in high doses Suspension of Development of Lovastatin • In April 1980, Merck began preliminary clinical studies of lovastatin • But after 5 months, in September 1980, they discontinued the clinical trials because of rumors that compactin caused cancers in dogs. • For this reason Merck halted studies on lovastatin. Early FDA Involvement • Following Merck's decision to terminate clinical trials, FDA became actively involved in maintaining interest in the development of the statins. -

An Overview of the Bioactivity of Monacolin K / Lovastatin
Food and Chemical Toxicology 131 (2019) 110585 Contents lists available at ScienceDirect Food and Chemical Toxicology journal homepage: www.elsevier.com/locate/foodchemtox An overview of the bioactivity of monacolin K / lovastatin T Zixiao Xionga,b, Xiaohua Caoc, Qinyou Wena,d, Zhiting Chena,d, Zuxin Chengc, Xinying Huangc, ∗ Yangxin Zhanga, Chuannan Longe, Yi Zhanga,b,d, Zhiwei Huanga,b,d, a College of Food Science, Fujian Agriculture and Forestry University, Fuzhou, 350002, China b China-Ireland International Cooperation Centre for Food Material Science and Structure Design, Fujian Agriculture and Forestry University, Fuzhou, 350002, China c Key Laboratory of Crop Biotechnology (Fujian Agriculture and Forestry University), Fujian Province University, Fuzhou, 350002, China d Fujian Provincial Key Laboratory of Quality Science and Processing Technology in Special Starch, Fujian Agriculture and Forestry University, Fuzhou, 350002, China e Jiangxi Key Laboratory of Bioprocess Engineering, Jiangxi Science and Technology Normal University, Nanchang, 330013, China ARTICLE INFO ABSTRACT Keywords: Monacolin K (MK) is the principal active substance in Monascus-fermentation products (e.g. red yeast rice). MK is Monascus effective in reducing cholesterol levels in humans and has been widely used as a lipid-lowering drug. The me- Red yeast rice chanism for this is through a high degree of competitive inhibition of the rate-limiting enzyme HMG-CoA re- Monacolin K ductase (HMGR) in the cholesterol synthesis pathway. In addition to lowering blood lipid levels, MK also pre- Lovastatin vents colon cancer, acute myeloid leukemia and neurological disorders such as Parkinson's disease and type I Statins neurofibromatosis. The aim of this manuscript is to comprehensively review the progress in the study of the Bioactivity biological activity of MK and its imechanism of action in reducing blood lipid concentration, prevention of cancer and its neuroprotective, anti-inflammatory and antibacterial properties. -

2008 LASKER AWARDS for MEDICAL RESEARCH
2008 LASKER AWARDS for MEDICAL RESEARCH Key Words: Lasker Awards – Lasker Foundation – small RNA – microRNA – gene silencing - statins – cholesterol - bacteria – microbes – microbiology – pathogenesis – infectious disease – Ambros – Ruvkun – Baulcombe – Endo - Falkow EMBARGOED FOR RELEASE: CONTACT: Kendall Christiansen For initial publication and broadcast Geto & de Milly, Inc. on Saturday, September 13, 2008 212.686.4551; cell: 917.359.0725 Email: [email protected] at 5 p.m. EST. DISCOVERERS OF SMALL REGULATORY RNAS AND CHOLESTEROL-LOWERING DRUGS TO RECEIVE LASKER AWARDS FOR MEDICAL RESEARCH PIONEER IN UNDERSTANDING HARMFUL BACTERIA HONORED WITH SPECIAL ACHIEVEMENT AWARD NEW YORK, Saturday, September 13, 2008 – The 2008 Albert Lasker Medical Research Awards were announced today. First presented in 1946, the Lasker Awards are the nation’s most distinguished honor for outstanding basic and clinical medical research discoveries and for lifetime contributions to medical science. The Lasker Award for Basic Medical Research honors Victor R. Ambros, 54, of the University of Massachusetts Medical School, Worcester, David C. Baulcombe, 56, of the University of Cambridge, and Gary B. Ruvkun, 56, of Massachusetts General Hospital, Boston and Harvard Medical School, who discovered tiny RNAs that regulate gene function. These RNAs, some of which are known as microRNAs, govern a multitude of activities in animals and plants, and they have been implicated in a wide range of diseases. The Lasker~DeBakey Award for Clinical Medical Research honors Akira Endo, 74, of Biopharm Research Laboratories, Inc., Tokyo, who discovered the first statin. Statins significantly lower LDL-cholesterol quantities in the blood, thus dramatically reducing the risk of coronary heart disease, a leading cause of death worldwide and the number one killer in the U.S. -

An Effective Method for Lovastatin Production by Fungi Over Submerged Fermentation
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by ePrints@Bangalore University E3 Journal of Biotechnology and Pharmaceutical Research Vol. 3(2), pp. 15-21, April 2012 Available online at http://www.e3journals.org/JBPR ISSN 2141-7474 © 2012 E3 Journals Mini Review Solid state fermentation: An effective method for Lovastatin production by fungi over submerged fermentation Praveen VK and Savitha J* Department of Microbiology and Biotechnology, Bangalore University, Jnana Bharathi Campus, Bangalore-560056. India. Accepted 13 March, 2012 The Enzyme 3-hydroxy-3-methylglutaryl-CoA reductase (HMG CoA reductase) catalyses conversion of HMG CoA to mevalonate during cholesterol biosynthesis. Lovastatin is used as an anti-cholesterol drug which blocks HMG CoA reductase activity. Lovastatin has been reported to be produced by Submerged Fermentation (SmF) and Solid State Fermentation (SSF) by fungi. Of-late it is used not only as anti- cholesterol drug but as anti-inflammatory agent, cancer cell apoptosis, restoration of renal function, bone disorders treatment; immune-modulatory role is also being investigated. This review provides insight into the different lovastatin production strategies employed by SSF, its advantages over SmF, optimisation parameters, lovastatin genetics etc. Key words: HMG CoA. Lovastatin, Fungi, SSF, SmF, Pleiotropic. INTRODUCTION The World Health Organization estimated that 17.3 antibiotic and other related pharmacological properties million lives were lost in 2008 and an expected 23.6 (Bedford et al., 1995). Noted among the fungal million people will die of cardiovascular diseases (CVD) metabolites are statins (anti-cholesterol compounds) that by the year 2030 (WHO, 2011). Close to 80% of mortality are considered as the most important class produced by rates were reported from the lower and middle income the polyketide pathway. -

A Gift from Nature: the Birth of the Statins
LASKER~DEBAKEY C L INICA L M E D ICA L COMMENTARY RESEARCH AWARD A gift from nature: the birth of the statins Akira Endo I was born into a rural farming family in study under him. Unfortunately, the autumn northern Japan, near Akita, where I lived for 1966 class for which I was applying was already 17 years with my extended family, including full. So I eventually studied from September grandparents, parents, three brothers and two 1966 to August 1968 at the Department of sisters. My grandfather, who had an interest Molecular Biology at the Albert Einstein College in medicine and science, was a great home of Medicine in New York. Under the guidance teacher to me. Thanks to his influence, at the of Bernard Horecker and Lawrence Rothfield, age of 8, I dreamt of becoming a scientist, I studied an enzyme that was involved in the much like the renowned Japanese scientist biosynthesis of bacterial cell wall lipopolysac- Hideyo Noguchi, who, in 1900 at the age of 24, charide. The outcome of my research depended went to the United States and studied syphilis upon purifying the unstable enzyme. A year and yellow fever at the Rockefeller Institute into the project, I succeeded and showed that in New York. the formation of an enzyme–phospholipid After finishing high school in Akita, I entered complex was crucial for its action. Tohoku University’s College of Agriculture in While living in New York, I was very sur- Sendai in 1953. I excelled in organic chemis- prised by the large number of elderly and over- try at high school.