Download Download
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

OPERATION SCHEME of the Executives of Sectors, Head Offices and Secretaries of Head Offices of Tashkent Region
OPERATION SCHEME of the Executives of Sectors, Head offices and secretaries of Head offices of Tashkent Region Sector 1 – Khokim’s Head office Sector 2 – Head office secretary of the Sector 3 –Head office secretary of the Sector 4 – Head office secretary of the secretary and location Prosecutor’s Office and location Department of Internal affairs (DIA) State Tax Inspectorate and location and location Khidoyatov Davron Abdulpattakhovich Samadov Salom Ismatovich Aripov Tokhir Tulkinovich Raimov Ravshan Isakjanovich KHOKIM OF THE REGION TASHKENT REGION PROSECUTOR MAIN DEPARTMENT OF INTERNAL STATE TAX INSPECTORATE OF HEAD OFFICE SECRETARY: A. Eshbaev HEAD OFFICE SECRETARY: М. Egamberdiev AFFAIRS OF TASHKENT REGION TASHKENT REGION Phone number: (98) 007-30-04 Phone number: (97) 733-57-37 HEAD OFFICE SECRETARY: F. HEAD OFFICE SECRETARY: E. Djumabaev Location: 1, Almalik city, Tashkent region. Location: 1, Tashkent yuli, Nurafshan city. Khamitov Phone number: (93) 398-54-34 Phone of the Head office: (70) 201-07-34 +6448 Phone number: (99) 301-70-77 Location: 79 A, Babur str., Tashkent. Location: Mevazor, Kuyichirchik region. Phone of the Head office: (78) 150-49-56 Phone of the Head office: (95) 476-75 -77 Saliyev Muzaffar Kholdorbolevich Mirzayev Fakhriddin Yusupovich Amanbaev Navruz Zokirjonovich Narkhodjaev Sanjar Rashidovich KHOKIM OF NURAFSHAN CITY PROSECUTOR OF NURAFSHAN CITY DIA OF NURAFSHAN CITY NURAFSHAN CITY STATE TAX HEAD OFFICE SECRETARY: О. Erbaev HEAD OFFICE SECRETARY: М.Shukrullaev HEAD OFFICE SECRETARY: F. INSPECTORATE Phone number: (99) 823-67-72 Phone: (97) 911-77-10 Imankulov HEAD OFFICE SECRETARY: E. Igamnazarov Location: Tashkent yuli str., Nurafshan city. Location: 4A, Shon shukhrat str., Obod turmush Phone: (94) 631-49-37 Phone: (94) 930-03-73 CCU, Nurafshan city. -

Measures to Stabilize the Socio-Economic Development of Regions in a Pandemic (On the Example of the Industrial Complex of the Tashkent Region)
© Journal «Bulletin Social-Economic and Humanitarian Research», № 9 (11), 2021, e-ISSN 2658-5561 Publication date: January 2, 2021 DOI: 10.5281/zenodo.4263353 Economical Sciences MEASURES TO STABILIZE THE SOCIO-ECONOMIC DEVELOPMENT OF REGIONS IN A PANDEMIC (ON THE EXAMPLE OF THE INDUSTRIAL COMPLEX OF THE TASHKENT REGION) Batirova, Nilufar Sherkulovna1 1Senior lecturer, International Islamic Academy of Uzbekistan, Tashkent, Uzbekistan Abstract The article describes the features of the industrial development of the Tashkent region. Within one region, an industrial complex was analyzed. Some views of theorists on regional development are given. The opinions of these scientists on the factors affecting the development of industry in the region are analyzed. The economic potential and geographical location of the regions can lead to a clear division of the individual territories in industrial production. The economic and industrial potential of the Tashkent region was evaluated. It also analyzes the economic potential of the region. The role of regional sectors of the economy in the country is considered. It describes the economic potential of districts and cities, the availability of financial resources and the level of development of scientific and technological progress. It indicates the need to change the principles of state regulation of the scientific sphere for innovative development and the effective functioning of the region’s industry, foreign experience is an example of organizational and economic measures supporting the innovative development of the region’s industry. The composition of factors influencing the innovative development of the region's industry is also analyzed in turn. In particular, the emphasis in innovation is on the development of the human factor, science and technology. -

Uzbekistan: Tashkent Province Sewerage Improvement Project
Initial Environmental Examination May 2021 Uzbekistan: Tashkent Province Sewerage Improvement Project Prepared by the Joint Stock Companies “Uzsuvtaminot” for the Asian Development Bank. ..Þ,zýUçâÛ,ÜINÞâ'' .,UzSUVTAMINoT" »KSIYADORLIK J°¼IY»ÂI JoINT ýâÞáÚ áÞÜà°ItÓr 1¾¾¾35, O'zbekiston Respublikasi l0OO35, Republic of Uzbekistan Toshkent shahri, Niyozbek yo'li ko'chasi 1-çã Tashkent ciý, Niyozbek 5ruli stÛÕÕt 1 apt. telefon: +998 55 5Þ3 l2 55 telephone: +998 55 503 12 55 uzst14,exat.uz, infcl(rtluzsuv. çz æzst{o exat. uz, iÛ[Þ(Ð æzsçç, æz _ 2 Ñ 1,1AÙ 202l Nq 4l2L 1 4 2 Ò ÂÞ: ¼r. Jung ½Þ ºim Project Officer SÕßiÞr UrÌÐß Development Specialist ÁÕßtrÐl and West Asia DÕàÐÓtmÕßt UrÌÐß Development and Water Division °siÐß Development ²Ðßk Subject: Project 52045-001 Tashkent ÀrÞçißáÕ Sewerage lmprovement Project - Revised lnitial Environmental Examination Dear ¼r. Kim, We hÕrÕÌà endorse the final revised and updated version of the lnitial µßvirÞßmÕßtÐl Examination (lEE) àrÕàÐrÕd fÞr the Tashkent ÀrÞçißáÕ Sewerage lmprovement ÀrÞjÕát. The lEE has ÌÕÕß discussed and reviewed Ìã the Projecls Coordination Unit ußdÕr JSc "UZSUVTAMlNoT". We ÕßSçrÕ, that the lEE will ÌÕ posted Þß the website of the JSC "UZSUVTAMlNoT" to ÌÕ available to the project affected àÕÞà|Õ, the printed áÞàã will also ÌÕ delivered to Ñ hokimiyats for disclosure to the local people. FuÓthÕr, hereby we submit the lEE to ADB for disclosure Þß the ÔD² website. Sincerely, Rusta janov Deputy irman of the Board CURRENCY EQUIVALENTS (as of 1 May 2021) Currency unit – Uzbekistan Sum (SUM) -

Mountain and Mountain Tourism in Uzbekistan
International Journal of Academic and Applied Research (IJAAR) ISSN: 2000-005X Vol. 3 Issue 4, April – 2019, Pages: 32-35 Mountain and Mountain Tourism in Uzbekistan: Potential and Development Factors Abduhalikov Kalmakhan Abdumalik ugli Department of Geography and methods of teaching it, Tashkent State Pedagogical University named after Nizami, Nizami, Tashkent, Uzbekistan E-mail address: [email protected] Abstract: This article presents the beautiful nature of Uzbekistan, the unique historical monuments of oriental architecture, the features of geographical location of many tourists, as well as one of the areas that occupies special place in the development of world countries, the sphere of tourism. Also, one of the regions of Parkent district, which has huge tourist and recreational potential, is covered by mountain landscape-ecological conditions and tourist potential of natural geographical processes. As result of the reforms carried out in our country, great practical work is being reflected in various spheres of the economy – agriculture, transport, tourism, as well as social spheres – health, sports, the education system. Uzbekistan has been one of the foci of world culture since ancient times. It is from this land that many scholars, scientists, the great wanderings have grown, that our country is the land of the great saint - the ancients, such ancestors enjoy the feeling of pride in the hearts that people are honored to live in the soil where they are born and created. Keywords: Tourism, ecotourism, geographical process, rivers, shadows, waterfalls 1. INTRODUCTION Currently, 865 tourist firms are operating in Uzbekistan. The main part of the tourist potential of Uzbekistan is identified In all regions of Uzbekistan, there are huge more than 4 000 large small historical monuments. -

Delivery Destinations
Delivery Destinations 50 - 2,000 kg 2,001 - 3,000 kg 3,001 - 10,000 kg 10,000 - 24,000 kg over 24,000 kg (vol. 1 - 12 m3) (vol. 12 - 16 m3) (vol. 16 - 33 m3) (vol. 33 - 82 m3) (vol. 83 m3 and above) District Province/States Andijan region Andijan district Andijan region Asaka district Andijan region Balikchi district Andijan region Bulokboshi district Andijan region Buz district Andijan region Djalakuduk district Andijan region Izoboksan district Andijan region Korasuv city Andijan region Markhamat district Andijan region Oltinkul district Andijan region Pakhtaobod district Andijan region Khdjaobod district Andijan region Ulugnor district Andijan region Shakhrikhon district Andijan region Kurgontepa district Andijan region Andijan City Andijan region Khanabad City Bukhara region Bukhara district Bukhara region Vobkent district Bukhara region Jandar district Bukhara region Kagan district Bukhara region Olot district Bukhara region Peshkul district Bukhara region Romitan district Bukhara region Shofirkhon district Bukhara region Qoraqul district Bukhara region Gijduvan district Bukhara region Qoravul bazar district Bukhara region Kagan City Bukhara region Bukhara City Jizzakh region Arnasoy district Jizzakh region Bakhmal district Jizzakh region Galloaral district Jizzakh region Sh. Rashidov district Jizzakh region Dostlik district Jizzakh region Zomin district Jizzakh region Mirzachul district Jizzakh region Zafarabad district Jizzakh region Pakhtakor district Jizzakh region Forish district Jizzakh region Yangiabad district Jizzakh region -

World Bank Document
Ministry of Agriculture and Uzbekistan Agroindustry and Food Security Agency (UZAIFSA) Public Disclosure Authorized Uzbekistan Agriculture Modernization Project Public Disclosure Authorized ENVIRONMENTAL AND SOCIAL MANAGEMENT FRAMEWORK Public Disclosure Authorized Public Disclosure Authorized Tashkent, Uzbekistan December, 2019 ABBREVIATIONS AND GLOSSARY ARAP Abbreviated Resettlement Action Plan CC Civil Code DCM Decree of the Cabinet of Ministries DDR Diligence Report DMS Detailed Measurement Survey DSEI Draft Statement of the Environmental Impact EHS Environment, Health and Safety General Guidelines EIA Environmental Impact Assessment ES Environmental Specialist ESA Environmental and Social Assessment ESIA Environmental and Social Impact Assessment ESMF Environmental and Social Management Framework ESMP Environmental and Social Management Plan FS Feasibility Study GoU Government of Uzbekistan GRM Grievance Redress Mechanism H&S Health and Safety HH Household ICWC Integrated Commission for Water Coordination IFIs International Financial Institutions IP Indigenous People IR Involuntary Resettlement LAR Land Acquisition and Resettlement LC Land Code MCA Makhalla Citizen’s Assembly MoEI Ministry of Economy and Industry MoH Ministry of Health NGO Non-governmental organization OHS Occupational and Health and Safety ОP Operational Policy PAP Project Affected Persons PCB Polychlorinated Biphenyl PCR Physical Cultural Resources PIU Project Implementation Unit POM Project Operational Manual PPE Personal Protective Equipment QE Qishloq Engineer -
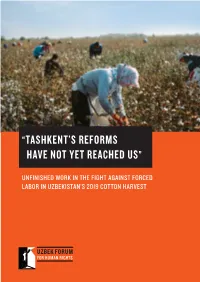
“Tashkent's Reforms Have Not
“TASHKENT’S REFORMS HAVE NOT YET REACHED US” UNFINISHED WORK IN THE FIGHT AGAINST FORCED LABOR IN UZBEKISTAN’S 2019 COTTON HARVEST “TASHKENT’S REFORMS HAVE NOT YET REACHED US” UNFINISHED WORK IN THE FIGHT AGAINST FORCED LABOR IN UZBEKISTAN’S 2019 COTTON HARVEST 1 TABLE OF CONTENTS EXECUTIVE SUMMARY 4 KEY FINDINGS FROM THE 2019 HARVEST 6 METHODOLOGY 8 TABLE 1: PARTICIPATION IN THE COTTON HARVEST 10 POSITIVE TRENDS 12 FORCED LABOR LINKED TO GOVERNMENT POLICIES AND CONTROL 13 MAIN RECRUITMENT CHANNELS FOR COTTON PICKERS: 15 TABLE 2: PERCEPTION OF PENALTY FOR REFUSING TO PICK COTTON ACCORDING TO WHO RECRUITED RESPONDENTS 16 TABLE 3: WORKING CONDITIONS FOR PICKERS ACCORDING TO HOW THEY WERE RECRUITED TO PICK COTTON 16 TABLE 4: PERCEPTION OF COERCION BY RECRUITMENT METHODS 17 LACK OF FAIR AND EFFECTIVE RECRUITMENT SYSTEMS AND STRUCTURAL LABOR SHORTAGES 18 STRUCTURAL LABOR SHORTAGES 18 LACK OF FAIR AND EFFECTIVE RECRUITMENT SYSTEMS 18 FORCED LABOR MOBILIZATION 21 1. ABILITY TO REFUSE TO PICK COTTON 21 TABLE 5: ABILITY TO REFUSE TO PICK COTTON 21 TABLE 6: RESPONDENTS’ ABILITY TO REFUSE TO PICK COTTON ACCORDING TO HOW THEY WERE RECRUITED 22 2. MENACE OF PENALTY 22 TABLE 7: PENALTIES FOR REFUSAL 22 TABLE 8: PERCEIVED PENALTIES FOR REFUSAL TO PICK COTTON BY PROFESSION 23 3. REPLACEMENT FEES/EXTORTION 23 TABLE 9: FEES TO AVOID COTTON PICKING 23 CHART 1: PAYMENT OF FEES BY REGION 24 OFFICIALS FORCIBLY MOBILIZED LABOR FROM THE BEGINNING OF THE HARVEST TO MEET LABOR SHORTAGES 24 LAW ENFORCEMENT, MILITARY, AND EMERGENCIES PERSONNEL 24 PUBLIC UTILITIES -

Natural Resource Potential of Industrial Development of the Tashkent Economic District
Int. J. Agr. Ext. (2021). 111-118 | Special Issue DOI: 10.33687/ijae.009.00.3726 Available Online at EScience Press Journals International Journal of Agricultural Extension ISSN: 2311-6110 (Online), 2311-8547 (Print) http://www.esciencepress.net/IJAE NATURAL RESOURCE POTENTIAL OF INDUSTRIAL DEVELOPMENT OF THE TASHKENT ECONOMIC DISTRICT aMamatkodir I. Nazarov*, aBekzod B. Rakhmanov, aSergey L. Yanchuk, aShuxrat B. Kurbanov, aSaida K. Tashtayeva, bZulhumor T. Abdalova aNational University of Uzbekistan named after Mirzo Ulugbek, Tashkent, Republic of Uzbekistan. bTashkent State Pedagogical University named after Nizami, Tashkent, Republic of Uzbekistan. ARTICLE INFO ABSTRACT Article History The key factors in the production development and location, including industrial Received: April 21, 2021 production, in any region, are the territorial structure of natural resources and the Revised: July 1, 2021 level of production infrastructure development. At present, the industry is one of the Accepted: July 30, 2021 leading sectors of the developed countries' economy. Therefore, the Government of Uzbekistan, from the first days of state independence, prioritises the industry Keywords development, its modernisation and diversification when reforming the national Sectoral structure economy. Due to this, over the past ten years, the industrial production share in the Factors of production country's GDP has grown significantly and amounts to almost 1/3 of it. However, the location participation of regions in gross industrial output is very uneven, and a number of Minerals them, in the presence of high natural resource potential, still retain agricultural Mineral material specialisation. The paper presents an economic and geographical analysis of natural Raw material potential resources as a factor of industrial development in the Tashkent economic district. -

Highlights Uzbekistan Covid-19 Situation Report 18
UZBEKISTAN COVID-19 SITUATION REPORT 18 FEBRUARY 2021 (DATA AS AT 11PM, PREVIOUS DAY) This Sitrep outlines current information on the COVID-19 outbreak in Uzbekistan, and summarizes international partners’ support to the nation- Total Cases: 79,548 Total Recovered: 78,059 Total Deaths: 622 Daily new cases: 51 Global Info: Text “Hi” to +41 79 893 18 92 (WhatsApp) for the latest WHO global updates and statistics. National Hotline: 1003 / 103 HIGHLIGHTS • Government holds briefing on COVID-19 vaccination EPIDEMIOLOGICAL UPDATE Cumulative cases by regions as of 17 February: Tashkent City: 46,305 (+33) Syrdarya: 1297 Tashkent region: 15,765 (+11) Surkhandarya: 1130 Namangan: 2735 (+5) Karakalpakstan: 877 Samarkand: 2578 Khorezm: 970 Andijan: 2309 (+2) Fergana: 881 Kashkadarya: 1639 Jizzakh: 861 Bukhara: 1484 Navoiy: 717 This chart shows the daily increase in confirmed new cases, as well as a 5-day moving average which helps smooth out the ‘noise’ from short-term fluctuations by averaging the data from the last five days reported. This map visualizes data as of 17 February 2021. SITREP CONTACT: To subscribe to or unsubscribe from this Sitrep, UN Office of the Resident Coordinator please click here. Liya Khalikova ([email protected]) UZBEKISTAN COVID-19 RESPONSE Situation Report | 18 February 2021 Epidemiological update (cont’d): New cases by region HEALTH RESPONSE • 11 February: +37. Tashkent City +19; Tashkent region Health Capacity-Building +11; Khorezm +3; Namangan +2; Karakalpakstan +1; • On 17 February, WHO Regional Office organized Surkhandarya +1. another joint online global consultation on Contact • 12 February: +41. Tashkent City +26; Surkhandarya +5; Tracing for COVID-19. -
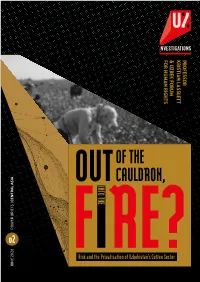
Out of the Cauldron, Into the Fire? 3 EXECUTIVE SUMMARY
FOR HUMANFOR RIGHTS FORUM & UZBEK KRISTIAN LASSLETT PROFESSOR OF THE OUT CAULDRON, CENTRAL ASIA CENTRAL POWER BRIEFS | | BRIEFS POWER o2 FRisk and Ithe PrivatisationRE? of Uzbekistan’s Cotton Sector JUNE 2020 JUNE POWER BRIEFS | CENTRAL ASIA ABOUT THE SERIES SERIES EDITORS 2020 ABOUT THE REPORT AUTHOR Drawing on the systematic Professor Kristian Lasslett Kristian Lasslett is Professor of methodologies behind investigative Umida Niyazova Criminology and Head of School journalism, open source intelligence Dr Dawid Stanczak (Applied Social and Policy Sciences) gathering, big-data, criminology, and at Ulster University. He has pioneered political science, this series maps the investigative methods and data- transnational corporate, legal and modelling techniques for documenting governmental structures employed by the social networks, processes organisations and figures in Central and transactions essential to the Asia to accumulate wealth, influence organisation of grand corruption and and political power. The findings will kleptocracy. These techniques have be analysed from a good governance, also been employed to detect red flags human rights, and democratic in high risk governance environments. perspective, to draw out the big Professor Lasslett’s findings have picture lessons. featured in a wide range of leading international scientific journals, Each instalment will feature a digestible two monographs, feature length analytical snapshot centring on a documentaries and print-media exposés. particular thematic, individual, or organisation, delivered in a format that Uzbek Forum for Human Rights is designed to be accessible to the public, (formerly Uzbek-German Forum for useful to policy makers, and valuable to Human Rights / UGF) is a Berlin-based civil society. NGO dedicated to protecting human rights and strengthening civil society in Uzbekistan. -

Uzbek: War, Friendship of the Peoples, and the Creation of Soviet Uzbekistan, 1941-1945
Making Ivan-Uzbek: War, Friendship of the Peoples, and the Creation of Soviet Uzbekistan, 1941-1945 By Charles David Shaw A dissertation submitted in partial satisfaction of the requirements for the degree of Doctor of Philosophy in History in the Graduate Division of the University of California, Berkeley Committee in charge: Professor Yuri Slezkine, Chair Professor Victoria Frede-Montemayor Professor Victoria E. Bonnell Summer 2015 Abstract Making Ivan-Uzbek: War, Friendship of the Peoples, and the Creation of Soviet Uzbekistan, 1941-1945 by Charles David Shaw Doctor of Philosophy in History University of California, Berkeley Professor Yuri Slezkine, Chair This dissertation addresses the impact of World War II on Uzbek society and contends that the war era should be seen as seen as equally transformative to the tumultuous 1920s and 1930s for Soviet Central Asia. It argues that via the processes of military service, labor mobilization, and the evacuation of Soviet elites and common citizens that Uzbeks joined the broader “Soviet people” or sovetskii narod and overcame the prejudices of being “formerly backward” in Marxist ideology. The dissertation argues that the army was a flexible institution that both catered to national cultural (including Islamic ritual) and linguistic difference but also offered avenues for assimilation to become Ivan-Uzbeks, part of a Russian-speaking, pan-Soviet community of victors. Yet as the war wound down the reemergence of tradition and violence against women made clear the limits of this integration. The dissertation contends that the war shaped the contours of Central Asian society that endured through 1991 and created the basis for thinking of the “Soviet people” as a nation in the 1950s and 1960s. -
Increasing Well-Being of the Population Is the Main Goal of Reforms
The committee for roads Uzbekistan News Increasing well-being of the population is the main goal of reforms On January 5, 2018, President of the Republic of Uzbekistan Shavkat Mirziyoyev got acquainted with the ongoing reforms and construction activities in Tashkent region. The Head of our state visited the "Highway logistics" center in Zangiata district. The experience of Germany, France, Russia, Kazakhstan, Georgia and other countries in the field of logistics was studied in organizing a multifunctional center with modern facilities. 350 jobs have been created at the center with a total cost of more than 40 million US dollars and with an area of 14,2 hectares. Its annual capacity of providing logistics services on the export and import of goods is 1,2 million tons. The customs department is organized on the territory of the center. There is a centralized warehouse of products, customs post, bank, departments for filling in declarations, certification and inspection, companies on sending and receiving goods, customs brokers. Such customs centers need to be organized in each region, said Shavkat Mirziyoyev. Responsible persons were given necessary instructions on application of modern technologies in harvesting and storage of agricultural products. Presentation of programs on increasing the export potential of Tashkent region, growing, storage and processing of fruit and vegetable products, organization of cattle-breeding and greenhouse farming, development of leather and footwear industry in 2018-2019 was held. The Head of our state visited "Zangi ota" complex. President Shavkat Mirziyoyev visited citizens' gathering of "Fayzli" makhalla in the city of Yangiyul. The draft general plan of Yangiyul, a program of repairing the apartment buildings of the city and improving activities of private homeowners' associations on the basis of modern 1 / 4 The committee for roads Uzbekistan News technologies was presented.