Complications of Head and Neck Radiotherapy: a Dental Perspective
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Clinical SHOWCASE Unintentional Replantation: a Technique to Avoid
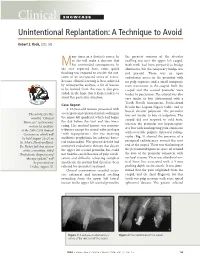
Clinical SHOWCASE Unintentional Replantation: A Technique to Avoid Robert S. Roda, DDS, MS any times in a dentist’s career, he the greatest contour of the alveolar or she will make a decision that swelling was over the upper left cuspid. Mhas unintended consequences. In Both teeth had been prepared as bridge the case reported here, some quick abutments, but the temporary bridge was thinking was required to resolve the out- not present. There was an open come of an unexpected series of events. endodontic access in the premolar with Because clinical learning is best achieved no pulp exposure and a small composite by retrospective analysis, a list of lessons resin restoration in the cuspid. Both the to be learned from this case is also pro- cuspid and the second premolar were vided, in the hope that it helps readers to tender to percussion. The cuspid was also avoid this particular situation. very tender to bite (determined with a Tooth Slooth instrument, Professional Case Report Results Inc, Laguna Niguel, Calif.) and to A 63-year-old woman presented with buccal alveolar palpation. The premolar severe pain and extraoral facial swelling in The articles for this was not tender to bite or palpation. The the upper left quadrant, which had begun month’s “Clinical cuspid did not respond to cold tests, the day before the visit and was wors- Showcase” section were whereas the premolar was hyperrespon- ening. Her medical history was noncon- written by speakers sive but with nonlingering pain consistent at the 2006 CDA Annual tributory except for mitral valve prolapse with reversible pulpitis. -

Oral Diagnosis: the Clinician's Guide
Wright An imprint of Elsevier Science Limited Robert Stevenson House, 1-3 Baxter's Place, Leith Walk, Edinburgh EH I 3AF First published :WOO Reprinted 2002. 238 7X69. fax: (+ 1) 215 238 2239, e-mail: [email protected]. You may also complete your request on-line via the Elsevier Science homepage (http://www.elsevier.com). by selecting'Customer Support' and then 'Obtaining Permissions·. British Library Cataloguing in Publication Data A catalogue record for this book is available from the British Library Library of Congress Cataloging in Publication Data A catalog record for this book is available from the Library of Congress ISBN 0 7236 1040 I _ your source for books. journals and multimedia in the health sciences www.elsevierhealth.com Composition by Scribe Design, Gillingham, Kent Printed and bound in China Contents Preface vii Acknowledgements ix 1 The challenge of diagnosis 1 2 The history 4 3 Examination 11 4 Diagnostic tests 33 5 Pain of dental origin 71 6 Pain of non-dental origin 99 7 Trauma 124 8 Infection 140 9 Cysts 160 10 Ulcers 185 11 White patches 210 12 Bumps, lumps and swellings 226 13 Oral changes in systemic disease 263 14 Oral consequences of medication 290 Index 299 Preface The foundation of any form of successful treatment is accurate diagnosis. Though scientifically based, dentistry is also an art. This is evident in the provision of operative dental care and also in the diagnosis of oral and dental diseases. While diagnostic skills will be developed and enhanced by experience, it is essential that every prospective dentist is taught how to develop a structured and comprehensive approach to oral diagnosis. -

Cracked Tooth Syndrome, an Update
International Journal of Applied Dental Sciences 2021; 7(2): 314-317 ISSN Print: 2394-7489 ISSN Online: 2394-7497 IJADS 2021; 7(2): 314-317 Cracked tooth syndrome, an update © 2021 IJADS www.oraljournal.com Received: 19-02-2021 Dariela Isabel Gonzalez-Guajardo, Guadalupe Magdalena Ramirez- Accepted: 21-03-2021 Herrera, Alejandro Mas-Enriquez, Guadalupe Rosalia Capetillo- Dariela Isabel Gonzalez-Guajardo Hernandez, Leticia Tiburcio-Morteo, Claudio Cabral-Romero, Rene Master in Sciences Student, Hernandez-Delgadillo and Juan Manuel Solis-Soto Universidad Autonoma de Nuevo Leon, Facultad de Odontologia, Monterrey, Nuevo Leon, CP 64460, DOI: https://doi.org/10.22271/oral.2021.v7.i2e.1226 Mexico Guadalupe Magdalena Ramirez- Abstract Herrera Introduction: Cracked tooth syndrome is defined as an incomplete fracture initiated from the crown and Professor, Universidad Autonoma de extending cervically, and sometimes gingivally, and is usually directed mesiodistally. Objective: To Nuevo Leon, Facultad de analyze the literature about cracked tooth syndrome, its etiology, prevalence, pulp involvement and Odontologia, Monterrey, Nuevo Leon, CP 64460, Mexico treatment. Methodology: Using the keywords “cracked tooth syndrome”, “etiology”, “prevalence”, “pulp Alejandro Mas-Enriquez involvement” and “treatment”, the MEDLINE/PubMed and ScienceDirect databases were searched, with Associate Professor, Universidad emphasis on the last 5 years. It was evaluated with the PRISMA and AMSTAR-2 guidelines. Autonoma de Nuevo Leon, Facultad de Odontologia, Monterrey, Nuevo Results: There are many causes for cracks, the main one being malocclusion. Another is due to Leon, CP 64460, Mexico restorations, pieces to which amalgam was placed due to the extension of the cavity for the retentions. The second lower molar presents more frequently fissures due to premature contact. -

Orofacial Pain
QUINTESSENCE INTERNATIONAL OROFACIAL PAIN Noboru Noma Cracked tooth syndrome mimicking trigeminal autonomic cephalalgia: A report of four cases Noboru Noma DDS, PhD1/Kohei Shimizu DDS, PhD2/Kosuke Watanabe DDS3/Andrew Young DDS, MSD4/ Yoshiki Imamura DDS, PhD5/Junad Khan BDS, MSD, MPH, PhD6 Background: This report describes four cases of cracked All cases mimicked trigeminal autonomic cephalalgias, a group tooth syndrome secondary to traumatic occlusion that mim- of primary headache disorders characterized by unilateral icked trigeminal autonomic cephalalgias. All patients were facial pain and ipsilateral cranial autonomic symptoms. referred by general practitioners to the Orofacial Pain Clinic at Trigeminal autonomic cephalalgias include cluster headache, Nihon University Dental School for assessment of atypical facial paroxysmal hemicrania, hemicrania continua, and short-lasting pain. Clinical Presentation: Case 1: A 51-year-old woman unilateral neuralgiform headache attacks with conjunctival presented with severe pain in the maxillary and mandibular injection and tearing/short-lasting neuralgiform headache left molars. Case 2: A 47-year-old woman presented with sharp, attacks with cranial autonomic features. Pulpal necrosis, when shooting pain in the maxillary left molars, which radiated to caused by cracked tooth syndrome, can manifest with pain the temple and periorbital region. Case 3: A 49-year-old man frequencies and durations that are unusual for pulpitis, as was presented with sharp, shooting, and stabbing pain in the max- seen in these cases. Conclusion: Although challenging, dif- illary left molars. Case 4: A 38-year-old man presented with ferentiation of cracked tooth syndrome from trigeminal intense facial pain in the left supraorbital and infraorbital areas, autonomic cephalalgias is a necessary skill for dentists. -

Pulp Canal Obliteration After Traumatic Injuries in Permanent Teeth – Scientific Fact Or Fiction?
CRITICAL REVIEW Endodontic Therapy Pulp canal obliteration after traumatic injuries in permanent teeth – scientific fact or fiction? Juliana Vilela BASTOS(a) Abstract: Pulp canal obliteration (PCO) is a frequent finding associated (b) Maria Ilma de Souza CÔRTES with pulpal revascularization after luxation injuries of young permanent teeth. The underlying mechanisms of PCO are still unclear, (a) Universidade Federal de Minas Gerais - and no experimental scientific evidence is available, except the results UFMG, School of Dentistry, Department of Restorative Dentistry, Belo Horizonte, MG, of a single histopathological study. The lack of sound knowledge Brazil. concerning this process gives rise to controversies, including the (b) Pontifícia Universidade Católica de Minas most suitable denomination. More than a mere semantic question, Gerais – PUC-MG, Department of Dentistry, the denomination is an important issue, because it reflects the nature Belo Horizonte, MG, Brazil. of this process, and directly impacts the treatment plan decision. The hypothesis that accelerated dentin deposition is related to the loss of neural control over odontoblastic secretory activity is well accepted, but demands further supportive studies. PCO is seen radiographically as a rapid narrowing of pulp canal space, whereas common clinical features are yellow crown discoloration and a lower or non-response to sensibility tests. Late development of pulp necrosis and periapical disease are rare complications after PCO, rendering prophylactic endodontic intervention -

Disease of Pulp and Periradicular Tissue: an Overview
Journal of Current Medical Research and Opinion Received 16-09-2020 | Accepted 10-10-2020 | Published Online 11--10-2020 DOI: https://doi.org/10.15520/jcmro.v3i10.351 ISSN (O) 2589-8779 | (P) 2589-8760 CMRO 11 (10), 652−664 (2020) REVIEW ARTICLE Disease of Pulp and Periradicular Tissue: An Overview ∗ Geetanjali Singh1 Sanjana Paul R2 Ayush Arora3 Shakti Kumar4 Lucky Jindal5 Sachin Raina6 1Senior Lecturer, Department of Abstract: Prosthodontics, Crown, Bridge Dental pain is the most common reason due to which patient seek dental and Implantology, Himachal treatment. Pain occur due to diseases involving pulp and periradicular Dental College, Sundernagar, Himachal Pradesh tissues, as these tissues are richly innervated and have ample of blood supply. Also it is enclosed by surrounding tissues that are incapable 2Consultant Endodontist, Kanyakumari, Tamil Nadu of expanding, such as dentin and also has terminal blood flow and small-gauge circulatory access the periapex. All of these characteristics 3Consultant Dental Surgeon, severely constrain the defensive capacity of the pulp tissue when faced Jaipur, Rajasthan with the different aggressions it may be subjected to. In addition to above mentioned characterstics, pulp tissue can also be affected by a 4Consultant Orthodontist, Sirsa, Haryana retrograde infection, arising from the secondary canaliculi, from the periodontal ligament or from the apex during the course of periodontitis. 5Senior Lecturer, Department of Paedodontics and Preventive this review article basically concentrates on structure -

Quality Resource Guide Diagnosing and Managing the Cracked Tooth Part 1: Crown-Originating Fractures
MetLife designates this activity for 1.5 continuing education credit for the review of this Quality Resource Guide Quality Resource Guide and successful completion of the post test. Diagnosing and Managing the Cracked Tooth Part 1: Crown-Originating Fractures FIRST EDITION Educational Objectives Following this unit of instruction, the practitioner should be able to: Author Acknowledgements Leif K. Bakland, DDS 1. Describe the three categories of dental fractures. Emeritus Professor 2. Recognize the usual symptoms of crown-originating fractures. Tory Silvestrin, DDS 3. Recognize the role of radiography in diagnosis of crown-originating fractures. Assistant Professor Loma Linda University, School of Dentistry 4. Describe the clinical tests used for identifying teeth with crown-originating fractures. Loma Linda, California 5. Describe treatment options for crown-originating fractures. Drs. Bakland and Silvestrin have no relevant relationships to disclose. 6. Develop a prognosis for a crown-originating fracture. The following commentary highlights fundamental and commonly accepted practices on the subject matter. The information is Introduction intended as a general overview and is for The term ‘cracked tooth’ has been used to describe Table 1 educational purposes only. This information many types of fractures and cracks in teeth. Other terms Terms Used For Dental Fractures does not constitute legal advice, which can only be provided by an attorney. have also been used (Table 1) for this dental problem, Cracked tooth © Metropolitan Life Insurance Company, indicating that dentistry has not previously been able to Cracked tooth syndrome New York, NY. All materials subject to develop a generally accepted categorization scheme. Green stick fracture this copyright may be photocopied for the 1 noncommercial purpose of scientific or Efforts have been made over the years. -

Itching Gingiva: an Early Sign of Pre-Inflammatory Pulp Necrosis Or Unsuccessful Endodontic Treatment: a Case Series
Journal of Oral Care and Dentistry Volume 1| Issue 9 Case Report Open Access Itching Gingiva: An Early Sign Of Pre-Inflammatory Pulp Necrosis or Unsuccessful Endodontic Treatment: A case series Fendi Alshaarani1, DDS, MSc, PhD, Imad Barngkgei2, DDS, MSc, PhD, Easter Joury3 BDS, DOrth, MSc (Lond), PhD (Lond), MFDS RCPS(Glasg), Kanaan Elias4 DDS, MSc, PhD. 1Department of Fixed Prosthodontics, Faculty of Dentistry, Damascus University, Damascus, Syria. 2Department of Oral Medicine, Faculty of Dentistry, Syrian Private University, Damascus, Syria. 3Population and Patient Health, King’s College London Dental Institute, Denmark Hill Campus, Bessemer Road, London, United Kingdom, SE5 9RS. 4Eastman Dental Institute, University College London. *Corresponding author: Dr. Imad Barngkgei, DDS, MSc, PhD, Department of Oral Medicine, Faculty of Dentistry, Syrian Private University, Damascus, Syria; Email: [email protected] Citation: Imad Barngkgei (2018) Itching Gingiva: An Early Sign Of Pre-Inflammatory Pulp Necrosis Or Unsuccessful Endodontic Treatment: A case series;Nessa J Oral Care and Dentistry Received: 11th August 2018, Accepted: 17th September 2018, Published: 2nd November 2018. Copyright: © 2018 Imad Barngkgei et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Abstract There is no report in the literature regarding the presence of an early sign of pulp necrosis preceding pulpal pain, incomplete endodontic fillings or radiographically complete endodontic fillings performed under unsterilized conditions. In this case series, we described four cases that had a common compliant of itching gingiva. The gingival itching, from which they suffered, disappeared after performing/redoing the endodontic treatment. -

DISORDERS of the PULP & PERIPAICAL TISSUES Prepared By
Diseases Of Pulp & Periapical Tissues By Dr. Intisar Ben Amer PULPITIS Pulpitis is the most common cause of pain and loss of teeth in younger persons. The usual cause is caries penetrating the dentine but there are other possibilities of pulpitis . If untreated, is followed by death of the pulp and spread of infection through the apical foramina into the periapical tissue . CAUSES OF PULP DISEASE The causes of pulp disease are Physical, Chemical and Bacterial. Physical a. Mechanical - Trauma: . Accidental . Iatrogenic dental procedures - Pathological wear - Crack through body of tooth b. Thermal - Heat from cavity preparation - Exothermic heat from setting of cements c. Electrical ( galvanic current from dissimilar metallic filling) 2. Chemical -Phosphoric acid, acrylic monomer, etc. -Erosion (acids) 3. Bacterial -Toxin associated with caries -Direct invasion of pulp from caries or trauma -Microbial colonization in the pulp by blood-borne microorganisms. CLASSIFICATION I. According to pathological condition: - - Focal or acute reversible pulpitis (Pulp hyperaemia) - Irreversible pulpitis II. According to its duration: - - Acute pulpitis - Chronic pulpitis III. According to presence of dentin covering the pulp chamber: - - Open pulpitis - Closed pulpitis CLASSIFICATION IV. According to extension of inflammation in pulp tissue: - - Partial pulpitis - Complete / total pulpitis V. According to amount of pus formation: - - Exudative pulpitis - Suppurative pulpitis FOCAL REVERSIBLE PULPITIS (PULP HYPEREMIA) Mild, transient, localized inflammatory response. It is a reversible condition . CLINICAL FEATURES: Tooth is sensitive to thermal changes, especially cold. Pain - short duration, disappears on withdrawal of irritant. Affected tooth responds to stimulation of electric pulp tester at lower level of current indicating low pain threshold. Teeth usually show deep caries, metallic restoration with defective margins. -
Strategies for the Endodontic Management of Concurrent Endodontic and Periodontal Diseases
Australian Dental Journal 2009; 54:(1 Suppl): S70–S85 doi: 10.1111/j.1834-7819.2009.01145.x Strategies for the endodontic management of concurrent endodontic and periodontal diseases PV Abbott,* J Castro Salgado* *School of Dentistry, The University of Western Australia. ABSTRACT Endodontic and periodontal diseases can provide many diagnostic and management challenges to clinicians, particularly when they occur concurrently. As with all diseases, a thorough history combined with comprehensive clinical and radiographic examinations are all required so an accurate diagnosis can be made. This is essential since the diagnosis will determine the type and sequence of treatment required. This paper reviews the relevant literature and proposes a new classification for concurrent endodontic and periodontal diseases. This classification is a simple one that will help clinicians to formulate management plans for when these diseases occur concurrently. The key aspects are to determine whether both types of diseases are present, rather than just having manifestations of one disease in the alternate tissue. Once it is established that both diseases are present and that they are as a result of infections of each tissue, then the clinician must determine whether the two diseases communicate via the periodontal pocket so that appropriate management can be provided using the guidelines outlined. In general, if the root canal system is infected, endodontic treatment should be commenced prior to any periodontal therapy in order to remove the intracanal infection before any cementum is removed. This avoids several complications and provides a more favourable environment for periodontal repair. The endodontic treatment can be completed before periodontal treatment is provided when there is no communication between the disease processes. -

Evaluation of Pathological Microbes in Root Canals with Pulp Necrosis
ORIGINAL RESEARCH Evaluation of Pathological Microbes in Root Canals with Pulp Necrosis Atul Anand Bajoria1, Ahmed Ali Alfawzan2, Vardharajula Venkata Ramaiah3, Mohammed Ali Habibullah4, Sabahat Ullah Tareen5, Prashant Babaji6 ABSTRACT Aim: The present study was conducted to evaluate the type of bacteria present in necrotic root canals of permanent teeth. Materials and methods: All 60 participants with infected root canals were made to use 10 mL of mouthwash containing 0.12% chlorhexidine. Access to pulp chamber was established, and the sterile absorbent paper cones were inserted into the canal for 20 seconds. The contaminated paper cones were inoculated in a brain–heart infusion (BHI) agar culture medium and incubated in an oven for 48 hours at 37°C. Results were analyzed statistically with SPSS version 20.0 using Chi-square test and analysis of variance (ANOVA). Results: In root canals with periapical lesions, gram-positive bacilli was present in 50 cases, gram-negative in 48 and yeast cells in 28; while in root canals without periapical lesions, gram-positive bacilli was present in 8. In 16 root canals of chronic apical periodontitis cases, gram-positive bacteria was present in 100%, gram-negative bacteria in 100%, and yeast cells in 20% cases. In 12 cases of periapical granuloma, gram-positive bacteria was present in 98%, gram-negative bacteria in 100%, and yeast cells in 40% cases. In 10 cases of chronic abscess with fistula, gram- positive bacteria was present in 86.2. In six cases of phoenix abscess, gram-positive bacteria was present in 100% and gram-negative bacteria in 100% cases. -

1 – Pathogenesis of Pulp and Periapical Diseases
1 Pathogenesis of Pulp and Periapical Diseases CHRISTINE SEDGLEY, RENATO SILVA, AND ASHRAF F. FOUAD CHAPTER OUTLINE Histology and Physiology of Normal Dental Pulp, 1 Normal Pulp, 11 Etiology of Pulpal and Periapical Diseases, 2 Reversible Pulpitis, 11 Microbiology of Root Canal Infections, 5 Irreversible Pulpitis, 11 Endodontic Infections Are Biofilm Infections, 5 Pulp Necrosis, 12 The Microbiome of Endodontic Infections, 6 Clinical Classification of Periapical (Apical) Conditions, 13 Pulpal Diseases, 8 Nonendodontic Pathosis, 15 LEARNING OBJECTIVES After reading this chapter, the student should be able to: 6. Describe the histopathological diagnoses of periapical lesions of 1. Describe the histology and physiology of the normal dental pulpal origin. pulp. 7. Identify clinical signs and symptoms of acute apical periodon- 2. Identify etiologic factors causing pulp inflammation. titis, chronic apical periodontitis, acute and chronic apical 3. Describe the routes of entry of microorganisms to the pulp and abscesses, and condensing osteitis. periapical tissues. 8. Discuss the role of residual microorganisms and host response 4. Classify pulpal diseases and their clinical features. in the outcome of endodontic treatment. 5. Describe the clinical consequences of the spread of pulpal 9. Describe the steps involved in repair of periapical pathosis after inflammation into periapical tissues. successful root canal treatment. palisading layer that lines the walls of the pulp space, and their Histology and Physiology of Normal Dental tubules extend about two thirds of the length of the dentinal Pulp tubules. The tubules are larger at a young age and eventually become more sclerotic as the peritubular dentin becomes thicker. The dental pulp is a unique connective tissue with vascular, lym- The odontoblasts are primarily involved in production of mineral- phatic, and nervous elements that originates from neural crest ized dentin.