Radiological and Histopathological Features of Internal Tooth Resorption TILL KOEHNE 1, JOZEF ZUSTIN 2, MICHAEL AMLING 2 and REINHARD E
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Glossary for Narrative Writing
Periodontal Assessment and Treatment Planning Gingival description Color: o pink o erythematous o cyanotic o racial pigmentation o metallic pigmentation o uniformity Contour: o recession o clefts o enlarged papillae o cratered papillae o blunted papillae o highly rolled o bulbous o knife-edged o scalloped o stippled Consistency: o firm o edematous o hyperplastic o fibrotic Band of gingiva: o amount o quality o location o treatability Bleeding tendency: o sulcus base, lining o gingival margins Suppuration Sinus tract formation Pocket depths Pseudopockets Frena Pain Other pathology Dental Description Defective restorations: o overhangs o open contacts o poor contours Fractured cusps 1 ww.links2success.biz [email protected] 914-303-6464 Caries Deposits: o Type . plaque . calculus . stain . matera alba o Location . supragingival . subgingival o Severity . mild . moderate . severe Wear facets Percussion sensitivity Tooth vitality Attrition, erosion, abrasion Occlusal plane level Occlusion findings Furcations Mobility Fremitus Radiographic findings Film dates Crown:root ratio Amount of bone loss o horizontal; vertical o localized; generalized Root length and shape Overhangs Bulbous crowns Fenestrations Dehiscences Tooth resorption Retained root tips Impacted teeth Root proximities Tilted teeth Radiolucencies/opacities Etiologic factors Local: o plaque o calculus o overhangs 2 ww.links2success.biz [email protected] 914-303-6464 o orthodontic apparatus o open margins o open contacts o improper -
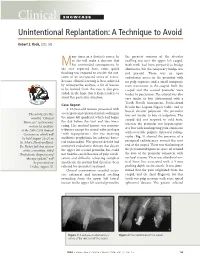
Clinical SHOWCASE Unintentional Replantation: a Technique to Avoid
Clinical SHOWCASE Unintentional Replantation: A Technique to Avoid Robert S. Roda, DDS, MS any times in a dentist’s career, he the greatest contour of the alveolar or she will make a decision that swelling was over the upper left cuspid. Mhas unintended consequences. In Both teeth had been prepared as bridge the case reported here, some quick abutments, but the temporary bridge was thinking was required to resolve the out- not present. There was an open come of an unexpected series of events. endodontic access in the premolar with Because clinical learning is best achieved no pulp exposure and a small composite by retrospective analysis, a list of lessons resin restoration in the cuspid. Both the to be learned from this case is also pro- cuspid and the second premolar were vided, in the hope that it helps readers to tender to percussion. The cuspid was also avoid this particular situation. very tender to bite (determined with a Tooth Slooth instrument, Professional Case Report Results Inc, Laguna Niguel, Calif.) and to A 63-year-old woman presented with buccal alveolar palpation. The premolar severe pain and extraoral facial swelling in The articles for this was not tender to bite or palpation. The the upper left quadrant, which had begun month’s “Clinical cuspid did not respond to cold tests, the day before the visit and was wors- Showcase” section were whereas the premolar was hyperrespon- ening. Her medical history was noncon- written by speakers sive but with nonlingering pain consistent at the 2006 CDA Annual tributory except for mitral valve prolapse with reversible pulpitis. -

Oral Diagnosis: the Clinician's Guide
Wright An imprint of Elsevier Science Limited Robert Stevenson House, 1-3 Baxter's Place, Leith Walk, Edinburgh EH I 3AF First published :WOO Reprinted 2002. 238 7X69. fax: (+ 1) 215 238 2239, e-mail: [email protected]. You may also complete your request on-line via the Elsevier Science homepage (http://www.elsevier.com). by selecting'Customer Support' and then 'Obtaining Permissions·. British Library Cataloguing in Publication Data A catalogue record for this book is available from the British Library Library of Congress Cataloging in Publication Data A catalog record for this book is available from the Library of Congress ISBN 0 7236 1040 I _ your source for books. journals and multimedia in the health sciences www.elsevierhealth.com Composition by Scribe Design, Gillingham, Kent Printed and bound in China Contents Preface vii Acknowledgements ix 1 The challenge of diagnosis 1 2 The history 4 3 Examination 11 4 Diagnostic tests 33 5 Pain of dental origin 71 6 Pain of non-dental origin 99 7 Trauma 124 8 Infection 140 9 Cysts 160 10 Ulcers 185 11 White patches 210 12 Bumps, lumps and swellings 226 13 Oral changes in systemic disease 263 14 Oral consequences of medication 290 Index 299 Preface The foundation of any form of successful treatment is accurate diagnosis. Though scientifically based, dentistry is also an art. This is evident in the provision of operative dental care and also in the diagnosis of oral and dental diseases. While diagnostic skills will be developed and enhanced by experience, it is essential that every prospective dentist is taught how to develop a structured and comprehensive approach to oral diagnosis. -

Establishment of a Dental Effects of Hypophosphatasia Registry Thesis
Establishment of a Dental Effects of Hypophosphatasia Registry Thesis Presented in Partial Fulfillment of the Requirements for the Degree Master of Science in the Graduate School of The Ohio State University By Jennifer Laura Winslow, DMD Graduate Program in Dentistry The Ohio State University 2018 Thesis Committee Ann Griffen, DDS, MS, Advisor Sasigarn Bowden, MD Brian Foster, PhD Copyrighted by Jennifer Laura Winslow, D.M.D. 2018 Abstract Purpose: Hypophosphatasia (HPP) is a metabolic disease that affects development of mineralized tissues including the dentition. Early loss of primary teeth is a nearly universal finding, and although problems in the permanent dentition have been reported, findings have not been described in detail. In addition, enzyme replacement therapy is now available, but very little is known about its effects on the dentition. HPP is rare and few dental providers see many cases, so a registry is needed to collect an adequate sample to represent the range of manifestations and the dental effects of enzyme replacement therapy. Devising a way to recruit patients nationally while still meeting the IRB requirements for human subjects research presented multiple challenges. Methods: A way to recruit patients nationally while still meeting the local IRB requirements for human subjects research was devised in collaboration with our Office of Human Research. The solution included pathways for obtaining consent and transferring protected information, and required that the clinician providing the clinical data refer the patient to the study and interact with study personnel only after the patient has given permission. Data forms and a custom database application were developed. Results: The registry is established and has been successfully piloted with 2 participants, and we are now initiating wider recruitment. -

The Cat Mandible (II): Manipulation of the Jaw, with a New Prosthesis Proposal, to Avoid Iatrogenic Complications
animals Review The Cat Mandible (II): Manipulation of the Jaw, with a New Prosthesis Proposal, to Avoid Iatrogenic Complications Matilde Lombardero 1,*,† , Mario López-Lombardero 2,†, Diana Alonso-Peñarando 3,4 and María del Mar Yllera 1 1 Unit of Veterinary Anatomy and Embryology, Department of Anatomy, Animal Production and Clinical Veterinary Sciences, Faculty of Veterinary Sciences, Campus of Lugo—University of Santiago de Compostela, 27002 Lugo, Spain; [email protected] 2 Engineering Polytechnic School of Gijón, University of Oviedo, 33203 Gijón, Spain; [email protected] 3 Department of Animal Pathology, Faculty of Veterinary Sciences, Campus of Lugo—University of Santiago de Compostela, 27002 Lugo, Spain; [email protected] 4 Veterinary Clinic Villaluenga, calle Centro n◦ 2, Villaluenga de la Sagra, 45520 Toledo, Spain * Correspondence: [email protected]; Tel.: +34-982-822-333 † Both authors contributed equally to this manuscript. Simple Summary: The small size of the feline mandible makes its manipulation difficult when fixing dislocations of the temporomandibular joint or mandibular fractures. In both cases, non-invasive techniques should be considered first. When not possible, fracture repair with internal fixation using bone plates would be the best option. Simple jaw fractures should be repaired first, and caudal to rostral. In addition, a ventral approach makes the bone fragments exposure and its manipulation easier. However, the cat mandible has little space to safely place the bone plate screws without damaging the tooth roots and/or the mandibular blood and nervous supply. As a consequence, we propose a conceptual model of a mandibular prosthesis that would provide biomechanical Citation: Lombardero, M.; stabilization, avoiding any unintended (iatrogenic) damage to those structures. -

Cracked Tooth Syndrome, an Update
International Journal of Applied Dental Sciences 2021; 7(2): 314-317 ISSN Print: 2394-7489 ISSN Online: 2394-7497 IJADS 2021; 7(2): 314-317 Cracked tooth syndrome, an update © 2021 IJADS www.oraljournal.com Received: 19-02-2021 Dariela Isabel Gonzalez-Guajardo, Guadalupe Magdalena Ramirez- Accepted: 21-03-2021 Herrera, Alejandro Mas-Enriquez, Guadalupe Rosalia Capetillo- Dariela Isabel Gonzalez-Guajardo Hernandez, Leticia Tiburcio-Morteo, Claudio Cabral-Romero, Rene Master in Sciences Student, Hernandez-Delgadillo and Juan Manuel Solis-Soto Universidad Autonoma de Nuevo Leon, Facultad de Odontologia, Monterrey, Nuevo Leon, CP 64460, DOI: https://doi.org/10.22271/oral.2021.v7.i2e.1226 Mexico Guadalupe Magdalena Ramirez- Abstract Herrera Introduction: Cracked tooth syndrome is defined as an incomplete fracture initiated from the crown and Professor, Universidad Autonoma de extending cervically, and sometimes gingivally, and is usually directed mesiodistally. Objective: To Nuevo Leon, Facultad de analyze the literature about cracked tooth syndrome, its etiology, prevalence, pulp involvement and Odontologia, Monterrey, Nuevo Leon, CP 64460, Mexico treatment. Methodology: Using the keywords “cracked tooth syndrome”, “etiology”, “prevalence”, “pulp Alejandro Mas-Enriquez involvement” and “treatment”, the MEDLINE/PubMed and ScienceDirect databases were searched, with Associate Professor, Universidad emphasis on the last 5 years. It was evaluated with the PRISMA and AMSTAR-2 guidelines. Autonoma de Nuevo Leon, Facultad de Odontologia, Monterrey, Nuevo Results: There are many causes for cracks, the main one being malocclusion. Another is due to Leon, CP 64460, Mexico restorations, pieces to which amalgam was placed due to the extension of the cavity for the retentions. The second lower molar presents more frequently fissures due to premature contact. -

Feline Tooth Resorption Feline Odontoclastic Resorptive Lesions (FORL)
Feline Tooth Resorption Feline Odontoclastic Resorptive Lesions (FORL) What is tooth resorption? Tooth resorption is a destructive process that eats away at teeth and is quite common in cats. Up to 50% of cats over the age of 8 will have resorptive lesions. Of those 50% with lesions, 50% of them will have more than one. This process can be very painful, and due to the nature of the cat, many will not show obvious signs of pain. These lesions will often require immediate treatment. Feline tooth resorption does progress and will require treatment to avoid pain and loss of function. This process is not necessarily preventable, but studies do show that cats who do not receive oral hygiene care are at an increased risk of development of resorptive lesions. Feline patients diagnosed with Feline Immunodeficiency Virus and Feline Leukemia Virus are also more likely to develop lesions. Despite the health status of your cat, it is important to know tooth resorption is a common and treatable disease. What causes tooth resorption? Tooth resorption is an idiopathic disease of the teeth. This means that the cause is unknown. We do know odontoclasts, the cat’s own cells, begin to destroy the structure of the tooth. Sometimes resorption will be associated with a tooth root abscess, although this is uncommon. What are the clinical signs of this? Cats with tooth resorption will often have inflammation of the gum tissue surrounding the affected tooth. Your veterinarian will comment on the teeth and gums during the oral part of the physical examination. Even though an oral exam is done, many of these lesions are below the gum line and require dental radiography to fully diagnose. -

Feline Alveolar Osteitis Treatment Planning: Implant Protocol with Osseodensification and Early Crown Placement Rocco E
Feline Alveolar Osteitis Treatment Planning: Implant Protocol with Osseodensification and Early Crown Placement Rocco E. Mele DVM1, Gregori M. Kurtzman, DDS, MAGD, DICOI,DIDIA2 1 Eastpoint Pet Clinic, Tucson, A, USA 2 Silver Spring, MD, USA Abstract: Feline dental implants are becoming a predictable and viable treatment option for the replacement of lost canines due to maxillary Alveolar Osteitis (AO) a painful condition, commonly experienced by a growing number of cats. Surgical extraction and debridement remains the treatment of choice for this complex inflammatory process. However, future complications can be a common sequela of maxillary canine loss. This case will demonstrate the successful surgical extraction of a maxillary canine with implant placement following the osseodensification protocol and utilizing the sockets osteitis buttressing bone formation to promote a positive result with final crown restoration 13 weeks following implant placement. Introduction: Alveolar Osteitis (AO) is a chronic inflammatory process more often diagnosed in maxillary canine sockets of the feline patient. Clinical presentation may include oral pain, bleeding, periodontitis, tooth resorption (ORL), and alveolar buccal bone changes.1-5 Clinical Features: A presumptive diagnosis of (AO) is made on the awake patient, documenting clinical features such as; gingivitis with soft tissue swelling, gingival mucosal erythema, buccal bone expansion, and coronal extrusion. (Figure 1) Radiographic Features: Radiographic changes are identified under general anesthesia. These bony changes and pathology may include; deep palatal probing (Figure 2 red), alveolar bone expansion (Figure 2 green), buttressing condensing bone (Figure 2 blue) and a mottled osseous appearance mimicking rough, large trabeculae (Figure 2 yellow) Osseodensification (OD): OD is a novel biomechanical bone preparation technique for dental implant placement to improve bone quality by increasing its density utilizing Densah burs. -

Orofacial Pain
QUINTESSENCE INTERNATIONAL OROFACIAL PAIN Noboru Noma Cracked tooth syndrome mimicking trigeminal autonomic cephalalgia: A report of four cases Noboru Noma DDS, PhD1/Kohei Shimizu DDS, PhD2/Kosuke Watanabe DDS3/Andrew Young DDS, MSD4/ Yoshiki Imamura DDS, PhD5/Junad Khan BDS, MSD, MPH, PhD6 Background: This report describes four cases of cracked All cases mimicked trigeminal autonomic cephalalgias, a group tooth syndrome secondary to traumatic occlusion that mim- of primary headache disorders characterized by unilateral icked trigeminal autonomic cephalalgias. All patients were facial pain and ipsilateral cranial autonomic symptoms. referred by general practitioners to the Orofacial Pain Clinic at Trigeminal autonomic cephalalgias include cluster headache, Nihon University Dental School for assessment of atypical facial paroxysmal hemicrania, hemicrania continua, and short-lasting pain. Clinical Presentation: Case 1: A 51-year-old woman unilateral neuralgiform headache attacks with conjunctival presented with severe pain in the maxillary and mandibular injection and tearing/short-lasting neuralgiform headache left molars. Case 2: A 47-year-old woman presented with sharp, attacks with cranial autonomic features. Pulpal necrosis, when shooting pain in the maxillary left molars, which radiated to caused by cracked tooth syndrome, can manifest with pain the temple and periorbital region. Case 3: A 49-year-old man frequencies and durations that are unusual for pulpitis, as was presented with sharp, shooting, and stabbing pain in the max- seen in these cases. Conclusion: Although challenging, dif- illary left molars. Case 4: A 38-year-old man presented with ferentiation of cracked tooth syndrome from trigeminal intense facial pain in the left supraorbital and infraorbital areas, autonomic cephalalgias is a necessary skill for dentists. -

An Insight Into Internal Resorption
Hindawi Publishing Corporation ISRN Dentistry Volume 2014, Article ID 759326, 7 pages http://dx.doi.org/10.1155/2014/759326 Review Article An Insight into Internal Resorption Priya Thomas, Rekha Krishna Pillai, Bindhu Pushparajan Ramakrishnan, and Jayanthi Palani Department of Oral and Maxillofacial Pathology, Annoor Dental College & Hospital, Muvattupuzha, Ernakulam District, Kerala 686673, India Correspondence should be addressed to Priya Thomas; [email protected] Received 20 January 2014; Accepted 27 March 2014; Published 12 May 2014 Academic Editors: S.-C. Choi and G. Mount Copyright © 2014 Priya Thomas et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Internal resorption, a rare phenomenon, has been a quandary from the standpoints of both its diagnosis and treatment. It is usually asymptomatic and discovered by chance on routine radiographic examinations or by a classic clinical sign, “pink spot” in the crown. This paper emphasizes the etiology and pathophysiologic mechanisms involved in internal root resorption. Prognosis is good for smaller lesions; however, for those with extensive resorption associated with perforation the tooth structure is greatly weakened and the prognosis remains poor. 1. Introduction teeth. Unlike the deciduous teeth, the permanent teeth rarely undergo resorption unless stimulated by a pathological Tooth resorption presents itself either as a physiological process. Pathologic resorption occurs following traumatic or a pathological process occurring internally (pulpally injuries, orthodontic tooth movement, or chronic infections derived) or externally (periodontally derived). According to of the pulp or periodontal structures [1]. -

Pulp Canal Obliteration After Traumatic Injuries in Permanent Teeth – Scientific Fact Or Fiction?
CRITICAL REVIEW Endodontic Therapy Pulp canal obliteration after traumatic injuries in permanent teeth – scientific fact or fiction? Juliana Vilela BASTOS(a) Abstract: Pulp canal obliteration (PCO) is a frequent finding associated (b) Maria Ilma de Souza CÔRTES with pulpal revascularization after luxation injuries of young permanent teeth. The underlying mechanisms of PCO are still unclear, (a) Universidade Federal de Minas Gerais - and no experimental scientific evidence is available, except the results UFMG, School of Dentistry, Department of Restorative Dentistry, Belo Horizonte, MG, of a single histopathological study. The lack of sound knowledge Brazil. concerning this process gives rise to controversies, including the (b) Pontifícia Universidade Católica de Minas most suitable denomination. More than a mere semantic question, Gerais – PUC-MG, Department of Dentistry, the denomination is an important issue, because it reflects the nature Belo Horizonte, MG, Brazil. of this process, and directly impacts the treatment plan decision. The hypothesis that accelerated dentin deposition is related to the loss of neural control over odontoblastic secretory activity is well accepted, but demands further supportive studies. PCO is seen radiographically as a rapid narrowing of pulp canal space, whereas common clinical features are yellow crown discoloration and a lower or non-response to sensibility tests. Late development of pulp necrosis and periapical disease are rare complications after PCO, rendering prophylactic endodontic intervention -

Disease of Pulp and Periradicular Tissue: an Overview
Journal of Current Medical Research and Opinion Received 16-09-2020 | Accepted 10-10-2020 | Published Online 11--10-2020 DOI: https://doi.org/10.15520/jcmro.v3i10.351 ISSN (O) 2589-8779 | (P) 2589-8760 CMRO 11 (10), 652−664 (2020) REVIEW ARTICLE Disease of Pulp and Periradicular Tissue: An Overview ∗ Geetanjali Singh1 Sanjana Paul R2 Ayush Arora3 Shakti Kumar4 Lucky Jindal5 Sachin Raina6 1Senior Lecturer, Department of Abstract: Prosthodontics, Crown, Bridge Dental pain is the most common reason due to which patient seek dental and Implantology, Himachal treatment. Pain occur due to diseases involving pulp and periradicular Dental College, Sundernagar, Himachal Pradesh tissues, as these tissues are richly innervated and have ample of blood supply. Also it is enclosed by surrounding tissues that are incapable 2Consultant Endodontist, Kanyakumari, Tamil Nadu of expanding, such as dentin and also has terminal blood flow and small-gauge circulatory access the periapex. All of these characteristics 3Consultant Dental Surgeon, severely constrain the defensive capacity of the pulp tissue when faced Jaipur, Rajasthan with the different aggressions it may be subjected to. In addition to above mentioned characterstics, pulp tissue can also be affected by a 4Consultant Orthodontist, Sirsa, Haryana retrograde infection, arising from the secondary canaliculi, from the periodontal ligament or from the apex during the course of periodontitis. 5Senior Lecturer, Department of Paedodontics and Preventive this review article basically concentrates on structure