Orofacial Pain
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Clinical SHOWCASE Unintentional Replantation: a Technique to Avoid
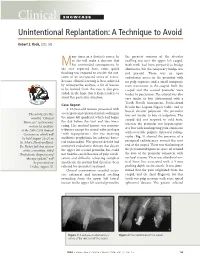
Clinical SHOWCASE Unintentional Replantation: A Technique to Avoid Robert S. Roda, DDS, MS any times in a dentist’s career, he the greatest contour of the alveolar or she will make a decision that swelling was over the upper left cuspid. Mhas unintended consequences. In Both teeth had been prepared as bridge the case reported here, some quick abutments, but the temporary bridge was thinking was required to resolve the out- not present. There was an open come of an unexpected series of events. endodontic access in the premolar with Because clinical learning is best achieved no pulp exposure and a small composite by retrospective analysis, a list of lessons resin restoration in the cuspid. Both the to be learned from this case is also pro- cuspid and the second premolar were vided, in the hope that it helps readers to tender to percussion. The cuspid was also avoid this particular situation. very tender to bite (determined with a Tooth Slooth instrument, Professional Case Report Results Inc, Laguna Niguel, Calif.) and to A 63-year-old woman presented with buccal alveolar palpation. The premolar severe pain and extraoral facial swelling in The articles for this was not tender to bite or palpation. The the upper left quadrant, which had begun month’s “Clinical cuspid did not respond to cold tests, the day before the visit and was wors- Showcase” section were whereas the premolar was hyperrespon- ening. Her medical history was noncon- written by speakers sive but with nonlingering pain consistent at the 2006 CDA Annual tributory except for mitral valve prolapse with reversible pulpitis. -

Oral Diagnosis: the Clinician's Guide
Wright An imprint of Elsevier Science Limited Robert Stevenson House, 1-3 Baxter's Place, Leith Walk, Edinburgh EH I 3AF First published :WOO Reprinted 2002. 238 7X69. fax: (+ 1) 215 238 2239, e-mail: [email protected]. You may also complete your request on-line via the Elsevier Science homepage (http://www.elsevier.com). by selecting'Customer Support' and then 'Obtaining Permissions·. British Library Cataloguing in Publication Data A catalogue record for this book is available from the British Library Library of Congress Cataloging in Publication Data A catalog record for this book is available from the Library of Congress ISBN 0 7236 1040 I _ your source for books. journals and multimedia in the health sciences www.elsevierhealth.com Composition by Scribe Design, Gillingham, Kent Printed and bound in China Contents Preface vii Acknowledgements ix 1 The challenge of diagnosis 1 2 The history 4 3 Examination 11 4 Diagnostic tests 33 5 Pain of dental origin 71 6 Pain of non-dental origin 99 7 Trauma 124 8 Infection 140 9 Cysts 160 10 Ulcers 185 11 White patches 210 12 Bumps, lumps and swellings 226 13 Oral changes in systemic disease 263 14 Oral consequences of medication 290 Index 299 Preface The foundation of any form of successful treatment is accurate diagnosis. Though scientifically based, dentistry is also an art. This is evident in the provision of operative dental care and also in the diagnosis of oral and dental diseases. While diagnostic skills will be developed and enhanced by experience, it is essential that every prospective dentist is taught how to develop a structured and comprehensive approach to oral diagnosis. -

Diagnosis of Cracked Tooth Syndrome
Dental Science - Review Article Diagnosis of cracked tooth syndrome Sebeena Mathew, Boopathi Thangavel, Chalakuzhiyil Abraham Mathew1, SivaKumar Kailasam, Karthick Kumaravadivel, Arjun Das Departments of ABSTRACT Conservative Dentistry The incidences of cracks in teeth seem to have increased during the past decade. Dental practitioners need and Endodontics and to be aware of cracked tooth syndrome (CTS) in order to be successful at diagnosing CTS. Early diagnosis 1Prosthodontics, KSR Institute of Dental Science has been linked with successful restorative management and predictably good prognosis. The purpose of this and Research, KSR Kalvi article is to highlight factors that contribute to detecting cracked teeth. Nagar, Thokkavadi (Po), Tiruchengode, Namakkal (Dt), Tamil Nadu, India Address for correspondence: Dr. Sebeena Mathe, E-mail: matsden@gmail. com Received : 01-12-11 Review completed : 02-01-12 Accepted : 26-01-12 KEY WORDS: Bite test, cracked tooth syndrome, transillumination racked tooth is defined as an incomplete fracture of the patient. Identification can be difficult because the discomfort C dentine in a vital posterior tooth that involves the dentine or pain can mimic that arising from other pathologies, such as and occasionally extends into the pulp. The term “cracked tooth sinusitis, temperomandibular joint disorders, headaches, ear syndrome” (CTS) was first introduced by Cameron in 1964.[1] pain, or atypical orofacial pain. Thus, diagnosis can be time consuming and represents a clinical challenge.[3] Early diagnosis The diagnosis of CTS is often problematic and has been known is paramount as restorative intervention can limit propagation of to challenge even the most experienced dental operators, the fracture, subsequent microleakage, and involvement of the accountable largely by the fact that the associated symptoms pulpal or periodontal tissues, or catastrophic failure of the cusp.[4] tend to be very variable and at times bizarre.[2] The aim of this article is to provide an overview of the diagnosis of CTS. -

Zeroing in on the Cause of Your Patient's Facial Pain
Feras Ghazal, DDS; Mohammed Ahmad, Zeroing in on the cause MD; Hussein Elrawy, DDS; Tamer Said, MD Department of Oral Health of your patient's facial pain (Drs. Ghazal and Elrawy) and Department of Family Medicine/Geriatrics (Drs. Ahmad and Said), The overlapping characteristics of facial pain can make it MetroHealth Medical Center, Cleveland, Ohio difficult to pinpoint the cause. This article, with a handy at-a-glance table, can help. [email protected] The authors reported no potential conflict of interest relevant to this article. acial pain is a common complaint: Up to 22% of adults PracticE in the United States experience orofacial pain during recommendationS F any 6-month period.1 Yet this type of pain can be dif- › Advise patients who have a ficult to diagnose due to the many structures of the face and temporomandibular mouth, pain referral patterns, and insufficient diagnostic tools. disorder that in addition to Specifically, extraoral facial pain can be the result of tem- taking their medication as poromandibular disorders, neuropathic disorders, vascular prescribed, they should limit disorders, or atypical causes, whereas facial pain stemming activities that require moving their jaw, modify their diet, from inside the mouth can have a dental or nondental cause and minimize stress; they (FIGURE). Overlapping characteristics can make it difficult to may require physical therapy distinguish these disorders. To help you to better diagnose and and therapeutic exercises. C manage facial pain, we describe the most common causes and underlying pathological processes. › Consider prescribing a tricyclic antidepressant for patients with persistent idiopathic facial pain. C Extraoral facial pain Extraoral pain refers to the pain that occurs on the face out- 2-15 Strength of recommendation (SoR) side of the oral cavity. -

Pratiqueclinique
Pratique CLINIQUE Sympathetically Maintained Pain Presenting First as Temporomandibular Disorder, then as Parotid Dysfunction Auteur-ressource Subha Giri, BDS, MS; Donald Nixdorf, DDS, MS Dr Nixdorf Courriel : nixdorf@ umn.edu SOMMAIRE Le syndrome douloureux régional complexe (SDRC) est un état chronique qui se carac- térise par une douleur intense, de l’œdème, des rougeurs, une hypersensibilité et des effets sudomoteurs accrus. Dans les 13 cas de SDRC siégeant dans la région de la tête et du cou qui ont été recensés dans la littérature, il a été établi que l’étiologie de la douleur était une lésion nerveuse. Dans cet article, nous présentons le cas d’une femme de 30 ans souffrant de douleur maintenue par le système sympathique, sans lésion nerveuse appa- rente. Ses principaux symptômes – douleur préauriculaire gauche et incapacité d’ouvrir grand la bouche – simulaient une arthralgie temporomandibulaire et une douleur myo- faciale des muscles masticateurs. Puis sont apparus une douleur préauriculaire intermit- tente et de l’œdème accompagnés d’hyposalivation – des signes cette fois-ci évocateurs d’une parotidite. Après une évaluation diagnostique exhaustive, aucune pathologie sous-jacente précise n’a pu être déterminée et un diagnostic de douleur névropathique à forte composante sympathique a été posé. Deux ans après l’apparition des symptômes et le début des soins, un traitement combinant des blocs répétés du ganglion cervico- thoracique et une pharmacothérapie (clonidine en perfusion entérale) a procuré un sou- lagement adéquat de la douleur. Mots clés MeSH : complex regional pain syndrome; pain, intractable; parotitis; temporomandibular joint disorders Pour les citations, la version définitive de cet article est la version électronique : www.cda-adc.ca/jcda/vol-73/issue-2/163.html omplex regional pain syndrome (CRPS) • onset following an initiating noxious is a chronic condition that usually affects event (CRPS-type I) or nerve injury (CRPS- Cextremities, such as the arms or legs. -

Cracked Tooth Syndrome, an Update
International Journal of Applied Dental Sciences 2021; 7(2): 314-317 ISSN Print: 2394-7489 ISSN Online: 2394-7497 IJADS 2021; 7(2): 314-317 Cracked tooth syndrome, an update © 2021 IJADS www.oraljournal.com Received: 19-02-2021 Dariela Isabel Gonzalez-Guajardo, Guadalupe Magdalena Ramirez- Accepted: 21-03-2021 Herrera, Alejandro Mas-Enriquez, Guadalupe Rosalia Capetillo- Dariela Isabel Gonzalez-Guajardo Hernandez, Leticia Tiburcio-Morteo, Claudio Cabral-Romero, Rene Master in Sciences Student, Hernandez-Delgadillo and Juan Manuel Solis-Soto Universidad Autonoma de Nuevo Leon, Facultad de Odontologia, Monterrey, Nuevo Leon, CP 64460, DOI: https://doi.org/10.22271/oral.2021.v7.i2e.1226 Mexico Guadalupe Magdalena Ramirez- Abstract Herrera Introduction: Cracked tooth syndrome is defined as an incomplete fracture initiated from the crown and Professor, Universidad Autonoma de extending cervically, and sometimes gingivally, and is usually directed mesiodistally. Objective: To Nuevo Leon, Facultad de analyze the literature about cracked tooth syndrome, its etiology, prevalence, pulp involvement and Odontologia, Monterrey, Nuevo Leon, CP 64460, Mexico treatment. Methodology: Using the keywords “cracked tooth syndrome”, “etiology”, “prevalence”, “pulp Alejandro Mas-Enriquez involvement” and “treatment”, the MEDLINE/PubMed and ScienceDirect databases were searched, with Associate Professor, Universidad emphasis on the last 5 years. It was evaluated with the PRISMA and AMSTAR-2 guidelines. Autonoma de Nuevo Leon, Facultad de Odontologia, Monterrey, Nuevo Results: There are many causes for cracks, the main one being malocclusion. Another is due to Leon, CP 64460, Mexico restorations, pieces to which amalgam was placed due to the extension of the cavity for the retentions. The second lower molar presents more frequently fissures due to premature contact. -

Chronic Orofacial Pain: Burning Mouth Syndrome and Other Neuropathic
anagem n M e ai n t P & f o M l e Journal of a d n i c r i u n o e J Pain Management & Medicine Tait et al., J Pain Manage Med 2017, 3:1 Review Article Open Access Chronic Orofacial Pain: Burning Mouth Syndrome and Other Neuropathic Disorders Raymond C Tait1, McKenzie Ferguson2 and Christopher M Herndon2 1Saint Louis University School of Medicine, St. Louis, USA 2Southern Illinois University Edwardsville School of Pharmacy, Edwardsville, USA *Corresponding author: RC Tait, Department of Psychiatry, Saint Louis University School of Medicine,1438 SouthGrand, Boulevard, St Louis, MO-63104, USA, Tel: 3149774817; Fax: 3149774879; E-mail: [email protected] Recevied date: October 4, 2016; Accepted date: January 17, 2017, Published date: January 30, 2017 Copyright: © 2017 Raymond C Tait, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Abstract Chronic orofacial pain is a symptom associated with a wide range of neuropathic, neurovascular, idiopathic, and myofascial conditions that affect a significant proportion of the population. While the collective impact of the subset of the orofacial pain disorders involving neurogenic and idiopathic mechanisms is substantial, some of these are relatively uncommon. Hence, patients with these disorders can be vulnerable to misdiagnosis, sometimes for years, increasing the symptom burden and delaying effective treatment. This manuscript first reviews the decision tree to be followed in diagnosing any neuropathic pain condition, as well as the levels of evidence needed to make a diagnosis with each of several levels of confidence: definite, probable, or possible. -

Acute Dental Pain I: Pulpal and Dentinal Pain Pulpal And
VIDENSKAB & KLINIK | Oversigtsartikel ABSTRACT Acute dental pain I: Acute dental pain I: pulpal and dentinal pain pulpal and The specialized anatomy of the pulp-dentin dentinal pain complex and the dense, predominantly noci- ceptive pulpal innervation from the trigeminal nerve explains the variety of pain sensations from this organ. Matti Närhi, professor, ph.d., Department of Dentistry/Physiology, Institute of Medicine, University of Eastern Finland, Finland Brief, sharp pain is typical of A-fibre-mediated pain, while long-lasting, dull/aching pain indi- Lars Bjørndal, associate professor, dr.odont., ph.d., Department of Cariology and Endodontics, Faculty of Health and Medical Sciences, cates C-fibre involvement. A-fibres react to University of Copenhagen cold or mechanical stimuli, such as cold drinks Maria Pigg, senior lecturer, dr.odont., Department of Endodontics or toothbrushing, whereas C-fibres are mainly and Department of Orofacial Pain and Jaw Function, Malmö activated by inflammatory mediators. Thus, lin- University, Sweden gering pain suggests presence of irreversible Inge Fristad, professor, ph.d., Department of Clinical Dentistry, pulpal inflammation. Faculty of Medicine and Dentistry,University of Bergen, Norway During pulpitis, structural changes of the pul- Sivakami Rethnam Haug, associate professor and head, dr.odont., pal nerves (sprouting) occur and neuropeptide Section for Endodontics, Department of Clinical Dentistry, Faculty of release triggers an immune response; neuro- Medicine and Dentistry, University of Bergen, Norway, Årstadveien 19 N5009, Bergen, Norway genic inflammation. Pain sensations during pul- pitis can range from hypersensitivity to thermal stimuli to severe throbbing. There might also be aching pain, possibly referred and often difficult to localize. Thus, diagnosis is challenging for ain localized to teeth is among the most frequently ex- the clinician. -

Diagnosis and Treatment of Temporomandibular Disorders ROBERT L
Diagnosis and Treatment of Temporomandibular Disorders ROBERT L. GAUER, MD, and MICHAEL J. SEMIDEY, DMD, Womack Army Medical Center, Fort Bragg, North Carolina Temporomandibular disorders (TMD) are a heterogeneous group of musculoskeletal and neuromuscular conditions involving the temporomandibular joint complex, and surrounding musculature and osseous components. TMD affects up to 15% of adults, with a peak incidence at 20 to 40 years of age. TMD is classified asintra-articular or extra- articular. Common symptoms include jaw pain or dysfunction, earache, headache, and facial pain. The etiology of TMD is multifactorial and includes biologic, environmental, social, emotional, and cognitive triggers. Diagnosis is most often based on history and physical examination. Diagnostic imaging may be beneficial when malocclusion or intra-articular abnormalities are suspected. Most patients improve with a combination of noninvasive therapies, including patient education, self-care, cognitive behavior therapy, pharmacotherapy, physical therapy, and occlusal devices. Nonsteroidal anti-inflammatory drugs and muscle relaxants are recommended initially, and benzodiazepines or antidepressants may be added for chronic cases. Referral to an oral and maxillofacial surgeon is indicated for refrac- tory cases. (Am Fam Physician. 2015;91(6):378-386. Copyright © 2015 American Academy of Family Physicians.) More online he temporomandibular joint (TMJ) emotional, and cognitive triggers. Factors at http://www. is formed by the mandibular con- consistently associated with TMD include aafp.org/afp. dyle inserting into the mandibular other pain conditions (e.g., chronic head- CME This clinical content fossa of the temporal bone. Muscles aches), fibromyalgia, autoimmune disor- conforms to AAFP criteria Tof mastication are primarily responsible for ders, sleep apnea, and psychiatric illness.1,3 for continuing medical education (CME). -

Pulp Canal Obliteration After Traumatic Injuries in Permanent Teeth – Scientific Fact Or Fiction?
CRITICAL REVIEW Endodontic Therapy Pulp canal obliteration after traumatic injuries in permanent teeth – scientific fact or fiction? Juliana Vilela BASTOS(a) Abstract: Pulp canal obliteration (PCO) is a frequent finding associated (b) Maria Ilma de Souza CÔRTES with pulpal revascularization after luxation injuries of young permanent teeth. The underlying mechanisms of PCO are still unclear, (a) Universidade Federal de Minas Gerais - and no experimental scientific evidence is available, except the results UFMG, School of Dentistry, Department of Restorative Dentistry, Belo Horizonte, MG, of a single histopathological study. The lack of sound knowledge Brazil. concerning this process gives rise to controversies, including the (b) Pontifícia Universidade Católica de Minas most suitable denomination. More than a mere semantic question, Gerais – PUC-MG, Department of Dentistry, the denomination is an important issue, because it reflects the nature Belo Horizonte, MG, Brazil. of this process, and directly impacts the treatment plan decision. The hypothesis that accelerated dentin deposition is related to the loss of neural control over odontoblastic secretory activity is well accepted, but demands further supportive studies. PCO is seen radiographically as a rapid narrowing of pulp canal space, whereas common clinical features are yellow crown discoloration and a lower or non-response to sensibility tests. Late development of pulp necrosis and periapical disease are rare complications after PCO, rendering prophylactic endodontic intervention -

Disease of Pulp and Periradicular Tissue: an Overview
Journal of Current Medical Research and Opinion Received 16-09-2020 | Accepted 10-10-2020 | Published Online 11--10-2020 DOI: https://doi.org/10.15520/jcmro.v3i10.351 ISSN (O) 2589-8779 | (P) 2589-8760 CMRO 11 (10), 652−664 (2020) REVIEW ARTICLE Disease of Pulp and Periradicular Tissue: An Overview ∗ Geetanjali Singh1 Sanjana Paul R2 Ayush Arora3 Shakti Kumar4 Lucky Jindal5 Sachin Raina6 1Senior Lecturer, Department of Abstract: Prosthodontics, Crown, Bridge Dental pain is the most common reason due to which patient seek dental and Implantology, Himachal treatment. Pain occur due to diseases involving pulp and periradicular Dental College, Sundernagar, Himachal Pradesh tissues, as these tissues are richly innervated and have ample of blood supply. Also it is enclosed by surrounding tissues that are incapable 2Consultant Endodontist, Kanyakumari, Tamil Nadu of expanding, such as dentin and also has terminal blood flow and small-gauge circulatory access the periapex. All of these characteristics 3Consultant Dental Surgeon, severely constrain the defensive capacity of the pulp tissue when faced Jaipur, Rajasthan with the different aggressions it may be subjected to. In addition to above mentioned characterstics, pulp tissue can also be affected by a 4Consultant Orthodontist, Sirsa, Haryana retrograde infection, arising from the secondary canaliculi, from the periodontal ligament or from the apex during the course of periodontitis. 5Senior Lecturer, Department of Paedodontics and Preventive this review article basically concentrates on structure -

Quality Resource Guide Diagnosing and Managing the Cracked Tooth Part 1: Crown-Originating Fractures
MetLife designates this activity for 1.5 continuing education credit for the review of this Quality Resource Guide Quality Resource Guide and successful completion of the post test. Diagnosing and Managing the Cracked Tooth Part 1: Crown-Originating Fractures FIRST EDITION Educational Objectives Following this unit of instruction, the practitioner should be able to: Author Acknowledgements Leif K. Bakland, DDS 1. Describe the three categories of dental fractures. Emeritus Professor 2. Recognize the usual symptoms of crown-originating fractures. Tory Silvestrin, DDS 3. Recognize the role of radiography in diagnosis of crown-originating fractures. Assistant Professor Loma Linda University, School of Dentistry 4. Describe the clinical tests used for identifying teeth with crown-originating fractures. Loma Linda, California 5. Describe treatment options for crown-originating fractures. Drs. Bakland and Silvestrin have no relevant relationships to disclose. 6. Develop a prognosis for a crown-originating fracture. The following commentary highlights fundamental and commonly accepted practices on the subject matter. The information is Introduction intended as a general overview and is for The term ‘cracked tooth’ has been used to describe Table 1 educational purposes only. This information many types of fractures and cracks in teeth. Other terms Terms Used For Dental Fractures does not constitute legal advice, which can only be provided by an attorney. have also been used (Table 1) for this dental problem, Cracked tooth © Metropolitan Life Insurance Company, indicating that dentistry has not previously been able to Cracked tooth syndrome New York, NY. All materials subject to develop a generally accepted categorization scheme. Green stick fracture this copyright may be photocopied for the 1 noncommercial purpose of scientific or Efforts have been made over the years.