High Carriers Frequency of an Apparently Ancient Founder
Total Page:16
File Type:pdf, Size:1020Kb

Load more
Recommended publications
-

Elio™ Plasma Complete
™ elio plasma complete About PGDx elioTM plasma complete PGDx elio™ plasma complete is an end-to-end kitted liquid biopsy solution that analyzes circulating tumor DNA for genetic alterations in cancer, eliminating the need for an invasive biopsy or tumor tissue. Designed to be used across the globe on the PGDx elio™ testing platform, PGDx elio plasma complete also includes automated bioinformatics ensuring consistent, high-quality results. What does PGDx elioTM mean? Assay Specifications Empowering Local PARAMETER DETAILS Insight for Oncology Panel Size 2.1MB 521 genes for SNV & Indels 38 genes for amplifications 21 genes for translocations Panel Content and Variant Type bMSI bTMB (Muts/Mb) LOH status Sample requirement plasma ctDNA DNA input requirement 25ng recommended, 10ng minimum End-to-end Kitted 521 Genes From a Single Solution Sample Pass Rate 97.4% overall pass rate (227/233) Sample Sequencing platform/flowcell NovaSeq 6000/S2 flow cell Sequence run 2 x 150 bp Cases per sequencing run 16 (no external control required) Turn-key Developed Under Workflow Manual and Automated Available Bioinformatics Design Control Pipeline Average total coverage ~20,000x Performance Specifications PRODUCT FEATURES Variant Reportable Analytical Analytical Range Sensitivity Specificity (LOD95) Actionable • Plasma analysis for pan-cancer solid ≥ 0.1% VAF 0.40% VAF 100% SNVs/Indels tumor biomarker testing and discovery • 500+ gene kitted assay developed under Non-actionable ≥ 0.5% VAF 1.16% VAF 99.9% Design Control SNVs/Indels • Comprehensive coverage of biomarkers, All clinically relevant targets, cancer ≥ 3 fusion reads 0.33% VAF 100% Translocations signaling pathways and DNA damage repair pathways All ≥ 1.15-fold 1.32-fold 100% • Large panel size supports TMB and LOH Amplifications For Research Use Only. -

Large XPF-Dependent Deletions Following Misrepair of a DNA Double Strand Break Are Prevented by the RNA:DNA Helicase Senataxin
www.nature.com/scientificreports OPEN Large XPF-dependent deletions following misrepair of a DNA double strand break are prevented Received: 26 October 2017 Accepted: 9 February 2018 by the RNA:DNA helicase Published: xx xx xxxx Senataxin Julien Brustel1, Zuzanna Kozik1, Natalia Gromak2, Velibor Savic3,4 & Steve M. M. Sweet1,5 Deletions and chromosome re-arrangements are common features of cancer cells. We have established a new two-component system reporting on epigenetic silencing or deletion of an actively transcribed gene adjacent to a double-strand break (DSB). Unexpectedly, we fnd that a targeted DSB results in a minority (<10%) misrepair event of kilobase deletions encompassing the DSB site and transcribed gene. Deletions are reduced upon RNaseH1 over-expression and increased after knockdown of the DNA:RNA helicase Senataxin, implicating a role for DNA:RNA hybrids. We further demonstrate that the majority of these large deletions are dependent on the 3′ fap endonuclease XPF. DNA:RNA hybrids were detected by DNA:RNA immunoprecipitation in our system after DSB generation. These hybrids were reduced by RNaseH1 over-expression and increased by Senataxin knock-down, consistent with a role in deletions. Overall, these data are consistent with DNA:RNA hybrid generation at the site of a DSB, mis-processing of which results in genome instability in the form of large deletions. DNA is the target of numerous genotoxic attacks that result in diferent types of damage. DNA double-strand breaks (DSBs) occur at low frequency, compared with single-strand breaks and other forms of DNA damage1, however DSBs pose the risk of translocations and deletions and their repair is therefore essential to cell integrity. -

MECHANISMS in ENDOCRINOLOGY: Novel Genetic Causes of Short Stature
J M Wit and others Genetics of short stature 174:4 R145–R173 Review MECHANISMS IN ENDOCRINOLOGY Novel genetic causes of short stature 1 1 2 2 Jan M Wit , Wilma Oostdijk , Monique Losekoot , Hermine A van Duyvenvoorde , Correspondence Claudia A L Ruivenkamp2 and Sarina G Kant2 should be addressed to J M Wit Departments of 1Paediatrics and 2Clinical Genetics, Leiden University Medical Center, PO Box 9600, 2300 RC Leiden, Email The Netherlands [email protected] Abstract The fast technological development, particularly single nucleotide polymorphism array, array-comparative genomic hybridization, and whole exome sequencing, has led to the discovery of many novel genetic causes of growth failure. In this review we discuss a selection of these, according to a diagnostic classification centred on the epiphyseal growth plate. We successively discuss disorders in hormone signalling, paracrine factors, matrix molecules, intracellular pathways, and fundamental cellular processes, followed by chromosomal aberrations including copy number variants (CNVs) and imprinting disorders associated with short stature. Many novel causes of GH deficiency (GHD) as part of combined pituitary hormone deficiency have been uncovered. The most frequent genetic causes of isolated GHD are GH1 and GHRHR defects, but several novel causes have recently been found, such as GHSR, RNPC3, and IFT172 mutations. Besides well-defined causes of GH insensitivity (GHR, STAT5B, IGFALS, IGF1 defects), disorders of NFkB signalling, STAT3 and IGF2 have recently been discovered. Heterozygous IGF1R defects are a relatively frequent cause of prenatal and postnatal growth retardation. TRHA mutations cause a syndromic form of short stature with elevated T3/T4 ratio. Disorders of signalling of various paracrine factors (FGFs, BMPs, WNTs, PTHrP/IHH, and CNP/NPR2) or genetic defects affecting cartilage extracellular matrix usually cause disproportionate short stature. -
Neurodegeneration in Accelerated Aging
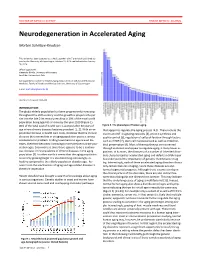
DOCTOR OF MEDICAL SCIENCE DANISH MEDICAL JOURNAL Neurodegeneration in Accelerated Aging Morten Scheibye-Knudsen This review has been accepted as a thesis together with 7 previously published pa- pers by the University of Copenhagen, October 16, 2014 and defended on January 14, 2016 Official opponents: Alexander Bürkle, University of Konstanz Lars Eide, University of Oslo Correspondence: Center for Healthy Aging, Department of Cellular and Molecular Medicine, Faculty of Health and Medical Sciences, University of Copenhagen E-mail: [email protected] Dan Med J 2016;63(11):B5308 INTRODUCTION The global elderly population has been progressively increasing throughout the 20th century and this growth is projected to per- sist into the late 21st century resulting in 20% of the total world population being aged 65 or more by the year 2100 (Figure 1). 80% of the total cost of health care is accrued after 40 years of Figure 2. The phenotype of human aging. age where chronic diseases become prevalent [1, 2]. With an ex- that appear to regulate the aging process [4,5]. These include the ponential increase in health care costs, it follows that the chronic insulin and IGF-1 signaling cascades [4], protein synthesis and diseases that accumulate in an aging population poses a serious quality control [6], regulation of cell proliferation through factors socioeconomic problem. Finding treatments to age related dis- such as mTOR [7], stem cell maintenance 8 as well as mitochon- eases, therefore becomes increasingly more pertinent as the pop- drial preservation [9]. Most of these pathways are conserved ulation ages. Even more so since there appears to be a continu- through evolution and appear to regulate aging in many lower or- ous increase in the prevalence of chronic diseases in the aging ganisms. -

Regulation of the Intranuclear Distribution of the Cockayne Syndrome Proteins Received: 26 July 2017 Teruaki Iyama, Mustafa N
www.nature.com/scientificreports OPEN Regulation of the Intranuclear Distribution of the Cockayne Syndrome Proteins Received: 26 July 2017 Teruaki Iyama, Mustafa N. Okur, Tyler Golato, Daniel R. McNeill, Huiming Lu , Accepted: 1 November 2018 Royce Hamilton, Aishwarya Raja, Vilhelm A. Bohr & David M. Wilson III Published: xx xx xxxx Cockayne syndrome (CS) is an inherited disorder that involves photosensitivity, developmental defects, progressive degeneration and characteristics of premature aging. Evidence indicates primarily nuclear roles for the major CS proteins, CSA and CSB, specifcally in DNA repair and RNA transcription. We reveal herein a complex regulation of CSB targeting that involves three major consensus signals: NLS1 (aa467-481), which directs nuclear and nucleolar localization in cooperation with NoLS1 (aa302-341), and NLS2 (aa1038-1055), which seemingly optimizes nuclear enrichment. CSB localization to the nucleolus was also found to be important for full UVC resistance. CSA, which does not contain any obvious targeting sequences, was adversely afected (i.e. presumably destabilized) by any form of truncation. No inter-coordination between the subnuclear localization of CSA and CSB was observed, implying that this aspect does not underlie the clinical features of CS. The E3 ubiquitin ligase binding partner of CSA, DDB1, played an important role in CSA stability (as well as DDB2), and facilitated CSA association with chromatin following UV irradiation; yet did not afect CSB chromatin binding. We also observed that initial recruitment of CSB to DNA interstrand crosslinks is similar in the nucleoplasm and nucleolus, although fnal accumulation is greater in the former. Whereas assembly of CSB at sites of DNA damage in the nucleolus was not afected by RNA polymerase I inhibition, stable retention at these sites of presumed repair was abrogated. -

Haplotype Patterns in Cancer-Related Genes with Long-Range Linkage Disequilibrium: No Evidence of Association with Breast Cancer Or Positive Selection
European Journal of Human Genetics (2008) 16, 252–260 & 2008 Nature Publishing Group All rights reserved 1018-4813/08 $30.00 www.nature.com/ejhg ARTICLE Haplotype patterns in cancer-related genes with long-range linkage disequilibrium: no evidence of association with breast cancer or positive selection Gloria Ribas*,1, Roger L Milne2, Anna Gonzalez-Neira2 and Javier Benı´tez1,2 1Human Genetics Group, Human Cancer Genetics Programme, Spanish National Cancer Centre (CNIO), Madrid, Spain; 2National Genotyping Centre (CeGen), Human Cancer Genetics Programme, Spanish National Cancer Centre (CNIO), Madrid, Spain The average length of linkage disequilibrium (LD) blocks in European populations is about 22 kb. In this study, we have selected 20 genes with LD blocks larger than 60 kb (with a median length of 88 kb) from a total of 121 cancer-related genes. We observed limited haplotype diversity, with an average of three haplotypes per gene accounting for more than 90% of the diversity, two of these being a Yin–Yang pair in 95% of the LD blocks. The mean frequency of the most common haplotype in the Spanish population was just below 50%, similar to those for the HapMap CEU and African samples, but lower than the 60% observed in Asian samples. Genes involved in the regulation of nucleobases and nucleic acid metabolism were overrepresented among these 20 genes with long LD blocks (eight genes ATM, BRCA1, BRCA2, ERCC6, MLH1, MSH3, RAD54B and XRCC4) relative to the other 101 cancer-related genes studied (P ¼ 1.23 Â 10À6). The ancestral haplotype was observed at a frequency greater than 3 in 67% of the genes either in the Spanish or one of the HapMap sampled populations. -

Understanding Nucleotide Excision Repair and Its Roles in Cancer and Ageing
REVIEWS DNA DAMAGE Understanding nucleotide excision repair and its roles in cancer and ageing Jurgen A. Marteijn*, Hannes Lans*, Wim Vermeulen, Jan H. J. Hoeijmakers Abstract | Nucleotide excision repair (NER) eliminates various structurally unrelated DNA lesions by a multiwise ‘cut and patch’-type reaction. The global genome NER (GG‑NER) subpathway prevents mutagenesis by probing the genome for helix-distorting lesions, whereas transcription-coupled NER (TC‑NER) removes transcription-blocking lesions to permit unperturbed gene expression, thereby preventing cell death. Consequently, defects in GG‑NER result in cancer predisposition, whereas defects in TC‑NER cause a variety of diseases ranging from ultraviolet radiation‑sensitive syndrome to severe premature ageing conditions such as Cockayne syndrome. Recent studies have uncovered new aspects of DNA-damage detection by NER, how NER is regulated by extensive post-translational modifications, and the dynamic chromatin interactions that control its efficiency. Based on these findings, a mechanistic model is proposed that explains the complex genotype–phenotype correlations of transcription-coupled repair disorders. The integrity of DNA is constantly threatened by endo of an intricate DNA-damage response (DDR), which genously formed metabolic products and by-products, comprises sophisticated repair and damage signalling such as reactive oxygen species (ROS) and alkylating processes. The DDR involves DNA-damage sensors and agents, and by its intrinsic chemical instability (for exam signalling kinases that regulate a range of downstream ple, by its ability to spontaneously undergo hydrolytic mediator and effector molecules that control repair, cell deamination and depurination). Environmental chemi cycle progression and cell fate4. The core of this DDR is cals and radiation also affect the physical constitution of formed by a network of complementary DNA repair sys DNA1. -

Nucleotide Excision Repair Gene Expression After Cisplatin Treatment in Melanoma
Published OnlineFirst August 31, 2010; DOI: 10.1158/0008-5472.CAN-10-0161 Molecular and Cellular Pathobiology Cancer Research Nucleotide Excision Repair Gene Expression after Cisplatin Treatment in Melanoma Nikola A. Bowden1,2,3, Katie A. Ashton1,2,3, Kelly A. Avery-Kiejda4, Xu Dong Zhang4, Peter Hersey4, and Rodney J. Scott1,2,3,5 Abstract Two of the hallmark features of melanoma are its development as a result of chronic UV radiation exposure and the limited efficacy of cisplatin in the disease treatment. Both of these DNA-damaging agents result in large helix-distorting DNA damage that is recognized and repaired by nucleotide excision repair (NER). The aim of this study was to examine the expression of NER gene transcripts, p53, and p21 in melanoma cell lines treated with cisplatin compared with melanocytes. Basal expression of all genes was greater in the melanoma cell lines compared with melanocytes. Global genome repair (GGR) transcripts showed significantly decreased relative expression (RE) in melanoma cell lines 24 hours after cisplatin treatment. The basal RE of p53 was significantly higher in the melanoma cell lines compared with the melanocytes. However, induction of p53 was only significant in the melanocytes at 6 and 24 hours after cisplatin treatment. Inhibition of p53 expression significantly decreased the expression of all the GGR transcripts in melanocytes at 6 and 24 hours after cis- platin treatment. Although the RE levels were lower with p53 inhibition, the induction of the GGR genes was very similar to that in the control melanocytes and increased significantly across the time points. The findings from this study revealed reduced GGR transcript levels in melanoma cells 24 hours after cisplatin treatment. -

Can Synthetic Lethality Approach Be Used with DNA Repair Genes for Primary and Secondary MDS?
Medical Oncology (2019) 36:99 https://doi.org/10.1007/s12032-019-1324-7 ORIGINAL PAPER Can synthetic lethality approach be used with DNA repair genes for primary and secondary MDS? Howard Lopes Ribeiro Junior1,2 · Roberta Taiane Germano de Oliveira1,2 · Daniela de Paula Borges1,2 · Marília Braga Costa1,2 · Izabelle Rocha Farias1,2 · Antônio Wesley Araújo dos Santos1,2 · Silvia Maria Meira Magalhães1,2 · Ronald Feitosa Pinheiro1,2,3 Received: 5 August 2019 / Accepted: 15 October 2019 / Published online: 30 October 2019 © Springer Science+Business Media, LLC, part of Springer Nature 2019 Abstract Cancer-specifc defects in DNA repair pathways create the opportunity to employ synthetic lethality approach. Recently, GEMA (gene expression and mutation analysis) approach detected insufcient expression of BRCA or NHEJ (non-homol- ogous end joining) to predict PARP inhibitors response. We evaluated a possible role of DNA repair pathways using gene expression of single-strand break (XPA, XPC, XPG/ERCC5, CSA/ERCC8, and CSB/ERCC6) and double-strand break (ATM, BRCA1, BRCA2, RAD51, XRCC5, XRCC6, LIG4) in 92 patients with myelodysplastic syndrome (73 de novo, 9 therapy- related (t-MDS). Therapy-related MDS (t-MDS) demonstrated a signifcant downregulation of axis BRCA1-BRCA2-RAD51 comparing to normal controls (p = 0.048, p = 0.001, p = 0.001). XRCC6 showed signifcantly low expression in de novo MDS comparing to controls (p = 0.039) and for patients who presented chromosomal abnormalities (p = 0.047). Downregula- tion of LIG4 was consistently associated with poor prognostic markers in de novo MDS (hemoglobin < 8 g/dL (p = 0.040), neutrophils < 800/mm3 (p < 0.001), patients with excess of blasts (p = 0.001), very high (p = 0.002)/high IPSS-R (p = 0.043) and AML transformation (p < 0.001). -
University of Cincinnati
UNIVERSITY OF CINCINNATI _____________ , 20 _____ I,______________________________________________, hereby submit this as part of the requirements for the degree of: ________________________________________________ in: ________________________________________________ It is entitled: ________________________________________________ ________________________________________________ ________________________________________________ ________________________________________________ Approved by: ________________________ ________________________ ________________________ ________________________ ________________________ BLM is a Suppressor of DNA Recombination A dissertation submitted to the Division of Research and Advanced Studies Of the University of Cincinnati In partial fulfillment of the Requirements for the degree of Doctorate of Philosophy (Ph.D.) In the Department of Molecular Genetics, Microbiology, and Biochemistry Of the College of Arts and Sciences 2002 by Joel E. Straughen B.S., The Ohio State University, 1985 M.D., University of Cincinnati, 2002 Committee Chair: Joanna Groden, Ph.D. i ABSTRACT Bloom’s syndrome (BS) is a rare, recessive chromosome breakage disorder characterized by small stature, sun sensitivity, facial erythema, immunodeficiency, female subfertility, male infertility, and a predisposition to a variety of cancers. When this body of work was started, the gene for Bloom’s syndrome (BLM)hadyettobe identified. This work presents characterization of the genomic region at BLM and the identification of BLM. With the cloning -

Somatic Mutations in Early Onset Luminal Breast Cancer
www.oncotarget.com Oncotarget, 2018, Vol. 9, (No. 32), pp: 22460-22479 Research Paper Somatic mutations in early onset luminal breast cancer Giselly Encinas1,*, Veronica Y. Sabelnykova2,*, Eduardo Carneiro de Lyra3, Maria Lucia Hirata Katayama1, Simone Maistro1, Pedro Wilson Mompean de Vasconcellos Valle1, Gláucia Fernanda de Lima Pereira1, Lívia Munhoz Rodrigues1, Pedro Adolpho de Menezes Pacheco Serio1, Ana Carolina Ribeiro Chaves de Gouvêa1, Felipe Correa Geyer1, Ricardo Alves Basso3, Fátima Solange Pasini1, Maria del Pilar Esteves Diz1, Maria Mitzi Brentani1, João Carlos Guedes Sampaio Góes3, Roger Chammas1, Paul C. Boutros2,4,5 and Maria Aparecida Azevedo Koike Folgueira1 1Instituto do Cancer do Estado de Sao Paulo, Departamento de Radiologia e Oncologia, Faculdade de Medicina FMUSP, Universidade de Sao Paulo, Sao Paulo, SP, Brazil 2Ontario Institute for Cancer Research, Toronto, Canada 3Instituto Brasileiro de Controle do Câncer, São Paulo, Brazil 4Department of Medical Biophysics, University of Toronto, Toronto, Canada 5Department of Pharmacology and Toxicology, University of Toronto, Toronto, Canada *These authors have contributed equally to this work Correspondence to: Maria Aparecida Azevedo Koike Folgueira, email: [email protected] Keywords: breast cancer; young patients; somatic mutation; germline mutation; luminal subtype Received: September 26, 2017 Accepted: March 06, 2018 Published: April 27, 2018 Copyright: Encinas et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License 3.0 (CC BY 3.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. ABSTRACT Breast cancer arising in very young patients may be biologically distinct; however, these tumors have been less well studied. -

Messenger RNA Levels of XPAC and ERCC1 in Ovarian Cancer Tissue Correlate with Response to Platinum-Based Chemotherapy
Messenger RNA levels of XPAC and ERCC1 in ovarian cancer tissue correlate with response to platinum-based chemotherapy. M Dabholkar, … , J J Yu, E Reed J Clin Invest. 1994;94(2):703-708. https://doi.org/10.1172/JCI117388. Research Article Nucleotide excision repair is a DNA repair pathway that is highly conserved in nature, with analogous repair systems described in Escherichia coli, yeast, and mammalian cells. The rate-limiting step, DNA damage recognition and excision, is effected by the protein products of the genes ERCC1 and XPAC. We therefore assessed mRNA levels of ERCC1 and XPAC in malignant ovarian cancer tissues from 28 patients that were harvested before the administration of platinum- based chemotherapy. Cancer tissues from patients whose tumors were clinically resistant to therapy (n = 13) showed greater levels of total ERCC1 mRNA (P = 0.059), full length transcript of ERCC1 mRNA (P = 0.026), and XPAC mRNA (P = 0.011), as compared with tumor tissues from those individuals clinically sensitive to therapy (n = 15). In 19 of these tissues, the percentage of alternative splicing of ERCC1 mRNA was assessed. ERCC1 splicing was highly variable, with no difference observed between responders and nonresponders. The alternatively spliced species constituted 2-58% of the total ERCC1 mRNA in responders (median = 18%) and 4-71% in nonresponders (median = 13%). These data suggest greater activity of the DNA excision repair genes ERCC1 and XPAC in ovarian cancer tissues of patients clinically resistant to platinum compounds. These data also