Swedish Seattle Community Health Needs Assessment First Hill Campus and Cherry Hill Campus 2016- 2018
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Changes to Premera's Heritage Prime Network Affects WEA Select Health
Changes to Premera’s Heritage Prime Network affects WEA Select Health Plans On Nov. 1, 2016, the WEA Select EasyChoice Plan B will change from the Premera Heritage network to the Heritage Prime network. Heritage Prime includes major medical facilities and providers across Washington that work closely with Premera to manage healthcare costs and quality. To help ensure Heritage Prime continues to offer the best combination of choice and value, there will be a change starting in the New Year. This will affect WEA Select EasyChoice B and Basic Plans. Some doctors, hospitals, and clinics in the Swedish, Providence, and CHI Franciscan Health systems will no longer be in- network for Heritage Prime as of January 1, 2017. Some will remain in-network in areas where there are few or no other options to get medical care. (Please see the list on the back page.) With Heritage Prime, Premera strives to keep health plans affordable while giving access to quality care High-quality Care — The medical professionals in Heritage Prime share Premera’s commitment to the highest levels of quality, safety, and enrollee experience. Cost-effective Care — The doctors and hospitals in Heritage Prime have contracts with Premera to keep the total cost of care as low as possible. Choice — Some of the major medical systems in Heritage Prime include: • EvergreenHealth Medical Center • The Everett Clinic • Overlake Hospital Medical Center • Deaconess Hospital (Rockwood • MultiCare Health System • UW Medicine Health System) • Northwest Physicians Network • Virginia Mason Remember, if you choose a doctor or hospital in the network, your out-of-pocket costs will be lower. -

WSHA Member Hospitals
WSHA Member Hospitals www.wsha.org WHATCOM BELLINGHAM REPUBLIC TONASKET Ferry County Memorial Hospital SAN JUAN PeaceHealth St. Joseph Medical Center OKANOGAN North Valley Hospital STEVENS SEDRO-WOOLLEY PEND SKAGIT PeaceHealth United General Medical Center OMAK OREILLE FRIDAY HARBOR MT. VERNON Mid-Valley Hospital F ERRY COLVILLE PeaceHealth Peace ANACORTES Skagit Valley Hospital Providence Mount Carmel Hospital Island Medical Center Island Hospital CHEWELAH ISLAND Providence St. Joseph’s Hospital COUPEVILLE ARLINGTON WhidbeyHealth Cascade Valley Hospital & Clinics BREWSTER MARYSVILLE Three Rivers Hospital NEWPORT Newport Hospital & Health Services CLALLAM PORT ANGELES Smokey Point Behavioral Health Olympic Medical Center PORT TOWNSEND EVERETT SNOHOMISH CHELAN FORKS Jefferson Healthcare Providence Regional Medical Center Everett SPOKANE Forks Community Hospital CHELAN GRAND COULEE BURIEN Lake Chelan Community Coulee Medical Center SEATTLE EDMONDS MONROE Hospital & Clinics SPOKANE VALLEY Highline Swedish Edmonds EvergreenHealth Monroe MultiCare Valley Hospital Kindred Hospital Seattle – Medical Center JEFFERSON KIRKLAND DAVENPORT Northgate & First Hill Regional Fairfax Behavioral Health DOUGLAS Lincoln Hospital u Navos Hospital for uSEATTLE EvergreenHealth LEAVENWORTH SPOKANE & MEDICAL LAKE Seattle Cancer Care Alliance Respiratory & See list BELLEVUE Cascade Medical Center See list Seattle Children’s Complex Care KITSAP Overlake Medical Center KING ISSAQUAH — Swedish/Issaquah MultiCare Deaconess Hospital Swedish Ballard BREMERTON BURIEN -

Participating Organization Locations UMP Plus – PSHVN Hospitals, Emergency Departments And/Or Trauma Centers and Clinics, Including Urgent Care
Network Organizations: Edmonds Family Medicine EvergreenHealth Partners MultiCare Connected Care Overlake Medical Center Rockwood Health System Seattle Children’s SignalHealth Virginia Mason Participating Organization Locations UMP Plus – PSHVN hospitals, emergency departments and/or trauma centers and clinics, including urgent care: Grays Harbor County ° EvergreenHealth Neuropsychological Services EvergreenHealth Orthopedic and Sports Care Grays Harbor Community Hospital and Harbor ° Medical Group (Part of MultiCare Connected Care) ° EvergreenHealth Orthopedic and Sports Care Monroe EvergreenHealth Orthpedics and Sports Medicine-Coral •• 915 Anderson Dr., Aberdeen, WA 98520 ° ° EvergreenHealth Pain Care ° 1006 North H St., Aberdeen, WA 98520 (East Campus) ° EvergreenHealth Parkinson’s Services EvergreenHealth Primary Care, Canyon Park King County ° ° EvergreenHealth Primary Care, Duvall EvergreenHealth Partners ° EvergreenHealth Primary Care, Kenmore ° Advanced Dermatology Northwest ° EvergreenHealth Primary Care, Monroe ° Advanced Family Medicine, PLLC •• EvergreenHealth Primary Care, Emergency Care & ° Aria Endocrinology, LLC Urgent Care Redmond ° Associated Gastroenterology of Northwest ° EvergreenHealth Primary Care, Sammamish ° Bellevue Bone & Joint Physicians, PLLC ° EvergreenHealth Primary Care, Sultan ° Bellevue Endocrine Consultants • EvergreenHealth Primary Care and Urgent Care Woodinville ° Bellevue Family Medicine ° EvergreenHealth Pulmonary Care ° Bellevue Lasik & Cataract ° EvergreenHealth Radiation Oncology ° Bel-Red Internal -
Quality Counts: Choose the Right Hospital and Doctor for You in The: Seattle Area
Quality Counts: Choose the right hospital and doctor for you in the: Seattle area WHAT IS TRANSPARENCY? Transparency in healthcare means having facts about cost and quality. As costs rise and provider networks narrow, it’s crucial that consumers have access to transparent information to make informed decisions when selecting the right hospital and the right doctor for their care. When presented with objective information about physician experience and related hospital quality, % OF PATIENTS 8would select5 a different physician than they did before doing their homework.* IN THE U.S. Consumers need to research the hospitals where physicians practice. Getting the right care means selecting the right doctor and the highest quality hospital for their care needs. MORE THAN 222,392 OUT LIVES POTENTIALLY OF COULD HAVE patients1 received care6 in 1-star BEEN SAVED hospitals with higher if all hospitals performed than expected mortality rates similarly to hospitals receiving or complication rates.** 5-stars.*** IN THE SEATTLE AREA Fortunately only By doing their homework, % consumers can select the of10.6 patients receive care right doctor and right in hospitals with higher than hospital for their care expected mortality rates or complication rates.** needs in the Seattle area. The Top Performers Before beginning their care journey, consumers should start their research at Healthgrades.com, where they can find the right hospital and the right doctor based on information physicians say matters most. By doing their homework, consumers can actively -

Emotional Effects” Section of Your Disaster Customer Service Kit
Taking the Report Directions for Taking the Loss Report To be used in new losses, call-backs and in-person. STEP ONE Identify/introduce yourself to the customer. Give your first and last name ________________________ and state “PEMCO Claims, how may I help you?” 1. Listen carefully and follow our insured’s lead. If they need to discuss other issues prior to taking the actual loss report, feel free to use your own judgment and do whatever seems best. 2. Remember that people in the midst of a disaster may exhibit behaviors (anger, grief, sadness, panic, anxiety, etc.) that require special handling on your part. See the “Emotional Effects” section of your Disaster customer Service Kit. STEP TWO Determine if this is a new loss report or a follow-up call to an existing claim: 1. If it’s a new loss report, take the report using your claim form. 2. If it’s an existing report, route the call or direct the claimant to the coverage confirmation group. STEP THREE Complete the Contingency/Storm Claim Form: 1. Document the date report made, time report taken and your name. 2. Document the insured’s name and the address of the insured property. 3. Document alternate addresses (for contact purposes). 4. Document insured’s e-mail address, phone number, and alternate phone numbers. 5. Document who reported the loss. 6. Record the type of policy (auto, property, mariner) and policy number (if available) at bottom of form. 7. Complete the loss description (include information about the damages to insured property, any injuries, fatalities, etc.). -

Swedish Ballard
Community Health Implementation Plan 2016-2018 Swedish Health Services Ballard Campus Table of contents Community Health Implementation Plan 2016-2018 Executive summary…………………….... page 3 Introduction……………………………...... page 5 Creating healthier communities, together Serving King County Purpose and process…………………..... page 7 Plan objective Prioritized health needs and community input page 10 Summary of Swedish prioritized needs and page 11 associated action plans Prioritized health needs o Access to Care o Preventable causes of death o Maternal/child health o Behavioral health o Violence and injury prevention Needs not addressed .............................. page 18 Next steps............................................... page 19 Plan approval .......................................... page 20 2 | P a g e Executive Summary Swedish Medical Center continually strives to honor its commitment to create healthier communities together. Partnering with others of similar intention, we conduct a formal community health needs assessment to learn about the greatest needs and assets from the perspective of some of the most marginalized groups of people in the communities we serve. This assessment helps us develop collaborative solutions to fulfill unmet needs while continuing to strengthen local resources. What follows is the Community Health Implementation Plan (CHIP) for Swedish Ballard. The CHIP is designed to be the “action plan” that will respond to the specific needs that were discovered during the assessment process. These plans are based on community health data and identifiable gaps in available care/services. It was determined that emphasis on these issues would ultimately have the greatest impact on the community’s overall health. The objective of the implementation plan is to measurably improve the health of the citizens in a specific community. -
Trauma Designated
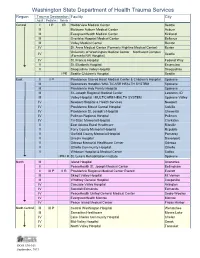
Washington State Department of Health Trauma Services Region Trauma Designation Facility City Adult Pediatric Rehab Central I I P IR Harborview Medical Center Seattle III Multicare Auburn Medical Center Auburn III EvergreenHealth Medical Center Kirkland III Overlake Hospital Medical Center Bellevue III Valley Medical Center Renton IV St. Anne Medical Center (Formerly Highline Medical Center) Burien University of Washington Medical Center – Northwest Campus IV Seattle (Formerly NW Hospital) IV St. Francis Hospital Federal Way V St. Elizabeth Hospital Enumclaw V Snoqualmie Valley Hospital Snoqualmie I PR Seattle Children’s Hospital Seattle East II II P Providence Sacred Heart Medical Center & Children’s Hospital Spokane III Deaconess Hospital / MULTICARE HEALTH SYSTEM Spokane III Providence Holy Family Hospital Spokane III St. Joseph Regional Medical Center Lewiston, ID III Valley Hospital / MULTICARE HEALTH SYSTEM Spokane Valley IV Newport Hospital & Health Services Newport IV Providence Mount Carmel Hospital Colville IV Providence St. Joseph’s Hospital Chewelah IV Pullman Regional Hospital Pullman IV Tri-State Memorial Hospital Clarkston V East Adams Rural Healthcare Ritzville V Ferry County Memorial Hospital Republic V Garfield County Memorial Hospital Pomeroy V Lincoln Hospital Davenport V Odessa Memorial Healthcare Center Odessa V Othello Community Hospital Othello V Whitman Hospital & Medical Center Colfax I PR-I R St. Luke’s Rehabilitation Institute Spokane North III Island Hospital Anacortes II PeaceHealth St. Joseph Medical Center -

Changes to Heritage Prime and Heritage Signature Networks Start Jan
FOR BENEFIT ADMINISTRATORS OF PREMERA BLUE CROSS GROUP MEDICAL PLANS Changes to Heritage Prime and Heritage Signature networks start Jan. 1, 2017 Starting Jan. 1, 2017, CHI Franciscan Health and Providence Health & Services, which includes Swedish Health Services, Swedish Edmonds, and PacMed systems, will not be part of the Heritage Prime and Heritage Signature networks offered by Premera medical plans. These changes impact only Providence and CHI Franciscan in Washington state. Although Harrison Medical Center, The Doctors Clinic, and Franciscan Medical Group in Kitsap County are affiliated with CHI Franciscan Health, they will remain part of the Heritage Prime and Heritage Signature networks to ensure members have in-network options for care. The Heritage Signature network is used by Premera’s small group plans (1-50). The Heritage Prime network is available to Premera’s large group customers (51+). Key facts Your options • Employees with the Heritage Prime or Heritage Signature network will have access to more than 33,000 providers across Washington state. If it is important for your group These providers share our commitment to quality care, managed costs, to maintain access to Providence and a better customer experience. Health & Services in 2017, you • If an employee is in the middle of care with a CHI Franciscan Health or should consider a plan that Providence hospital, facility, or physicians’ group on Jan. 1, 2017, Premera uses the Heritage network, our will work with them and their doctor to determine if continuity of care is broadest provider network. needed. Employees are encouraged to contact customer service for help. Groups will save money and • If an employee tries to schedule an appointment in 2017 with a CHI maintain access to a large Franciscan Health or Providence provider, they should be informed by the network of providers by using provider that they are not in network for Prime or Signature. -

Swedish Foot & Ankle Surgery and Medicine Program With
Additional Information Our Mission For further information about the Swedish • Develop highly skilled physicians who specialize in foot and ankle care Foot & Ankle Surgery and Medicine Swedish Foot & Ankle Program with Reconstructive Rearfoot/ • Provide a sound foundation of academic and Surgery and Medicine clinical education for our podiatric residents Ankle Surgery or Externship Program, please contact: Program with • Promote educational excellence throughout the medical community Swedish Foot & Ankle Surgery and Reconstructive Rearfoot/ Medicine Program with Reconstructive Ankle Surgery The Program Rearfoot/Ankle Surgery A Three-Year Program Emphasizing Swedish Foot & Ankle Surgery and Medicine Swedish Medical Center Reconstructive Foot and Ankle Surgery Program with Reconstructive Rearfoot/Ankle Graduate Medical Education-Podiatry and Traumatology Surgery is a three-year program in foot and 747 Broadway, WW-735 ankle medicine and surgery, including extensive Seattle, WA 98122 T 206-320-5301 training in reconstruction of the rearfoot and F 206-320-4780 ankle. It has been developed with special www.swedish.org/podiatricresidency emphasis on a multidisciplinary approach to lower-extremity disorders. The program is accredited by the Council on Podiatric Medical Education as a Podiatric Medicine & Surgery Residency with added reconstructive rearfoot/ankle surgery credential Swedish Foot & Ankle Surgery and (PMSR/RRA). Two residents are selected each Medicine Program with Reconstructive year. Rearfoot/Ankle Surgery This residency began in 1969 as the Waldo Residency Program and moved to its present location at Swedish in 1997. Application through SWEDISH FOOT & ANKLE SURGERY AND CASPR™ required MEDICINE PROGRAM WITH RECONSTRUCTIVE REARFOOT/ANKLE SURGERY www.swedish.org/podiatricresidency © 2013 SWEDISH HEALTH SERVICES. ALL RIGHTS RESERVED. -

Swedish Foot & Ankle Surgery and Medicine Program With
Additional information Our mission For further information about the Swedish • Develop highly skilled surgeons who specialize in comprehensive foot and Foot & Ankle Surgery and Medicine Swedish Foot & Ankle ankle care Program with Reconstructive Rearfoot/ Ankle Surgery or Externship Program, Surgery and Medicine • Foster and develop a robust foundation for academic and clinical leadership in please contact: Program with the podiatric community Swedish Foot & Ankle Surgery and Reconstructive Rearfoot/ Medicine Program with Reconstructive The program Rearfoot/Ankle Surgery Ankle Surgery Swedish Foot & Ankle Surgery and Medicine Podiatry Residency A three-year program emphasizing Program with Reconstructive Rearfoot/ 500 17th Ave. reconstructive foot and ankle surgery Ankle Surgery is a three-year program in foot Seattle, WA 98122 and traumatology and ankle medicine and surgery, including T 206-215-2221 extensive training in reconstruction of the E [email protected] rearfoot and ankle. It has been developed www.swedish.org/podiatryresidency with special emphasis on a multidisciplinary approach to lower-extremity disorders. The program is accredited by the Council on Podiatric Medical Education as a Podiatric Medicine & Surgery Residency with added reconstructive rearfoot/ankle surgery credential (PMSR/RRA). Two residents are selected each year. Swedish Foot & Ankle Surgery Due to our strong emphasis on and Medicine Program reconstructive rearfoot and ankle surgery, with Reconstructive our residents achieve well over the CPME required numbers to graduate. Rearfoot/Ankle Surgery SWEDISH FOOT & ANKLE SURGERY AND MEDICINE PROGRAM WITH RECONSTRUCTIVE REARFOOT/ANKLE SURGERY Application through CASPR™ required We do not discriminate on the basis of race, color, national origin, sex, age or disability in our health programs and activities. -
Manager and Executive Compensation in Hospitals and Health Systems Survey Report
2019 Manager and Executive Compensation in Hospitals and Health Systems Survey Report Survey data effective January 1, 2019 © 2019 SullivanCotter, Inc. All rights reserved. 200 W. Madison Street, Suite 2450 Chicago, IL 60606-3416 2019 MANAGER AND EXECUTIVE COMPENSATION IN HOSPITALS AND HEALTH SYSTEMS SURVEY REPORT Survey data effective January 1, 2019 LICENSE AGREEMENT LICENSE AGREEMENT By accessing or downloading the Survey Report files online or by opening the packaging for this Survey Report, you agree to the terms of this License Agreement (this “Agreement”). If you do not agree to these terms and have not yet accessed or downloaded the Survey Report files or opened the packaging for this Survey Report, you may cancel your online purchase or download at this time or you may return this Survey Report to SullivanCotter, Inc. for a full refund within thirty (30) days of receipt, but you may not access or download the Survey Report files or open the packaging for, or otherwise use, this Survey Report. Accessing or downloading the Survey Report files or opening the packaging, or otherwise using, this Survey Report binds you to this Agreement. This Agreement is entered into by and between SullivanCotter, Inc. ("SullivanCotter") and the purchaser or participant of this Survey Report (the “Licensee”). In consideration of the mutual covenants in this Agreement, SullivanCotter and the Licensee agree as follows: Grant of License. This Survey Report contains the aggregation of compensation data and other data provided to SullivanCotter by its survey participants, statistics, tables, reports, research, aggregations, calculations, data analysis, formulas, summaries, content, text and other information and materials provided to the Licensee by SullivanCotter through any other means, whether digital or hard copy, related thereto (the “Aggregated Data”). -

CN App #19-12 Swedish Issaquah
EVALUATION DATED SEPTEMBER 16, 2019, FOR THE CERTIFICATE OF NEED APPLICATION SUBMITTED BY SWEDISH HEALTH SERVICES PROPOSING TO ESTABLISH A 6-BED PEDIATRIC INTENSIVE CARE UNIT AT SWEDISH MEDICAL CENTER – ISSAQUAH CAMPUS, WITHIN KING COUNTY. APPLICANT DESCRIPTION Swedish Health Services (Swedish) is a not-for-profit health system serving the residents of King and Snohomish Counties and the surrounding areas. Swedish Health Services oversees operations of five hospital campuses, two free-standing emergency rooms, eight urgent care clinics, and a variety of primary and specialty care clinics, among others. [sources: Application pp7-8, Swedish website] Swedish Health Services affiliated with Providence Health & Services in 2011, which merged with St Joseph Health System in 2016 to form Providence St. Joseph Health (PH&S). Swedish currently operates through Western HealthConnect – a branch of Providence Ministries that is separate from Providence hospital operations. For ease of reference, the applicant will simple be referred to as “Swedish” throughout this evaluation. [source: CN Historical files] PROJECT DESCRIPTION This project focuses on Swedish Medical Center – Issaquah Campus, located in Issaquah. The hospital has been in operation since 2011 and provides a variety of healthcare services to the residents of East King County and surrounding communities. For reader ease, the hospital will be referred to as “Swedish Issaquah” throughout this evaluation. As of the writing of this evaluation, Swedish Issaquah is licensed for a total of 175 beds located at 751 Northeast Blakely Drive in Issaquah [98029]. Table 1 shows 175 beds broken down by service. [source: CN historical files] Table 1 Swedish Issaquah Current Configuration of Licensed Acute Care Beds Services Provided Beds General Medical Surgical 160 Intermediate Care Nursery - Level II 15 Total 175 As of the writing of this evaluation, Swedish Issaquah provides a variety of general medical surgical services, including intensive care, emergency services, and a Level II intermediate care nursery.