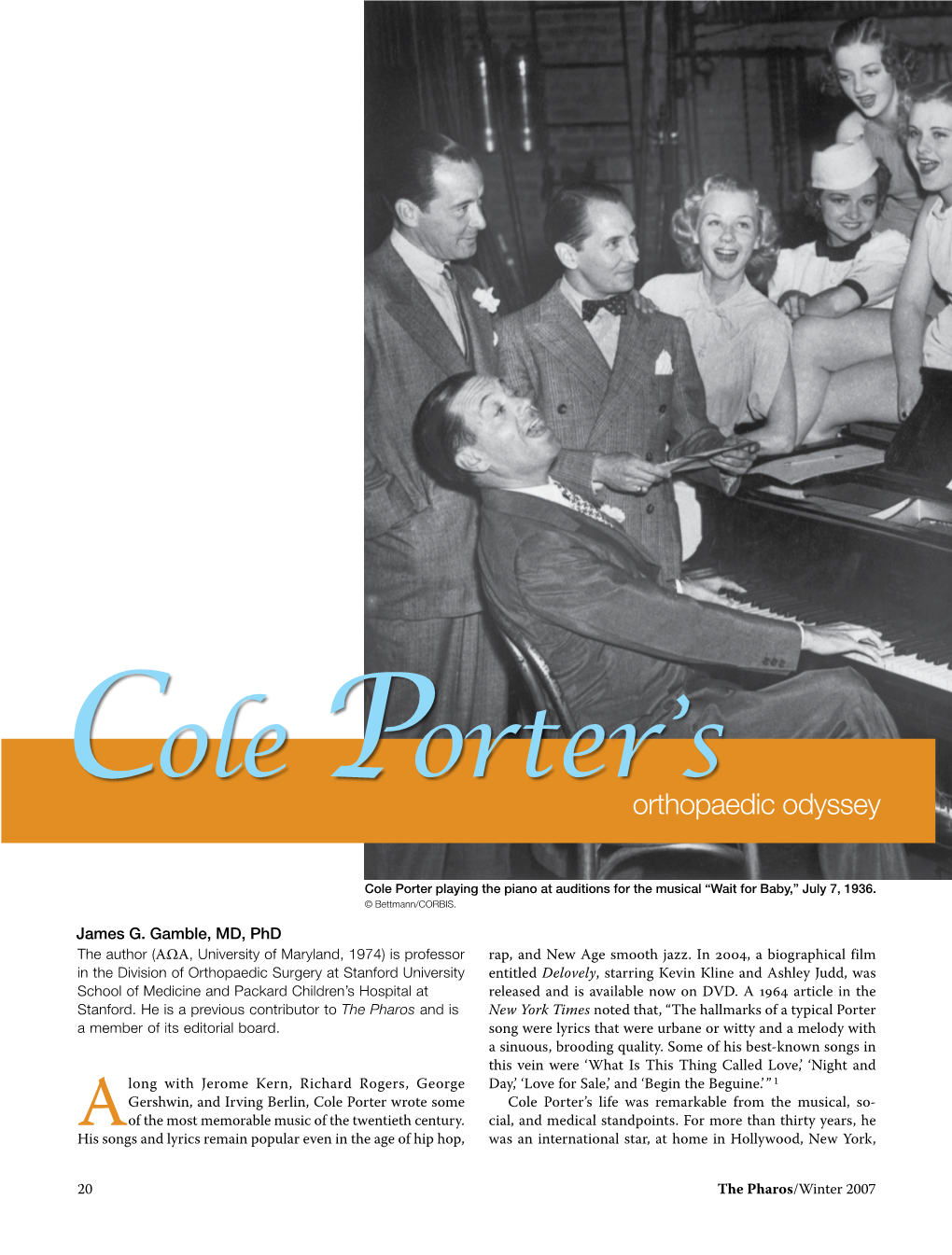
Cole Porter's
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Music, Dance and Theatre (MDT) 1
Music, Dance and Theatre (MDT) 1 MDT 510 Latin American Music (3 Credits) MUSIC, DANCE AND THEATRE A course in the music of selected Latin America countries offering music and Spanish-language majors and educators perspectives into the (MDT) musical traditions of this multifaceted region. Analysis of the music will be discussed in terms that accommodate non specialists, and all lyrics MDT 500 Louis Armstrong-American Hero (3 Credits) will be supplied with English translations. A study of the development of jazz with Louis Armstrong as the vehicle: MDT 511 Vocal Pedagogy (3 Credits) who he influenced and how he did it. Comparative analytical studies with This course is to provide the student of singing a deeper understanding his peers and other musicians are explored. of the vocal process, physiology, and synergistic nature of the vocal MDT 501 Baroque Music (3 Credits) mechanism. We will explore the anatomical construction of the voice as This course offers a study of 17th and 18th century music with particular well as its function in order to enlighten the performer, pedagogue and emphasis on the works of Johann Sebastian Bach, Dietrich Buxtehude, scholar. Each student will learn to codify a practical knowledge of, and Arcangelo Corelli, Francois Couperin, Andrea and Giovanni Gabrieli, skill in, teaching voice. George Frederick Handel, Jean-Baptiste Lully, Claudio Monteverdi, Jean- MDT 520 Musical On B'Way&Hollywood I (3 Credits) Philippe Rameau, Alessandro and Domenico Scarlatti, Gerog Telemann, This course offers an analysis of current Broadway musicals with special and Antonio Vivaldi. seminars with those connected with one or two productions. -

A Quantitative Analysis of the Songs of Cole Porter and Irving Berlin
i DEVELOPMENT OF CREATIVE EXPERTISE IN MUSIC: A QUANTITATIVE ANALYSIS OF THE SONGS OF COLE PORTER AND IRVING BERLIN A Dissertation Submitted to the Temple University Graduate Board In Partial Fulfillment of the Requirements for the Degree of Doctor of Philosophy By Richard W. Hass January, 2009 ii ABSTRACT Previous studies of musical creativity lacked strong foundations in music theory and music analysis. The goal of the current project was to merge the study of music perception and cognition with the study of expertise-based musical creativity. Three hypotheses about the nature of creativity were tested. According to the productive-thinking hypothesis, creativity represents a complete break from past knowledge. According to the reproductive-thinking hypothesis, creators develop a core collection of kernel ideas early in their careers and continually recombine those ideas in novel ways. According to what can be called the field hypothesis, creativity involves more than just the individual creator; creativity represents an interaction between the individual creator, the domain in which the creator works, and the field, or collection of institutions that evaluate creative products. In order to evaluate each hypothesis, the musical components of a sample of songs by two eminent 20 th century American songwriters, Cole Porter and Irving Berlin, were analyzed. Five separate analyses were constructed to examine changes in the psychologically salient musical components of Berlin’s and Porter’s songs over time. In addition, comparisons between hit songs and non-hit songs were also drawn to investigate whether the composers learned from their cumulative songwriting experiences. Several developmental trends were found in the careers of both composers; however, there were few differences between hit songs and non-hit songs on all measures. -

Download Chapter (PDF)
PLATES 1. Cole Porter, Yale yearbook photograph (1913). 2. Westleigh Farms, Cole Porter’s childhood home in Indiana (2011). 3. Cole Porter’s World War I draft registration card (5 June 1917). War Department, Office of the Provost Marshal General. 4. Linda Porter, passport photograph (1919). 5. Cole Porter, Linda Porter, Bernard Berenson and Howard Sturges in Venice (c.1923). 6. Gerald Murphy, Ginny Carpenter, Cole Porter and Sara Murphy in Venice (1923). 7. Serge Diaghilev, Boris Kochno, Bronislava Nijinska, Ernest Ansermet and Igor Stravinsky in Monte Carlo (1923). Library of Congress, Music Division, Reproduction number: 200181841. 8. Letter from Cole Porter to Boris Kochno (September 1925). Courtesy of The Cole Porter Musical and Literary Property Trusts. 9. Scene from the original stage production of Fifty Million Frenchmen (1929). PHOTOFEST. 10. Irene Bordoni, star of Porter’s show Paris (1928). 11. Sheet music, ‘Love for Sale’ from The New Yorkers (1930). 12. Production designer Jo Mielziner showing a set for Jubilee (1935). PHOTOFEST. 13. Cole Porter composing as he reclines on a couch in the Ritz Hotel during out-of-town tryouts for Du Barry Was a Lady (1939). George Karger / Getty Images. 14. Cole and Linda Porter (c.1938). PHOTOFEST. 15. Ethel Merman in the New York production of Cole Porter’s Panama Hattie (1940). George Karger / Getty Images. vi PLATES 16. Sheet music, ‘Let’s Be Buddies’ from Panama Hattie (1940). 17. Draft of ‘I Am Ashamed that Women Are So Simple’ from Kiss Me, Kate (1948), Library of Congress. Courtesy of The Cole Porter Musical and Literary Property Trusts. -

Groove Doctors - Song List
GROOVE DOCTORS - SONG LIST VOCAL STANDARDS A KISS TO BUILD A DREAM ON ALL THE WAY AT LAST AS TIME GOES BY BEYOND THE SEA BUT NOT FOR ME CHEEK TO CHEEK COME FLY WITH ME COME RAIN AND COME SHINE DO NOTHING TILL YOU HEAR FROM ME DOWN IN BRAZIL EAST OF THE SUN EMBRACEABLE YOU FLY ME TO THE MOON GREEN DOLPIN STREET HEART ANDSOUL HERE’S THAT RAINY DAY HOW HIGH THE MOON I CONCENTRATE ON YOU I LEFT MY HEART IN SAN FRANCISCO I LOVE BEIN HERE WITH YOU ISN’T IT ROMANTIC I THOUGHT ABOUT YOU IT DON’T MEAN A THING I’VE GOT THE WORLD ON A STRING I’VE GOT YOU UNDER MY SKIN I WANNA BE AROUND LET’S FALL IN LOVE LIKE A LOVER LIKE SOMEONE IN LOVE LOVE AND MARRIAGE LOVE DANCE MASQUERADE MISTY MOONDANCE MY FUNNY VALENTINE MY ONE AND ONLY LOVE MY ROMANCE NEW YORK NEW YORK NEW YORK STATE OF MIND NIGHT AND DAY VOCAL STANDARDS OLD DEVIL MOON ON THE SUNNY SIDE OF THE STREET OUR LOVE IS HERE TO STAY PIANO MAN RUBY RUBY SCOTCH AND SODA SINCE I FELL FOR YOU SOMEONE TO WATCH OVER ME SPEAK LOW STARDUST STEPPIN OUT WITH MY BABY STOMPIN AT THE SAVOY SUMMERTIME SUMMER WINDS TEACH ME TONIGHT THAT’S ALL THE BEST IS YET TO COME THE GOOD LIFE THE NEARNESS OF YOU THE SECOND TIME AROUND THE VERY THOUGHT OF YOU THE WAY YOU LOOK TONIGHT THERE WILL NEVER BE ANOTHER YOU TIME AFTER TIME UNFORGETTABLE WATCH WHAT HAPPENS WHAT A WONDERFUL WORLD WHAT ARE YOU DOIN NEW YEARS EVE WHEN I FALL IN LOVE WITCHCRAFT YOU DON’T KNOW ME YOU’D BE SO NICE TO COME HOME TO YOUR NOBODY TILL SOMEBODY LOVES YOU POP AND BALLADS ANOTHER STAR A SONG FOR YOU BACK AT ONE COPACABANA DADDY’S LITTLE GIRL FEEL LIKE -

KEVIN COLE “America's Pianist” Kevin Cole Has Delighted
KEVIN COLE “America’s Pianist” Kevin Cole has delighted audiences with a repertoire that includes the best of American Music. Cole’s performances have prompted accolades from some of the foremost critics in America. "A piano genius...he reveals an understanding of harmony, rhythmic complexity and pure show-biz virtuosity that would have had Vladimir Horowitz smiling with envy," wrote critic Andrew Patner. On Cole’s affinity for Gershwin: “When Cole sits down at the piano, you would swear Gershwin himself was at work… Cole stands as the best Gershwin pianist in America today,” Howard Reich, arts critic for the Chicago Tribune. Engagements for Cole include: sold-out performances with the Los Angeles Philharmonic at the Hollywood Bowl; BBC Concert Orchestra at Royal Albert Hall; National Symphony at the Kennedy Center; Hong Kong Philharmonic; San Francisco Symphony, Chicago Symphony, Philadelphia Orchestra, Philharmonia Orchestra (London); Boston Philharmonic, Adelaide Symphony Orchestra (Australia) Minnesota Orchestra, Pittsburgh Symphony, Dallas Symphony, Seattle Symphony,Vietnam National Symphony Orchestra; New Zealand Symphony, Edmonton Symphony (Canada), Ravinia Festival, Wolf Trap, Savannah Music Festival, Castleton Festival, Chautauqua Institute and many others. He made his Carnegie Hall debut with the Albany Symphony in May 2013. He has shared the concert stage with, William Warfield, Sylvia McNair, Lorin Maazel, Brian d’Arcy James, Barbara Cook, Robert Klein, Lucie Arnaz, Maria Friedman, Idina Menzel and friend and mentor Marvin Hamlisch. Kevin was featured soloist for the PBS special, Gershwin at One Symphony Place with the Nashville Symphony. He has written, directed, co- produced and performed multimedia concerts for: The Gershwin’s HERE TO STAY -The Gershwin Experience, PLAY IT AGAIN, MARVIN!-A Celebration of the music of Marvin Hamlisch with Pittsburgh Symphony and Chicago Symphony and YOU’RE THE TOP!-Cole Porter’s 125th Birthday Celebration and I LOVE TO RHYME – An Ira Gershwin Tribute for the Ravinia Festival with Chicago Symphony. -

Lister); an American Folk Rhapsody Deutschmeister Kapelle/JULIUS HERRMANN; Band of the Welsh Guards/Cap
Guild GmbH Guild -Light Catalogue Bärenholzstrasse 8, 8537 Nussbaumen, Switzerland Tel: +41 52 742 85 00 - e-mail: [email protected] CD-No. Title Track/Composer Artists GLCD 5101 An Introduction Gateway To The West (Farnon); Going For A Ride (Torch); With A Song In My Heart QUEEN'S HALL LIGHT ORCHESTRA/ROBERT FARNON; SIDNEY TORCH AND (Rodgers, Hart); Heykens' Serenade (Heykens, arr. Goodwin); Martinique (Warren); HIS ORCHESTRA; ANDRE KOSTELANETZ & HIS ORCHESTRA; RON GOODWIN Skyscraper Fantasy (Phillips); Dance Of The Spanish Onion (Rose); Out Of This & HIS ORCHESTRA; RAY MARTIN & HIS ORCHESTRA; CHARLES WILLIAMS & World - theme from the film (Arlen, Mercer); Paris To Piccadilly (Busby, Hurran); HIS CONCERT ORCHESTRA; DAVID ROSE & HIS ORCHESTRA; MANTOVANI & Festive Days (Ancliffe); Ha'penny Breeze - theme from the film (Green); Tropical HIS ORCHESTRA; L'ORCHESTRE DEVEREAUX/GEORGES DEVEREAUX; (Gould); Puffin' Billy (White); First Rhapsody (Melachrino); Fantasie Impromptu in C LONDON PROMENADE ORCHESTRA/ WALTER COLLINS; PHILIP GREEN & HIS Sharp Minor (Chopin, arr. Farnon); London Bridge March (Coates); Mock Turtles ORCHESTRA; MORTON GOULD & HIS ORCHESTRA; DANISH STATE RADIO (Morley); To A Wild Rose (MacDowell, arr. Peter Yorke); Plink, Plank, Plunk! ORCHESTRA/HUBERT CLIFFORD; MELACHRINO ORCHESTRA/GEORGE (Anderson); Jamaican Rhumba (Benjamin, arr. Percy Faith); Vision in Velvet MELACHRINO; KINGSWAY SO/CAMARATA; NEW LIGHT SYMPHONY (Duncan); Grand Canyon (van der Linden); Dancing Princess (Hart, Layman, arr. ORCHESTRA/JOSEPH LEWIS; QUEEN'S HALL LIGHT ORCHESTRA/ROBERT Young); Dainty Lady (Peter); Bandstand ('Frescoes' Suite) (Haydn Wood) FARNON; PETER YORKE & HIS CONCERT ORCHESTRA; LEROY ANDERSON & HIS 'POPS' CONCERT ORCHESTRA; PERCY FAITH & HIS ORCHESTRA; NEW CONCERT ORCHESTRA/JACK LEON; DOLF VAN DER LINDEN & HIS METROPOLE ORCHESTRA; FRANK CHACKSFIELD & HIS ORCHESTRA; REGINALD KING & HIS LIGHT ORCHESTRA; NEW CONCERT ORCHESTRA/SERGE KRISH GLCD 5102 1940's Music In The Air (Lloyd, arr. -

Cole Porter: the Social Significance of Selected Love Lyrics of the 1930S
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Unisa Institutional Repository Cole Porter: the social significance of selected love lyrics of the 1930s by MARILYN JUNE HOLLOWAY submitted in accordance with the requirements for the degree of MASTER OF ARTS in the subject of ENGLISH at the UNIVERSITY OF SOUTH AFRICA SUPERVISOR: PROFESSOR IA RABINOWITZ November 2010 DECLARATION i SUMMARY This dissertation examines selected love lyrics composed during the 1930s by Cole Porter, whose witty and urbane music epitomized the Golden era of American light music. These lyrics present an interesting paradox – a man who longed for his music to be accepted by the American public, yet remained indifferent to the social mores of the time. Porter offered trenchant social commentary aimed at a society restricted by social taboos and cultural conventions. The argument develops systematically through a chronological and contextual study of the influences of people and events on a man and his music. The prosodic intonation and imagistic texture of the lyrics demonstrate an intimate correlation between personality and composition which, in turn, is supported by the biographical content. KEY WORDS: Broadway, Cole Porter, early Hollywood musicals, gays and musicals, innuendo, musical comedy, social taboos, song lyrics, Tin Pan Alley, 1930 film censorship ii ACKNOWLEDGEMENTS I should like to thank Professor Ivan Rabinowitz, my supervisor, who has been both my mentor and an unfailing source of encouragement; Dawie Malan who was so patient in sourcing material from libraries around the world with remarkable fortitude and good humour; Dr Robin Lee who suggested the title of my dissertation; Dr Elspa Hovgaard who provided academic and helpful comment; my husband, Henry Holloway, a musicologist of world renown, who had to share me with another man for three years; and the man himself, Cole Porter, whose lyrics have thrilled, and will continue to thrill, music lovers with their sophistication and wit. -

Cole Albert Porter (June 9, 1891 October 15, 1964) Was An
Cole Albert Porter (June 9, 1891 October 15, 1964) was an American composer and songwriter. Born to a wealthy family in Indiana, he defied the wishes of his dom ineering grandfather and took up music as a profession. Classically trained, he was drawn towards musical theatre. After a slow start, he began to achieve succe ss in the 1920s, and by the 1930s he was one of the major songwriters for the Br oadway musical stage. Unlike many successful Broadway composers, Porter wrote th e lyrics as well as the music for his songs. After a serious horseback riding accident in 1937, Porter was left disabled and in constant pain, but he continued to work. His shows of the early 1940s did not contain the lasting hits of his best work of the 1920s and 30s, but in 1948 he made a triumphant comeback with his most successful musical, Kiss Me, Kate. It w on the first Tony Award for Best Musical. Porter's other musicals include Fifty Million Frenchmen, DuBarry Was a Lady, Any thing Goes, Can-Can and Silk Stockings. His numerous hit songs include "Night an d Day","Begin the Beguine", "I Get a Kick Out of You", "Well, Did You Evah!", "I 've Got You Under My Skin", "My Heart Belongs to Daddy" and "You're the Top". He also composed scores for films from the 1930s to the 1950s, including Born to D ance (1936), which featured the song "You'd Be So Easy to Love", Rosalie (1937), which featured "In the Still of the Night"; High Society (1956), which included "True Love"; and Les Girls (1957). -

Paris, New York, and Post-National Romance
Sex and the Series: Paris, New York, and Post-National Romance Dana Heller / love Paris every moment, Every moment of the year I love Paris, why oh why do I love Paris? Because my love is here. —Cole Porter, / Love Paris This essay will examine and contrast two recent popular situation comedies, NBC's Friends and HBO's Sex and the City, as narratives that participate in the long-standing utilization of Paris as trope, or as an instrumental figure within the perennially deformed and reformed landscape of the American national imaginary. My argument is that Paris re-emerges in post-9/11 popular culture as a complex, multi-accentual figure within the imagined mise-en-scene of the world Americans desire. The reasons for this are to a large degree historical: in literature, cinema, television, popular music, and other forms of U.S. cultural production, from the late nineteenth century through the twentieth century and into the twenty first, Paris has remained that city where one ventures, literally and/or imaginatively, to dismember history, or to perform a disarticulation of the national subject that suggests possibilities for the interrogation of national myths and for 0026-3079/2005/4602-145$2.50/0 American Studies, 46:1 (Summer 2005): 145-169 145 146 Dana Heller the articulation of possible new forms of national unity and allegiance. These forms frequently find expression in the romantic transformation of a national citizen-subject into a citizen-subject of the world, a critique of the imperialist aspirations of the nation-state that antithetically masks those same aspirations under the sign of the disillusioned American cosmopolitan abroad. -

June 2015 President: Vice President: Price 50P When Sold Simon Russell Beale CBE Nickolas Grace
No. 491 - June 2015 President: Vice President: Price 50p when sold Simon Russell Beale CBE Nickolas Grace WHAT A SWELL PARTY IT WAS! Liz Schafer reviews Shakespeare’s Birthday Party 2015 This year’s Shakespeare’s Birthday Party was marked by a ‘can do’ spirit of improvisation and the result was a thoroughly enjoyable event. The Old Vic circle bar, where the party is normally held these days, was full of props and so there was no room for the party. Crisis! But Ned Seago, the Old Vic doorman, arranged for the party to be held instead backstage in the rehearsal room. Once the rehearsal room had been commandeered, Nickolas Grace stood outside the theatre greeting guests with his usual charm and directing us to the Webber Street Stage Door entrance. After we had all recovered from the lift, which probably should be granted ancient monument status – it had lovely wooden panelling and a sign sternly warning Maria Friedman with Jamie Parker and The Bard everyone that ‘weight must be evenly distributed’, we were able to relax in the open, airy rehearsal room. This, as members with long memories reminded us, used to be the venue for the VWA parties. I would certainly vote for parties being held there in the future if at all possible. As Nick pointed out, although the floorboards were now sanded down, they were the very ones trodden by stars such as Olivier, Ashcroft, Gielgud in their days at the Vic, when they were in rehearsal. Nick certainly had plenty of interesting memories of working in that room. -
The First Screen Jeeves
Plum L in es The quarterly journal of The Wodehouse Society Vol. 22 No. 2 Summer 2001 The First Screen Jeeves By Brian Taves Brian Taves (PhD, University of Southern California) is a film archivist at the Library of Congress and author of three books. t the end o f 1935,20th detective, and Chan was A Century-Fox bought the studio’s most popular the film rights to Thank “star” after Shirley Ton, Jeeves (along with a Temple. one-year option on the Like Chan, Jeeves had other stories) and the right been brought to the no to make other films cen tice of the American read tered around Jeeves. Look ing public in The Saturday ing for potentially pro Evening Post. The Jeeves lific—and profitable — film series seems to have properties, the studio was been launched on what interested in any character was perceived as a sure who seemed to have the bet, casting Arthur potential to lure filmgoers Treacher, known for play to film after film, no less ing butler roles, as the fa than a modern television mous literary butler. series. Earlier in the year, However, while the Chan Fox’s merger with 20th series was cast and pre Century had enhanced the sented in a manner conso A studio photo of the three principals in the first Jeeves film: studio’s status, and a CCB” nant with Biggers’s liter David Niven, Virginia Field, and Arthur Treacher. unit was organized under ary creation, the Jeeves Sol Wurtzel, who had a $6,000,000 annual budget for films revealed no sense of the situations and character pat 24 “Bs” per year. -

Wodehouse and the Baroque*1
Connotations Vol. 20.2-3 (2010/2011) Worcestershirewards: Wodehouse and the Baroque*1 LAWRENCE DUGAN I should define as baroque that style which deli- berately exhausts (or tries to exhaust) all its pos- sibilities and which borders on its own parody. (Jorge Luis Borges, The Universal History of Infamy 11) Unfortunately, however, if there was one thing circumstances weren’t, it was different from what they were, and there was no suspicion of a song on the lips. The more I thought of what lay before me at these bally Towers, the bowed- downer did the heart become. (P. G. Wodehouse, The Code of the Woosters 31) A good way to understand the achievement of P. G. Wodehouse is to look closely at the style in which he wrote his Jeeves and Wooster novels, which began in the 1920s, and to realise how different it is from that used in the dozens of other books he wrote, some of them as much admired as the famous master-and-servant stories. Indeed, those other novels and stories, including the Psmith books of the 1910s and the later Blandings Castle series, are useful in showing just how distinct a style it is. It is a unique, vernacular, contorted, slangy idiom which I have labeled baroque because it is in such sharp con- trast to the almost bland classical sentences of the other Wodehouse books. The Merriam Webster’s Collegiate Dictionary describes the ba- roque style as “marked generally by use of complex forms, bold or- *For debates inspired by this article, please check the Connotations website at <http://www.connotations.de/debdugan02023.htm>.