Collection Tube Guide for the Full Array of BD Vacutainer® Blood Collection Tubes, Visit
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Enoxaparin Sodium Solution for Injection, Manufacturer's Standard
PRODUCT MONOGRAPH INCLUDING PATIENT MEDICATION INFORMATION PrLOVENOX® Enoxaparin sodium solution for injection 30 mg in 0.3 mL solution (100 mg/mL), pre-filled syringes for subcutaneous or intravenous injection 40 mg in 0.4 mL solution (100 mg/mL), pre-filled syringes for subcutaneous or intravenous injection 60 mg in 0.6 mL solution (100 mg/mL), pre-filled syringes for subcutaneous or intravenous injection 80 mg in 0.8 mL solution (100 mg/mL), pre-filled syringes for subcutaneous or intravenous injection 100 mg in 1 mL solution (100 mg/mL), pre-filled syringes for subcutaneous or intravenous injection 300 mg in 3 mL solution (100 mg/mL), multidose vials for subcutaneous or intravenous injection PrLOVENOX® HP Enoxaparin sodium (High Potency) solution for injection 120 mg in 0.8 mL solution (150 mg/mL), pre-filled syringes for subcutaneous or intravenous injection 150 mg in 1 mL solution (150 mg/mL), pre-filled syringes for subcutaneous or intravenous injection Manufacturer’s standard Anticoagulant/Antithrombotic Agent ATC Code: B01AB05 Product Monograph – LOVENOX (enoxaparin) Page 1 of 113 sanofi-aventis Canada Inc. Date of Initial Approval: 2905 Place Louis-R.-Renaud February 9, 1993 Laval, Quebec H7V 0A3 Date of Revision September 7, 2021 Submission Control Number: 252514 s-a version 15.0 dated September 7, 2021 Product Monograph – LOVENOX (enoxaparin) Page 2 of 113 TABLE OF CONTENTS Sections or subsections that are not applicable at the time of authorization are not listed. TABLE OF CONTENTS .............................................................................................................. -

Handout Page 1 of 8
MLT 112: Principles of Phlebotomy Learning Unit 3: Handout Specimen Collection – Venipuncture Procedure I. Collecting and Processing of Specimens A. Blood 1. Venipuncture Procedure (arm + dorsal/hand) – vacutainer, syringe, butterfly a. Approaching the Patient Correct patient identification Wash hands Have patient recite his/her name Wrist identification – mandatory must match requisition check ankle on babies and peds Out-patients – ask patient to spell name In-patients – see wrist ID Unconscious patient – see wrist ID Unidentified patient – emergency – use temporary I.D. band non-emergency – wait for I.D. Explanation and Reassurance – Inspire confidence Conversation Ensure that patient has complied with test requirements, such as fasting (only water), NPO (nothing per oral), etc. Check for any allergies, such as to latex, adhesive bandages, etc. b. Positions Positioning the patient Vein accessibility Sitting vs. lying down Phlebotomist position – always in front in case of fainting. c. Applying the Tourniquet See previous lecture Page 1 of 8 MLT 112: Principles of Phlebotomy Learning Unit 3: Handout d. Veins Used - Antecubital Fossa Cephalic Median Cephalic Median Basilic Median Cubital Vein – vein of choice, anchored best Other Structures – avoid Brachial artery – apply pressure 5 minutes Cutaneous nerve – very painful Tendon for the biceps muscle – always draw below crease e. Other Vein Sites Wrist (never palm side) Hand Ankle Foot f. Preparing Equipment Syringes Assembly – always work plunger before procedure. Plunger position – must -

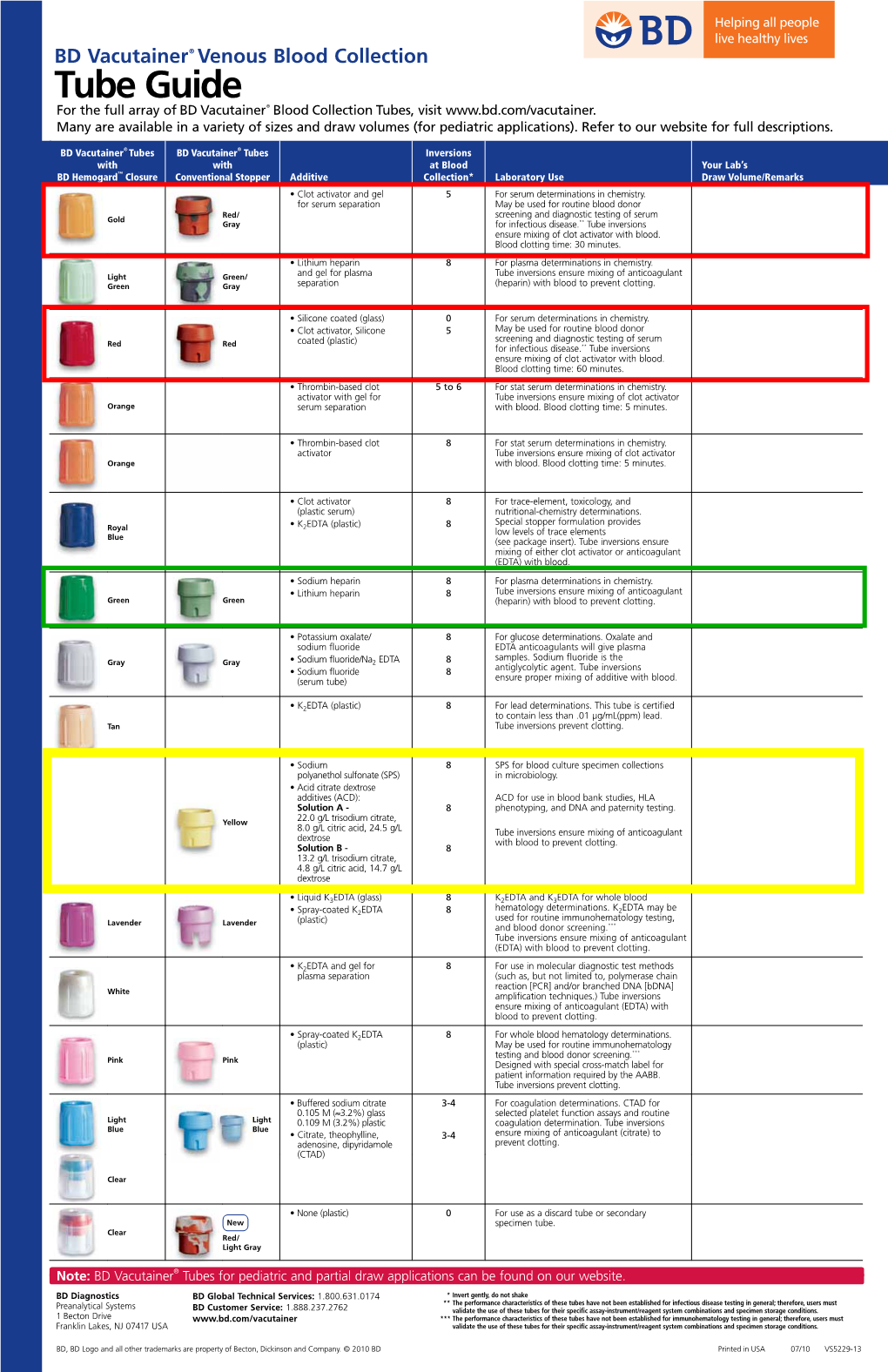
Vacutainer Tubes
Vacutainer Tube Guide - Order of Draw for routine volumes See separate guide for micro-tainers Number of Tube Inversions at Label Blood Collection Volume Tubes/Bottles Abbrev. Additive (Do Not Shake) General Laboratory Use Draw 1 Aerobic and 1 5 Blood Culture / requires Adapter 20 mL Anaerobic Culture Note: A separate venipuncture for trace BLCLT Bottles metal analysis is required if blood cultures are ordered at the same time. NAYYP Clot activator 8 Trace Element serum tube for Copper 6 mL Royal Trace Element whole blood for Aluminum, NAVYE 2 Call 2-5002 Blue K EDTA Lead, Zinc, Selenium, Manganese, Mercury, 8 for tubes Cadmium, Arsenic Discard tube or secondary sterile specimen 6 mL Clear None 0 tube 3 mL 2.7 mL Light (Blue) BLUE Sodium Citrate (3.2%) Coagulation Testing on Plasma Blue 3-4 1.8 mL (Blue/clear) Serum determinations where a gel-barrier is 6 mL Red RED Clot Activator 5 contraindicated; Therapeutic Drug 4 mL Monitoring (TDM) Clot Activator and gel SST - Serum determinations in Chemistry, Gold SST 5 5 mL for serum separation Immunology, Serology; HLA Ab screen, DSA Light Lithium heparin and PST PST - Plasma determinations in Chemistry 4.5 mL Green gel - plasma separation 8 GLI Lithium heparin 8 Whole Blood Plasma: Troponin, Lactic Acid, Ion. Ca+ 6 mL Dark 4 mL Green GNA Sodium heparin 8 Whole Blood Plasma: Tissue typing, plasma hemoglobin, plasma catecholamine, chromosome analysis Pink PINK Dry K2EDTA 8 Blood Bank / Transfusion; HLA Typing 6 mL Tan TAN K2EDTA 8 Lead Testing only 3 mL LAV 4 Whole Blood Hematology; some Flow, 4 mL Lavender Dry K2EDTA 8 Molecular, and Genetic tests; HIV Viral 2 mL LAV6 Load Whole Blood tube with Glycolytic inhibitor Potassium Oxalate / for GTT, Gray 6 mL GRAY Sodium fluoride 8 Post-Prandial Glucose, D-Xylose, and Volatiles panel ACDA ACD Whole Blood tube for Flow Yellow (Acid Citrate Dextrose 8 immunophenotyping; HLA cross matching; 8.5 mL ACDB Solution A) genetic and other referred tests ALWAYS Check Expiration Dates before use! If unsure of use, refer to the on-line “Lab User’s Guide” or call the lab at 25002 . -

Rtpa) for the Treatment of Hepatic Veno-Occlusive Disease (VOD
Bone Marrow Transplantation, (1999) 23, 803–807 1999 Stockton Press All rights reserved 0268–3369/99 $12.00 http://www.stockton-press.co.uk/bmt Recombinant tissue plasminogen activator (rtPA) for the treatment of hepatic veno-occlusive disease (VOD) S Kulkarni1, M Rodriguez2, A Lafuente2, P Mateos2, J Mehta1, S Singhal1, R Saso3, D Tait4, JG Treleaven3 and RL Powles1 Departments of 1Medical Oncology, 3Haematology and 4Radiotherapy, Royal Marsden NHS Trust, Sutton, Surrey, UK; and 2Haematology Department, Hospital La Paz, Madrid, Spain Summary: clinical syndrome characterized by hyperbilirubinemia, hepatomegaly and fluid retention,2,3 and results from dam- Seventeen patients who developed hepatic veno-occlus- age to structures in zone 3 of the liver acinus.4 In patients ive disease (VOD) following hematopoietic stem cell who have undergone hematopoietic stem cell transplan- transplantation were treated with recombinant tissue tation, chemoradiotherapy-induced endothelial cell damage plasminogen activator (rtPA) with or without heparin. is likely to be responsible for the pathogenesis of vessel rtPA was started a median of 13 days post transplant obstruction.5 (range 4–35). All patients received rtPA at a dose of 10 Treatment of established VOD has primarily been sup- mg/day as a starting dose, and 12 patients also received portive and any specific measures have resulted in little heparin (1500 U bolus; then 100 U/kg/day as a continu- impact on outcome. Based on the available evidence for ous i.v. infusion). The median number of days of rtPA involvement of hemostatic mechanisms and cytokines in therapy was 2.5 (1–12). The median total serum biliru- the pathogenesis of VOD,6–8 anti-thrombotic and anti-cyto- bin level was 116 mmol/l (range 63–194) at the begin- kine agents have been assessed for their role in treatment. -

Transition of Anticoagulants 2019
Transition of Anticoagulants 2019 Van Hellerslia, PharmD, BCPS, CACP, Brand Generic Clinical Assistant Professor of Pharmacy Practice, Angiomax bivalirudin Temple University School of Pharmacy, Philadelphia, PA Arixtra fondaparinux Bevyxxa betrixaban Pallav Mehta, MD, Assistant Professor of Medicine, Coumadin warfarin Division of Hematology/Oncology, Eliquis apixaban MD Anderson Cancer Center at Cooper, Camden, NJ Fragmin dalteparin Lovenox enoxaparin Reviewer: Kelly Rudd, PharmD, BCPS, CACP, Pradaxa dabigatran Clinical Specialist, Anticoagulation, Bassett Medical Center, Savaysa edoxaban Cooperstown, NY Xarelto rivaroxaban From To Action Apixaban Argatroban/ Wait 12 hours after last dose of apixaban to initiate parenteral anticoagulant. In cases of Bivalirudin/ high bleeding risk, consider omitting initial bolus when transitioning to heparin infusion. Enoxaparin/ Dalteparin/ Fondaparinux/ Heparin Apixaban Warfarin When going from apixaban to warfarin, consider the use of parenteral anticoagulation as a bridge (eg, start heparin infusion or therapeutic enoxaparin AND warfarin 12 hours after last dose of apixaban and discontinue parenteral anticoagulant when INR is therapeutic). Apixaban affects INR so that initial INR measurements during the transition may not be useful for determining the appropriate dose of warfarin. Apixaban Betrixaban, Wait 12 hours from last dose of apixaban to initiate betrixaban, dabigatran, edoxaban, or Dabigatran, rivaroxaban. Edoxaban, or Rivaroxaban Argatroban Apixaban, Start apixaban, betrixaban, dabigatran, -

(Dipotassium Salt) and Heparin on the Estimation of Packed Cell Volume
J Clin Pathol: first published as 10.1136/jcp.19.2.196 on 1 March 1966. Downloaded from J. clin. Path. (1966), 19, 196 Effect of ethylene-diamine-tetra-acetic acid (dipotassium salt) and heparin on the estimation of packed cell volume C. A. PENNOCK AND K. W. JONES From the Department of Haematology, Gibson Laboratories, Radcliffe Infirmary, Oxford SYNOPSIS The effect of varying concentrations of ethylene-diamine-tetra-acetic acid (E.D.T.A.) (dipotassium salt) and heparin on the estimation of packed cell volume has been studied using a microhaematocrit method. Varying concentrations of E.D.T.A. can produce serious errors in estimation of packed cell volume (P.C.V.) and reliable results are only obtained within the range of 1 to 2 mg./ml. Heparin is a more suitable anticoagulant for this investigation as varying the con- centration has little effect. Storage with either anticoagulant at suitable concentrations for 24 hours at room temperature has little influence on the results. The estimation ofthe packed cell volume (P.C.V.) is bottles are often returned to this laboratory contain- regarded as a reliable investigation in the diagnosis ing less than the recommended amount of blood.copyright. of anaemia, and errors in the estimation of mean Ethylene-diamine-tetra-acetic acid is known to corpuscular haemoglobin concentration (M.C.H.C.) cause distortion and shrinkage of red cells and are thought to be due more often to errors in the to affect the estimation of P.C.V. by conventional estimation of haemoglobin than of the P.C.V. -

Direct Versus Indirect Thrombin Inhibition in Percutaneous Coronary Intervention
Direct Versus Indirect Thrombin Inhibition in Percutaneous Coronary Intervention Jonathan D. Marmur, MD, FACC Heparin rally occurring but slow thrombin inhibitor. The heparin:AT interaction produces conformational Heparin has been used to prevent intravascular changes in AT and accelerates its inhibition of throm- thrombosis and clotting on the surface of equipment bin, factor Xa, and factor IXa.10 used during percutaneous coronary interventions (PCI) Heparin catalysis of factor Xa inhibition does not since Andreas Gruentzig performed the first require bridging between factor Xa and AT. Since almost angioplasty.1 In fact, the development of coronary all the heparin chains are at least 18 units long, heparin angioplasty and of coronary artery bypass surgery would has equivalent inhibitory activity against thrombin and probably not have been possible without heparin. How- factor Xa.3 However, when thrombin is bound to fibrin, ever, with the availability of low molecular weight the heparin:AT complex is less able to access and inhibit heparin (LMWH) and the approval of bivalirudin, a thrombin.9 Furthermore, with respect to anti Xa activity, direct thrombin inhibitor for use during PCI, the ques- the heparin:AT complex is unable to inhibit factor Xa tion is more and more frequently asked whether heparin bound to the surface of activated platelets.11 should be replaced in PCI. The purpose of this paper is to critically review the evidence for the use of heparins Pharmacokinetics/pharmacodynamics. Heparin (indirect thrombin inhibitors) and direct thrombin must be given by injection since it is not absorbed when inhibitors during PCI. administered orally.10 Heparin is cleared via a biphasic process combining rapid saturable and slower first- Structure and mechanism of action of heparin. -

Public Assessment Report
PUBLIC ASSESSMENT REPORT Decentralised Procedure Fraxiparine 0.3 2,850 I.U. anti-Xa/ 0.3 ml; Fraxiparine 0.4 3,800 I.U. anti-Xa/ 0.4 ml; Fraxiparine 0.6 5,700 I.U. anti-Xa/ 0.6 ml; Fraxiparine 0.8 7,600 I.U. anti-Xa/ 0.8 ml Procedure Number: DE/H/4762/002-005/DC Fraxodi 19000 UL / ml; 0.6 ml Fraxodi 19000 UL / ml; 0.8 ml Fraxodi 19000 UL / ml; 1.0 ml Procedure Number: DE/H/4763/001-003/DC Fraxiparine Multi 9,500 anti-Xa IU/ 1.0 ml Fraxiparine Multi 9,500 anti-Xa IU/ 1.0 ml Procedure Number: DE/H/4770/001-002/DC Active Substance: Nadroparin-Calcium Dosage Form: Solution for injection Marketing Authorisation Holder in the RMS, Germany: Aspen Pharma Trading Limited Publication: 19.11.2018 TABLE OF CONTENTS I. RECOMMENDATION ................................................................................................................ 4 II. EXECUTIVE SUMMARY ....................................................................................................... 4 II.1 Problem statement ..................................................................................................................... 4 II.2 About the product ..................................................................................................................... 4 II.3 General comments on the submitted dossier .......................................................................... 4 II.4 General comments on compliance with GMP, GLP, GCP and agreed ethical principles. 5 III. SCIENTIFIC OVERVIEW AND DISCUSSION .................................................................. -
Laboratory-General Specimen Collection and Handling Guidelines
Laboratory-General Specimen Collection and Handling Guidelines Contents: Microbiology continued. Orders/Requests Stool Patient Preparation Throat or Pharynx Specimen Containers Tuberculosis (TB) Specimen Quality Urine Order of Draw Viral Specimen Transport VRE Surveillance (Vancomycin- Resistant entercoccus) Specimen Rejection Wound General Lab Sample/Source: Whole Blood Cytology (Cytopathology) Plasma Aspiration, Fine Needle Serum Aspiration, Cyst Fluids Urine Submission of slide Fecal (Stool) Tips on making smears Body Fluid Body Cavity Fluids Cerebrospinal Spinal Fluid Breast Nipple Secretions Synovial Fluid Brushing Specimens Microbiology Cerebrospinal Fluid (CSF) Sample/Source: Ectocervix, Endocervical canal, Vaginal pool Abscess (Deep aspirate) Pap Smear, Conventional Abscess (superficial swab) Pap Smear, Liquid Base Acid Fast Bacillus (AFB) Sputum Specimens Anaerobic Surface Scrape Specimen (Tzanck Smear) Aspirate, drainage, cyst fluid, or pustule Vaginal Wall (Maturation Index) Biopsy, Bone, Tissue Washing Specimens Blood (Adult) Histology (Anatomic Pathology) Blood )Pediatric Routine Submission Blood for Acid Fast Bacillus (AFB) Fresh Specimen Body Fluids Surgical Specimen and Microbiology test(s) Bronchial Washing Lavage Breast Tissue Catheter Tip Brushing Specimens C. difficile Toxin B Bronchial Washing and Brushings Chlamydia/Gonorrhea Amplified Detection Muscle Biopsy Crytococcal Antigen Renal Biopsy (Kidney) Cerebral Spinal Fluid (CSF) Renal calculi (Kidney/Bladder Stones) Ear (outer) Bone Marrow Ear (inner) Cytogenics Eye -

Elective Surgery and Invasive Procedures in Patients Taking
Volume 10, No. 5 January 2020 This Medicines Information Leaflet is produced locally to optimise the use of medicines by encouraging prescribing that is safe, clinically appropriate and cost-effective to the NHS. The management of patients who are receiving oral therapy if they are regarded as at high risk of anticoagulation with warfarin or a Direct Oral thrombosis (see table 1). The dose of dalteparin Anticoagulant (DOAC e.g. dabigatran, rivaroxaban, recommended for bridging is outlined in table 2. apixaban, edoxaban) who require surgery or are All patients who do not require bridging with full undergoing a procedure depends on the underlying treatment dose heparin peri-operatively should be thrombotic risk, the intended surgical intervention, risk assessed and given prophylactic dose LMWH as and the risk of bleeding associated with it. This MIL appropriate. covers the management of patients on warfarin or a DOAC undergoing elective procedures, grouped into Table 1: Consider bridging with full treatment dose three categories: major surgery (excluding vascular heparin in patients who stop warfarin if thrombotic surgery), minor surgery and endoscopy. risk is high Note: Patients within 3 months of acute venous Consider bridging with full treatment dose thromboembolism (VTE) are at high risk of recurrent heparin in: VTE if anticoagulation is stopped; it is estimated that VTE Patients with a VTE within previous 3 cessation of anticoagulation in the first month after months. an acute VTE is associated with a 40% one-month risk of recurrent VTE, and 10% for the subsequent Very high risk patients such as patients with two months. Therefore, wherever possible elective a previous VTE whilst on therapeutic surgery should be delayed until 3 months after an anticoagulation who now have a target INR acute VTE. -

Research Article Comparison of Small-Volume Tubes and Vacuum
INTERNATIONAL JOURNAL OF MEDICAL BIOCHEMISTRY DOI: 10.14744/ijmb.2018.69188 Int J Med Biochem 2019;2(1):24-9 Research Article Comparison of small-volume tubes and vacuum blood tubes for complete blood count Kubranur Unal Department of Biochemistry, Polatlı Public Hospital, Ankara, Turkey Abstract Objectives: A complete blood count (CBC) is one of the most commonly requested clinical laboratory tests. Vacuum blood tubes are used routinely, and now, new small-volume tubes (SVTs) containing dipotassium ethylenediaminete- traacetic acid (K2EDTA) are also in use. The aim of this research was to compare SVTs with vacuum blood tubes for use in a CBC. Methods: Venous blood samples were taken from 40 healthy volunteers and were collected in BD Vacutainer (Becton, Dickinson and Company, Franklin Lakes, NJ, USA) K2EDTA tubes and BD Microtainer (Becton, Dickinson and Company, Franklin Lakes, NJ, USA) K2EDTA tubes. CBC parameters were analyzed using an ABX Pentra DF 120 device (Horiba, Ltd., Kyoto, Japan). Results: Red blood cells (RBC), hemoglobin (HGB), hematocrit (HCT), mean corpuscular hemoglobin (MCH), mean cor- puscular hemoglobin concentration (MCHC), and basophil (BASO) levels were found to be statistically significantly higher, while platelet (PLT) levels were determined to be statistically significantly lower in the SVT analyses compared with those of the vacuum blood tubes. When the percentage difference was compared with the total allowable error, RBC, HGB, HCT, MCH, MCHC, red cell distribution width, white blood cell count, neutrophil, lymphocyte, monocyte, eosinophil, and BASO values demonstrated a general trend of positive bias, while PLT values demonstrated a general trend of negative bias on a Bland-Altman bias plot. -

Cleveland Clinic Anticoagulation Management Program (C-Camp)
CLEVELAND CLINIC ANTICOAGULATION MANAGEMENT PROGRAM (C-CAMP) 1 Table of Contents I. EXECUTIVE SUMMARY ......................................................................................................................................... 6 II. VENOUS THROMBOEMBOLISM RISK ASSESSMENT AND PROPHYLAXIS ............................................. 9 III. RECOMMENDED PROPHYLAXIS OPTIONS FOR THE PREVENTION OF VENOUS THROMBOEMBOLISM. ........................................................................................................................................ 10 IIIA. RECOMMENDED PROPHYLAXIS OPTIONS FOR THE PREVENTION OF VENOUS THROMBOEMBOLISM BASED ON RISK FACTOR ASSESSMENT ............................................................. 12 A) UNFRACTIONATED HEPARIN (UFH) ................................................................................................................... 14 B) LOW MOLECULAR WEIGHT HEPARIN (LMWH) ENOXAPARIN (LOVENOX®) .............................................. 14 C) FONDAPARINUX/ (ARIXTRA®) …………………………………………………………………………..……16 D) RIVAROXABAN (XARELTO®) .......................................................................................................................... 16 E) DESIRUDIN (IPRIVASK®)………………………………………………………………………………..…….17 F) WARFARIN/COUMADIN®) ............................................................................................................................... 16 G) ASPIRIN……………………………………………………………………………………………………..……18 H) INTERMITTENT PNEUMATIC COMPRESSION DEVICES .....................................................................................