Expert John L
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Enoxaparin Sodium Solution for Injection, Manufacturer's Standard
PRODUCT MONOGRAPH INCLUDING PATIENT MEDICATION INFORMATION PrLOVENOX® Enoxaparin sodium solution for injection 30 mg in 0.3 mL solution (100 mg/mL), pre-filled syringes for subcutaneous or intravenous injection 40 mg in 0.4 mL solution (100 mg/mL), pre-filled syringes for subcutaneous or intravenous injection 60 mg in 0.6 mL solution (100 mg/mL), pre-filled syringes for subcutaneous or intravenous injection 80 mg in 0.8 mL solution (100 mg/mL), pre-filled syringes for subcutaneous or intravenous injection 100 mg in 1 mL solution (100 mg/mL), pre-filled syringes for subcutaneous or intravenous injection 300 mg in 3 mL solution (100 mg/mL), multidose vials for subcutaneous or intravenous injection PrLOVENOX® HP Enoxaparin sodium (High Potency) solution for injection 120 mg in 0.8 mL solution (150 mg/mL), pre-filled syringes for subcutaneous or intravenous injection 150 mg in 1 mL solution (150 mg/mL), pre-filled syringes for subcutaneous or intravenous injection Manufacturer’s standard Anticoagulant/Antithrombotic Agent ATC Code: B01AB05 Product Monograph – LOVENOX (enoxaparin) Page 1 of 113 sanofi-aventis Canada Inc. Date of Initial Approval: 2905 Place Louis-R.-Renaud February 9, 1993 Laval, Quebec H7V 0A3 Date of Revision September 7, 2021 Submission Control Number: 252514 s-a version 15.0 dated September 7, 2021 Product Monograph – LOVENOX (enoxaparin) Page 2 of 113 TABLE OF CONTENTS Sections or subsections that are not applicable at the time of authorization are not listed. TABLE OF CONTENTS .............................................................................................................. -

Gastrostomy Feeding Tubes
Gastrostomy feeding tubes With Dr Anastasia Volovets, Gastroenterologist and Hepatologist, Royal Prince Alfred Hospital, Sydney, Australia Introduction In patients with prolonged inadequate or absent oral intake gastrostomy tubes can be used to provide a route for enteral feeding, hydration, and medication administration. Case 1 - You are a junior doctor on the wards and you’re called to see a 65 year old male, who is day 5 post- stroke with an impaired swallow he is unable to tolerate oral feed and his family is worried he will starve to death. 1. Management of this patient IV fluids do not provide the caloric support or nutrients needed by patients, after 48 hours of impaired oral feeding, enteral feeding should be considered. • Short term this would be a nasogastric tube • Longer term (greater than 6 weeks) a gastrostomy or jejunostomy should be considered 2. Indications for enteral feeding • Neurological disorders causing impaired swallowing and aspiration of food o Stroke (most common) o Traumatic brain injury o Parkinson’s disease • Structural problems o Malignancy obstructing the gastrointestinal tract, this can include upper GI, head, nose or throat. Gastrostomy insertion can be done prophylactically prior to treatment that will impair the functioning or path of the tract such as surgery or radiotherapy 3. Contraindications to gastric feeding tubes • Absolute o High bleeding risk - uncorrected coagulopathy, thrombocytopenia o Chronic liver disease - varies and ascites o Peritonitis or abdominal perforation o Cellulitis at selected -

High Number of Endometrial Polyps Is a Strong Predictor of Recurrence: findings of a Prospective Cohort Study in Reproductive-Age Women
ORIGINAL ARTICLE: GYNECOLOGY AND MENOPAUSE High number of endometrial polyps is a strong predictor of recurrence: findings of a prospective cohort study in reproductive-age women Fang Gu, M.D.,a Huanxiao Zhang, M.D.,b Simin Ruan, M.D.,c Jiamin Li, M.D.,d Xinyan Liu, M.D.,a Yanwen Xu, M.D.,a,e and Canquan Zhou, M.D.a,e a Center for Reproductive Medicine, Department of Obstetrics and Gynecology, b Division of Gynecology, Department of Obstetrics and Gynecology, and c Department of Medical Ultrasonics, Institute of Diagnostic and Interventional Ultrasound, First Affiliated Hospital of Sun Yat-sen University; d Department of Obstetrics and Gynecology, Second Affiliated Hospital of Guangzhou Medical College; and e Key Laboratory of Reproductive Medicine of Guangdong Province, Guangzhou, People's Republic of China Objective: To compare the incidence of recurrence between a cohort with a high number (R6) of endometrial polyps (EPs) and a single- EP cohort among reproductive-age patients after polypectomy. Design: Prospective observational cohort study. Setting: Single university center. Patient(s): Premenopausal women who underwent hysteroscopic endometrial polypectomy were recruited. Intervention(s): Patients underwent a transvaginal ultrasound scan every 3 months after polypectomy to detect EP recurrence. Kaplan- Meier and Cox regression models were used to compare the risk of recurrence between the two cohorts and analyze the potential risk factors for EP recurrence. Main Outcome Measure(s): EP recurrence rate. Result(s): The study enrolled 101 cases with a high number of EP and 81 cases with a single EP. All baseline parameters were similar except that the high number of EP cohort had a slightly lower mean age than the single EP cohort (33.5 [range 30.0–39.0] vs. -

Pancreaticogastrostomy
eCommons@AKU Section of General Surgery Department of Surgery October 2017 Pancreaticogastrostomy - an alternate for dealing with pancreatic remnant after pancreaticoduodenectomy - experience from a tertiary care center of Pakistan Tabish Chawla Aga Khan University, [email protected] Hassaan Bari Aga Khan University Shahrukh Effendi Follow this and additional works at: https://ecommons.aku.edu/pakistan_fhs_mc_surg_gen Part of the Surgery Commons Recommended Citation Chawla, T., Bari, H., Effendi, S. (2017). Pancreaticogastrostomy - an alternate for dealing with pancreatic remnant after pancreaticoduodenectomy - experience from a tertiary care center of Pakistan. Journal of Pakistan Medical Association, 67(10), 1621-1624. Available at: https://ecommons.aku.edu/pakistan_fhs_mc_surg_gen/76 1621 CASE SERIES Pancreaticogastrostomy — an alternate for dealing with pancreatic remnant after pancreaticoduodenectomy — experience from a tertiary care center of Pakistan Tabish Chawla, Hassaan Bari, Shahrukh Effendi Abstract as part of PD. Therefore it was associated with high Whipple's pancreaticoduodenectomy has been refined morbidity and mortality resulting from high rates of over the years to be a safe operation though the leakage from pancreatic stump. morbidity rate still remains high (30-50%). Pancreatic Pancreatcogastrostomy is a repopularized technique fistula is the most important cause of mortality which has been described previously in literature. 3 This following pancreaticoduodenectomy. To prevent it, study was done to review the experience of PG being surgeons have used two anastomotic techniques: done as an alternate to PJ after PD. pancreaticojejunostomy and pancreaticogastrostomy. Recent studies found that pancreaticogastrostomy is Material and Methods associated with fewer overall complications than It is a case series collected at the Department of Surgery of pancreaticojejunostomy. -

High Risk Percutaneous Endoscopic Gastrostomy Tubes: Issues to Consider
NUTRITIONINFLAMMATORY ISSUES BOWEL IN GASTROENTEROLOGY, DISEASE: A PRACTICAL SERIES APPROACH, #105 SERIES #73 Carol Rees Parrish, M.S., R.D., Series Editor High Risk Percutaneous Endoscopic Gastrostomy Tubes: Issues to Consider Iris Vance Neeral Shah Percutaneous endoscopy gastrostomy (PEG) tubes are a valuable tool for providing long- term enteral nutrition or gastric decompression; certain circumstances that complicate PEG placement warrant novel approaches and merit review and discussion. Ascites and portal hypertension with varices have been associated with poorer outcomes. Bleeding is one of the most common serious complications affecting approximately 2.5% of all procedures. This article will review what evidence exists in these high risk scenarios and attempt to provide more clarity when considering these challenging clinical circumstances. INTRODUCTION ince the first Percutaneous Endoscopic has been found by multiple authors to portend a poor Gastrostomy tube was placed in 1979 (1), they prognosis in PEG placement (3,4, 5,6,7,8). This review Shave become an invaluable tool for providing will endeavor to provide more clarity when considering long-term enteral nutrition (EN) and are commonly used these challenging clinical circumstances. in patients with dysphagia following stroke, disabling motor neuron diseases such as multiple sclerosis and Ascites & Gastric Varices amyotrophic lateral sclerosis, and in those with head The presence of ascites is frequently viewed as a and neck cancer.They are also used for patients with relative, if not absolute, contraindication to PEG prolonged mechanical intubation, as well as gastric placement. Ascites adds technical difficulties and the decompression in those with severe gastroparesis, risk for potential complications (see Table 1). -

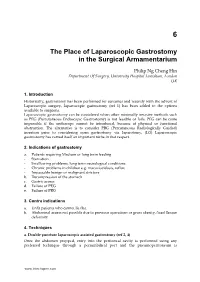
Quick Guide to Gastrostomy Feeding Tubes and Devices
QUICK GUIDE TO GASTROSTOMY FEEDING TUBES AND DEVICES A gastrostomy feeding tube or device is one which has been inserted directly through the abdominal wall into the stomach. It is secured by an internal retention device (either a balloon or a soft disc known as a “bumper”) on the inside and a firm external retention device (known as a “flange”) on the outside.11 Placement of a ballooned gastrostomy tube Cross-section: non-ballooned tube Oesophagus Stomach Clamp External Flange Gastrostomy tube Skin Fat Muscle Skin Internal Bumper Stomach Photo: APhoto: Kennedy Photo: MPhoto: Sutherland Patient with a ballooned gastrostomy Patient lying down with a non-ballooned tube insitu gastrostomy tube in situ See page 8 and 9 for a summary of the different types of tubes and devices you might see. A Clinician’s Guide: Caring for people with gastrostomy tubes and devices 7 Common features of gastrostomy feeding tubes and devices include, but are not limited to: Refer to manufacturer’s guidelines for advice on brand specific tube and device features Ballooned Gastrostomy Tube Ballooned Gastrostomy Tube With side port Without side port Feeding Port Feeding Port (Enteral Dispenser (Enteral Dispenser and Feed Bag and Feed Bag connect here) connect here) ml/cc Balloon Port Balloon Port ml/cc Side Port (X ml/cc) (X ml/cc) French (size) [For example:16/18/20] French (size) [For example:16/18/20] FR FR cm markings cm markings External External Flange Flange Balloon Balloon Non-ballooned Gastrostomy Tube Non-ballooned Gastrostomy Tube with collapsible internal -

ANMC Specialty Clinic Services
Cardiology Dermatology Diabetes Endocrinology Ear, Nose and Throat (ENT) Gastroenterology General Medicine General Surgery HIV/Early Intervention Services Infectious Disease Liver Clinic Neurology Neurosurgery/Comprehensive Pain Management Oncology Ophthalmology Orthopedics Orthopedics – Back and Spine Podiatry Pulmonology Rheumatology Urology Cardiology • Cardiology • Adult transthoracic echocardiography • Ambulatory electrocardiology monitor interpretation • Cardioversion, electrical, elective • Central line placement and venous angiography • ECG interpretation, including signal average ECG • Infusion and management of Gp IIb/IIIa agents and thrombolytic agents and antithrombotic agents • Insertion and management of central venous catheters, pulmonary artery catheters, and arterial lines • Insertion and management of automatic implantable cardiac defibrillators • Insertion of permanent pacemaker, including single/dual chamber and biventricular • Interpretation of results of noninvasive testing relevant to arrhythmia diagnoses and treatment • Hemodynamic monitoring with balloon flotation devices • Non-invasive hemodynamic monitoring • Perform history and physical exam • Pericardiocentesis • Placement of temporary transvenous pacemaker • Pacemaker programming/reprogramming and interrogation • Stress echocardiography (exercise and pharmacologic stress) • Tilt table testing • Transcutaneous external pacemaker placement • Transthoracic 2D echocardiography, Doppler, and color flow Dermatology • Chemical face peels • Cryosurgery • Diagnosis -

Rtpa) for the Treatment of Hepatic Veno-Occlusive Disease (VOD
Bone Marrow Transplantation, (1999) 23, 803–807 1999 Stockton Press All rights reserved 0268–3369/99 $12.00 http://www.stockton-press.co.uk/bmt Recombinant tissue plasminogen activator (rtPA) for the treatment of hepatic veno-occlusive disease (VOD) S Kulkarni1, M Rodriguez2, A Lafuente2, P Mateos2, J Mehta1, S Singhal1, R Saso3, D Tait4, JG Treleaven3 and RL Powles1 Departments of 1Medical Oncology, 3Haematology and 4Radiotherapy, Royal Marsden NHS Trust, Sutton, Surrey, UK; and 2Haematology Department, Hospital La Paz, Madrid, Spain Summary: clinical syndrome characterized by hyperbilirubinemia, hepatomegaly and fluid retention,2,3 and results from dam- Seventeen patients who developed hepatic veno-occlus- age to structures in zone 3 of the liver acinus.4 In patients ive disease (VOD) following hematopoietic stem cell who have undergone hematopoietic stem cell transplan- transplantation were treated with recombinant tissue tation, chemoradiotherapy-induced endothelial cell damage plasminogen activator (rtPA) with or without heparin. is likely to be responsible for the pathogenesis of vessel rtPA was started a median of 13 days post transplant obstruction.5 (range 4–35). All patients received rtPA at a dose of 10 Treatment of established VOD has primarily been sup- mg/day as a starting dose, and 12 patients also received portive and any specific measures have resulted in little heparin (1500 U bolus; then 100 U/kg/day as a continu- impact on outcome. Based on the available evidence for ous i.v. infusion). The median number of days of rtPA involvement of hemostatic mechanisms and cytokines in therapy was 2.5 (1–12). The median total serum biliru- the pathogenesis of VOD,6–8 anti-thrombotic and anti-cyto- bin level was 116 mmol/l (range 63–194) at the begin- kine agents have been assessed for their role in treatment. -

The Appropriate Time Interval Between Hysteroscopic Polypectomy and the Start of FET : a Retrospective Corchort Study
The Appropriate Time Interval Between Hysteroscopic Polypectomy and the Start of FET : A Retrospective Corchort Study Zhong-Kai Wang Zhengzhou University Third Hospital and Henan Province Women and Children's Hospital Hong-Wu Qiao Zhengzhou University Third Hospital and Henan Province Women and Children's Hospital She-Ling Wu Zhengzhou University Third Hospital and Henan Province Women and Children's Hospital Wen Zhang Zhengzhou University Third Hospital and Henan Province Women and Children's Hospital Xiao-Na Yu Zhengzhou University Third Hospital and Henan Province Women and Children's Hospital Jing Li Zhengzhou University Third Hospital and Henan Province Women and Children's Hospital Xing-Ling Wang Zhengzhou University Third Hospital and Henan Province Women and Children's Hospital Hua Lou Zhengzhou University Third Hospital and Henan Province Women and Children's Hospital Yi-Chun Guan ( [email protected] ) Zhengzhou University Third Hospital and Henan Province Women and Children's Hospital https://orcid.org/0000-0002-0312-3984 Research Keywords: Endometrial polyps, hysteroscopy, polypectomy, Frozen-embryo transfer, timing Posted Date: November 19th, 2020 DOI: https://doi.org/10.21203/rs.3.rs-110131/v1 License: This work is licensed under a Creative Commons Attribution 4.0 International License. Read Full License Page 1/14 Abstract Objective: To investigate when is the appropriate time interval between hysteroscopic polypectomy and the start of FET cycles Design: Retrospective cohort study. Setting: Academic center. Patient(s): All patients diagnosed with endometrial polyps undergoing hysteroscopic polypectomy before FET. Intervention(s): Hysteroscopic polypectomy. MainOutcomeMeasure(s): Patients were divided into four groups based on the time interval between hysteroscopic polypectomy and the start of FET Demographics, baseline FET characteristics, pregnancy outcomes after FET were compared among the groups. -
The Place of Laparoscopic Gastrostomy in the Surgical Armamentarium
6 The Place of Laparoscopic Gastrostomy in the Surgical Armamentarium Philip Ng Cheng Hin Department Of Surgery, University Hospital Lewisham, London UK 1. Introduction Historically, gastrostomy has been performed for centuries and recently with the advent of Laparoscopic surgery, laparoscopic gastrostomy (ref 1) has been added to the options available to surgeons. Laparoscopic gastrostomy can be considered when other minimally invasive methods such as PEG (Percutaneous Endoscopic Gastrostomy) is not feasible or fails. PEG can be come impossible if the endoscope cannot be introduced, because of physical or functional obstruction. The alternative is to consider PRG (Percutaneous Radiologically Guided) insertion prior to considering open gastrostomy via laparotomy, (LG) Laparoscopic gastrostomy has carved itself an important niche in that respect. 2. Indications of gastrostomy a. Patients requiring Medium or long term feeding - Starvation - Swallowing problems, long term neurological conditions - Chronic problems in children e.g. mucoviscidosis, reflux - Impassable benign or malignant stricture b. Decompression of the stomach c. Gastric access d. Failure of PEG e. Failure of PRG 3. Contra indications a. Unfit patients who cannot lie flat. b. Abdominal access not possible due to previous operations or gross obesity, fixed flexion deformity. 4. Techniques a. Double puncture laparoscopic assisted gastrostomy (ref 2, 4) Once the abdomen prepped, entry into the peritoneal cavity is performed using any preferred technique through a periumbilical port and the pneumoperitoneum is www.intechopen.com 84 Gastrostomy established, the anterior wall of the stomach is identified with certainty, and a second port (10mm) is inserted at a convenient point on the anterior abdominal wall. This operative step is greatly assisted by changing the position of the operating table 20 degrees head up. -

Gastrostomy Allows Removal of Obstructive Pancreatic Duct Stones
Original article Antegrade pancreatoscopy via EUS-guided pancreatico- gastrostomy allows removal of obstructive pancreatic duct stones Authors Theodore W. James, Todd H. Baron Institution pancreaticolithiasis, including use of pancreatoscopy for in- Division of Gastroenterology and Hepatology, University of traductal electrohydraulic lithotripsy (IEHL). Pancreatosco- North Carolina, Chapel Hill, North Carolina, United States py is often limited by a small-caliber downstream pancreat- ic duct as well as an unstable pancreatoscope position submitted 8.3.2018 within the pancreatic head. Endoscopic ultrasound-guided accepted after revision 11.4.2018 pancreaticogastrostomy (EUS-PG) has been developed as a method to relieve ductal obstruction when retrograde ac- Bibliography cess fails. The current study describes pancreatoscopy via DOI https://doi.org/10.1055/a-0607-2484 | EUS-PG, a novel method for managing obstructing pancrea- Endoscopy International Open 2018; 06: E735–E738 ticolithiasis. © Georg Thieme Verlag KG Stuttgart · New York Patients and methods From September 2017 to January ISSN 2364-3722 2018, patients who underwent EUS-PG followed by ante- grade pancreatoscopy via PG were identified. Endoscopy re- Corresponding author ports, medical charts and relevant laboratory data were re- Todd Huntley Baron, MD, Division of Gastroenterology and viewed and recorded. Hepatology, University of North Carolina School of Results Five patients underwent EUS-PG and antegrade Medicine, 101 Manning Drive, Chapel Hill, NC 27599 pancreatoscopy via PG during the study period; clinical suc- Fax: +1-984-974-0744 cess rate was 100%. There were no significant adverse [email protected] events during the procedure or follow up period. Conclusions Pancreatoscopy via PG for IEHL is safe and ef- fective for treating obstructing pancreaticolithiasis in pa- ABSTRACT tients who have previously failed ERCP or in clinical scenar- Background and study aims Endoscopic retrograde cho- ios were ERCP is not possible. -

Post-Polypectomy Colonoscopy Surveillance: European Society of Gastrointestinal Endoscopy (ESGE) Guideline – Update 2020
Guideline Post-polypectomy colonoscopy surveillance: European Society of Gastrointestinal Endoscopy (ESGE) Guideline – Update 2020 Authors Cesare Hassan1, Giulio Antonelli1, Jean-Marc Dumonceau2, Jaroslaw Regula3, Michael Bretthauer4,Stanislas Chaussade5, Evelien Dekker6, Monika Ferlitsch7, Antonio Gimeno-Garcia8,RodrigoJover9,MetteKalager4,Maria Pellisé10,ChristianPox11, Luigi Ricciardiello12, Matthew Rutter13, Lise Mørkved Helsingen4, Arne Bleijenberg6,Carlo Senore14, Jeanin E. van Hooft6, Mario Dinis-Ribeiro15, Enrique Quintero8 Institutions 13 Gastroenterology, University Hospital of North Tees, 1 Gastroenterology Unit, Nuovo Regina Margherita Stockton-on-Tees, UK and Northern Institute for Hospital, Rome, Italy Cancer Research, Newcastle University, Newcastle 2 Gastroenterology Service, Hôpital Civil Marie Curie, upon Tyne, UK Charleroi, Belgium 14 Epidemiology and screening Unit – CPO, Città della 3 Centre of Postgraduate Medical Education and Maria Salute e della Scienza University Hospital, Turin, Italy Sklodowska-Curie Memorial Cancer Centre, Institute of 15 CIDES/CINTESIS, Faculty of Medicine, University of Oncology, Warsaw, Poland Porto, Porto, Portugal 4 Clinical Effectiveness Research Group, Oslo University Hospital and University of Oslo, Norway Bibliography 5 Gastroenterology and Endoscopy Unit, Faculté de DOI https://doi.org/10.1055/a-1185-3109 Médecine, Hôpital Cochin, Assistance Publique- Published online: 22.6.2020 | Endoscopy 2020; 52: 1–14 Hôpitaux de Paris (AP-HP), Université Paris Descartes, © Georg Thieme Verlag