SUMMARY of DRUG LIMITATIONS Medications Listed in This Document May Or May Not Require a Prior Authorization
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Genmab and ADC Therapeutics Announce Amended Agreement for Camidanlumab Tesirine (Cami)
Genmab and ADC Therapeutics Announce Amended Agreement for Camidanlumab Tesirine (Cami) Media Release Copenhagen, Denmark and Lausanne, Switzerland, October 30, 2020 • ADC Therapeutics to continue the development and commercialization of Cami • Genmab to receive mid-to-high single-digit tiered royalty Genmab A/S (Nasdaq: GMAB) and ADC Therapeutics SA (NYSE: ADCT) today announced that they have executed an amended agreement for ADC Therapeutics to continue the development and commercialization of camidanlumab tesirine (Cami). The parties first entered into a collaboration and license agreement in June 2013 for the development of Cami, an antibody drug conjugate (ADC) which combines Genmab’s HuMax®-TAC antibody targeting CD25 with ADC Therapeutics’ highly potent pyrrolobenzodiazepine (PBD) warhead technology. Under the terms of the 2013 agreement, the parties were to determine the path forward for continued development and commercialization of Cami upon completion of a Phase 1a/b clinical trial. ADC Therapeutics previously announced that Cami achieved an overall response rate of 86.5%, including a complete response rate of 48.6%, in Hodgkin lymphoma patients in this trial who had received a median of five prior lines of therapy. Cami is currently being evaluated in a 100-patient pivotal Phase 2 clinical trial intended to support the submission of a Biologics License Application (BLA) to the U.S. Food and Drug Administration (FDA). The trial is more than 50 percent enrolled and ADC Therapeutics anticipates reporting interim results in the first half of 2021. “We have a long-standing relationship with the ADC Therapeutics team and believe they are an ideal partner for the ongoing development and potential commercialization of Cami,” said Jan van de Winkel, Ph.D., Chief Executive Officer of Genmab. -

Emergency Use Authorization (EUA) for Sotrovimab 500 Mg Center for Drug Evaluation and Research (CDER) Review
Emergency Use Authorization (EUA) for Sotrovimab 500 mg Center for Drug Evaluation and Research (CDER) Review Identifying Information Application Type EUA (EUA or Pre-EUA) If EUA, designate whether pre-event or intra-event EUA request. EUA Application EUA 000100 Number(s) Sponsor (entity EUA Sponsor requesting EUA or GlaxoSmithKline Research & Development Limited pre-EUA 980 Great West Road consideration), point Brentford Middlesex, TW8 9GS of contact, address, UK phone number, fax number, email GSK US Point of Contact address Debra H. Lake, M.S. Sr. Director Global Regulatory Affairs GlaxoSmithKline 5 Moore Drive PO Box 13398 Research Triangle Park, NC 27709-3398 (b) (6) Email: Phone Manufacturer, if GlaxoSmithKline, Parma. different from Sponsor Submission Date(s) Part 1: March 24, 2021 Part 2: March 29, 2021 Receipt Date(s) Part 1: March 24, 2021 Part 2: March 29, 2021 OND Division / Office Division of Antivirals /Office of Infectious Disease 1 Reference ID: 4802027 Product in the No Strategic National Stockpile (SNS) Distributor, if other (b) (4) than Sponsor I. EUA Determination/Declaration On February 4, 2020, the Secretary of Health and Human Services determined pursuant to section 564 of the Federal Food, Drug and Cosmetic (FD&C) Act that there is a public health emergency that has a significant potential to affect national security or the health and security of United States (US) citizens living abroad and that involves a novel (new) coronavirus (nCoV) first detected in Wuhan City, Hubei Province, China in 2019 (2019-nCoV). The virus is now named SARS-CoV-2, which causes the illness COVID-19. -

Minutes of the CHMP Meeting 14-17 September 2020
13 January 2021 EMA/CHMP/625456/2020 Corr.1 Human Medicines Division Committee for medicinal products for human use (CHMP) Minutes for the meeting on 14-17 September 2020 Chair: Harald Enzmann – Vice-Chair: Bruno Sepodes Disclaimers Some of the information contained in these minutes is considered commercially confidential or sensitive and therefore not disclosed. With regard to intended therapeutic indications or procedure scopes listed against products, it must be noted that these may not reflect the full wording proposed by applicants and may also vary during the course of the review. Additional details on some of these procedures will be published in the CHMP meeting highlights once the procedures are finalised and start of referrals will also be available. Of note, these minutes are a working document primarily designed for CHMP members and the work the Committee undertakes. Note on access to documents Some documents mentioned in the minutes cannot be released at present following a request for access to documents within the framework of Regulation (EC) No 1049/2001 as they are subject to on- going procedures for which a final decision has not yet been adopted. They will become public when adopted or considered public according to the principles stated in the Agency policy on access to documents (EMA/127362/2006). 1 Addition of the list of participants Official address Domenico Scarlattilaan 6 ● 1083 HS Amsterdam ● The Netherlands Address for visits and deliveries Refer to www.ema.europa.eu/how-to-find-us Send us a question Go to www.ema.europa.eu/contact Telephone +31 (0)88 781 6000 An agency of the European Union © European Medicines Agency, 2020. -

Draft Minutes PDCO 12-15 November 2019
11 December 2019 EMA/PDCO/615413/2019 Inspections, Human Medicines Pharmacovigilance and Committees Division Paediatric Committee (PDCO) Minutes for the meeting on 12-15 November 2019 Chair: Koenraad Norga – Vice-Chair: Sabine Scherer Health and safety information In accordance with the Agency’s health and safety policy, delegates are to be briefed on health, safety and emergency information and procedures prior to the start of the meeting. Disclaimers Some of the information contained in these minutes is considered commercially confidential or sensitive and therefore not disclosed. With regard to intended therapeutic indications or procedure scopes listed against products, it must be noted that these may not reflect the full wording proposed by applicants and may also vary during the course of the review. Additional details on some of these procedures will be published in the PDCO Committee meeting reports (after the PDCO Opinion is adopted), and on the Opinions and decisions on paediatric investigation plans webpage (after the EMA Decision is issued). Of note, this set of minutes is a working document primarily designed for PDCO members and the work the Committee undertakes. Further information with relevant explanatory notes can be found at the end of this document. Note on access to documents Some documents mentioned in these minutes cannot be released at present following a request for access to documents within the framework of Regulation (EC) No 1049/2001 as they are subject to on- going procedures for which a final decision has not yet been adopted. They will become public when adopted or considered public according to the principles stated in the Agency policy on access to documents (EMA/127362/2006). -

Mark Taylor; [email protected]; (317) 276-5795 (Media) Kevin Hern; Hern Kevin [email protected]; (317) 277-1838 (Investors)
January 29, 2021 Eli Lilly and Company Lilly Corporate Center Indianapolis, Indiana 46285 U.S.A. +1.317.276.2000 www.lilly.com For Release: Immediately Refer to: Mark Taylor; [email protected]; (317) 276-5795 (Media) Kevin Hern; [email protected]; (317) 277-1838 (Investors) Lilly Reports Strong Fourth-Quarter and Full-Year 2020 Financial Results • Revenue in the fourth quarter of 2020 increased 22 percent, driven by volume growth of 24 percent. Excluding bamlanivimab revenue of $871 million, fourth-quarter 2020 revenue grew 7 percent. • Full-year 2020 revenue increased 10 percent, driven by volume growth of 15 percent. Excluding bamlanivimab, full-year 2020 revenue grew 6 percent, driven by volume growth of 11 percent. • Key growth products launched since 2014, consisting of Trulicity, Verzenio, Taltz, Tyvyt, Olumiant, Jardiance, Emgality, Cyramza, Retevmo, Baqsimi and Basaglar contributed nearly 12 percentage points of revenue growth and represented approximately 48 percent of total revenue in the fourth quarter of 2020, or 55 percent of total revenue excluding bamlanivimab. • Fourth-quarter 2020 operating expenses increased 3 percent, driven by higher research and development investments, including expenses of $265 million to develop COVID-19 therapies. • Notable pipeline events included Emergency Use Authorizations from the FDA for both bamlanivimab and baricitinib for the treatment of COVID-19, as well as positive data readouts for donanemab for Alzheimer's disease, tirzepatide for type 2 diabetes and LOXO-305 for cancer. • Fourth-quarter 2020 earnings per share (EPS) increased to $2.32 on a reported basis and $2.75 on a non- GAAP basis. Full year 2020 EPS decreased to $6.79 on a reported basis and increased to $7.93 on a non- GAAP basis. -

Predictive QSAR Tools to Aid in Early Process Development of Monoclonal Antibodies
Predictive QSAR tools to aid in early process development of monoclonal antibodies John Micael Andreas Karlberg Published work submitted to Newcastle University for the degree of Doctor of Philosophy in the School of Engineering November 2019 Abstract Monoclonal antibodies (mAbs) have become one of the fastest growing markets for diagnostic and therapeutic treatments over the last 30 years with a global sales revenue around $89 billion reported in 2017. A popular framework widely used in pharmaceutical industries for designing manufacturing processes for mAbs is Quality by Design (QbD) due to providing a structured and systematic approach in investigation and screening process parameters that might influence the product quality. However, due to the large number of product quality attributes (CQAs) and process parameters that exist in an mAb process platform, extensive investigation is needed to characterise their impact on the product quality which makes the process development costly and time consuming. There is thus an urgent need for methods and tools that can be used for early risk-based selection of critical product properties and process factors to reduce the number of potential factors that have to be investigated, thereby aiding in speeding up the process development and reduce costs. In this study, a framework for predictive model development based on Quantitative Structure- Activity Relationship (QSAR) modelling was developed to link structural features and properties of mAbs to Hydrophobic Interaction Chromatography (HIC) retention times and expressed mAb yield from HEK cells. Model development was based on a structured approach for incremental model refinement and evaluation that aided in increasing model performance until becoming acceptable in accordance to the OECD guidelines for QSAR models. -

Assessment of Overall Survival, Quality of Life, And
Supplementary Online Content Salas-Vega S, Iliopoulos O, Mossialos E. Assesment of overall survival, quality of life, and safety benefits associated with new cancer medicines [published online December 29, 2016]. JAMA Oncol. doi:10.1001/jamaoncol.2016.4166 eTable 1. Therapeutic profile of all cancer medicines approved by the FDA between 2003- 2013 eTable 2. Regulatory evidence in support of classification of drug clinical benefits eFigure 1. Number of cancer drugs that were evaluated by all three HTA agencies, sorted by magnitude of clinical benefits eTable 3. Interagency agreement–Krippendorff’s alpha coefficients eMethods This supplementary material has been provided by the authors to give readers additional information about their work. Online-Only Supplement © 2016 American Medical Association. All rights reserved. Downloaded From: https://jamanetwork.com/ on 09/25/2021 Clinical value of cancer medicines Contents eExhibits ......................................................................................................................................................... 3 eTable 1. Therapeutic profile of all cancer medicines approved by the FDA between 2003- 2013 (Summary of eTable 2) ................................................................................................................... 3 eTable 2. Regulatory evidence in support of classification of drug clinical benefits ....................... 6 eFigure 1. Number of cancer drugs that were evaluated by all three HTA agencies, sorted by magnitude of clinical benefits -

Drug Information Center Highlights of FDA Activities
Drug Information Center Highlights of FDA Activities – 3/1/21 – 3/31/21 FDA Drug Safety Communications & Drug Information Updates: Ivermectin Should Not Be Used to Treat or Prevent COVID‐19: MedWatch Update 3/5/21 The FDA advised consumers against the use of ivermectin for the treatment or prevention of COVID‐19 following reports of patients requiring medical support and hospitalization after self‐medicating. Ivermectin has not been approved for this use and is not an anti‐viral drug. Health professionals are encouraged to report adverse events associated with ivermectin to MedWatch. COVID‐19 EUA FAERS Public Dashboard 3/15/21 The FDA launched an update to the FDA Adverse Event Reporting System (FAERS) Public Dashboard that provides weekly updates of adverse event reports submitted to FAERS for drugs and therapeutic biologics used under an Emergency Use Authorization (EUA) during the COVID‐19 public health emergency. Monoclonal Antibody Products for COVID‐19 – Fact Sheets Updated to Address Variants 3/18/21 The FDA authorized revised fact sheets for health care providers to include susceptibility of SARS‐CoV‐2 variants to each of the monoclonal antibody products available through EUA for the treatment of COVID‐19 (bamlanivimab, bamlanivimab and etesevimab, and casirivimab and imdevimab). Abuse and Misuse of the Nasal Decongestant Propylhexedrine Causes Serious Harm 3/25/21 The FDA warned that abuse and misuse of the nasal decongestant propylhexedrine, sold OTC in nasal decongestant inhalers, has been increasingly associated with cardiovascular and mental health problems. The FDA has recommended product design changes to support safe use, such as modifications to preclude tampering and limits on the content within the device. -

Summary of Drug Limitations Mary C
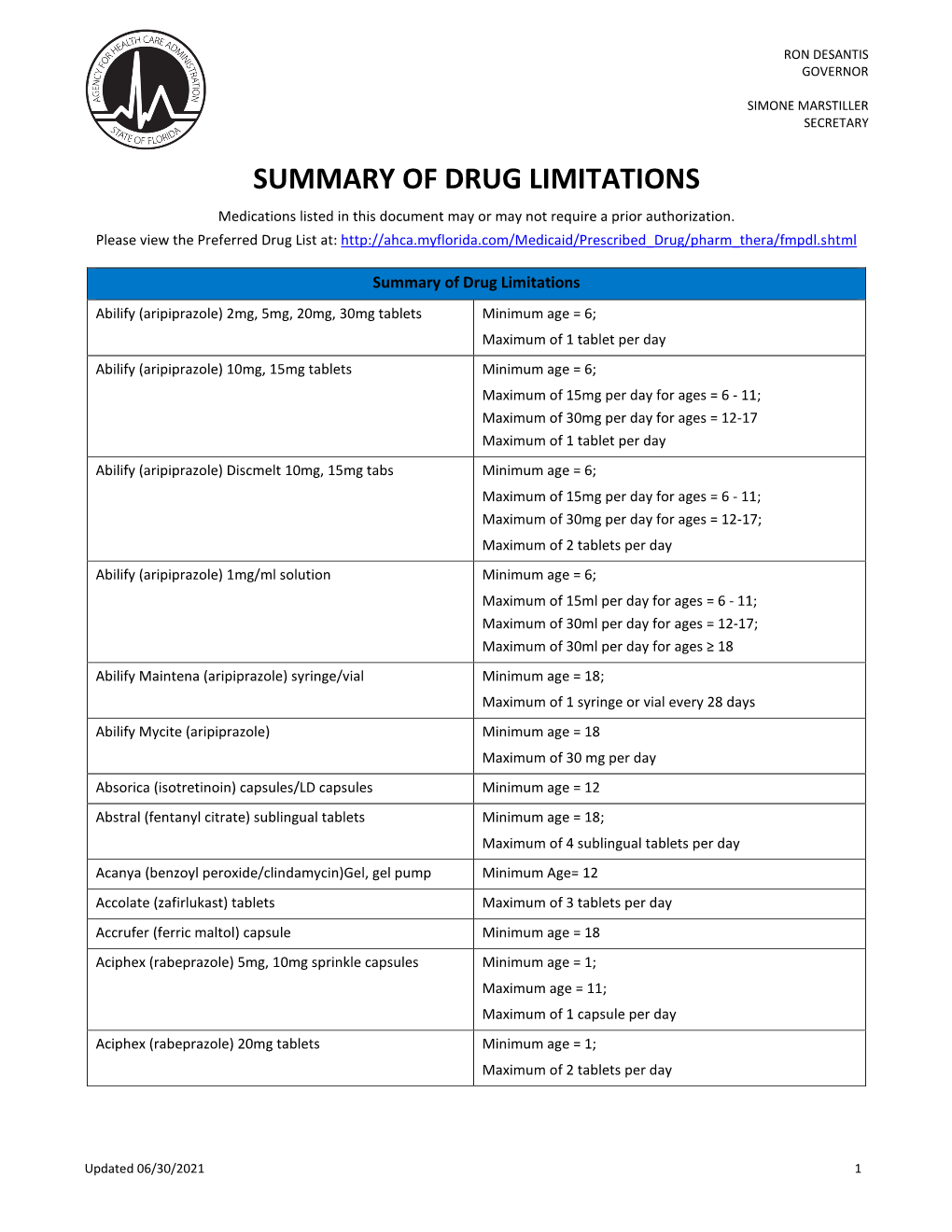
RON DESANTIS GOVERNOR SUMMARY OF DRUG LIMITATIONS MARY C. MAYHEW SECRETARY **Medications listed in this document may or may not require a prior authorization. Please view the Preferred Drug List at: http://ahca.myflorida.com/Medicaid/Prescribed_Drug/pharm_thera/fmpdl.shtml** Summary of Drug Limitations Abilify (aripiprazole) 2mg, 5mg, 20mg, 30mg tablets Minimum age = 6; Maximum of 1 tablet per day Abilify (aripiprazole) 10mg, 15mg tablets Minimum age = 6; Maximum of 15mg per day for ages = 6 - 11; Maximum of 30mg per day for ages = 12-17 Maximum of 1 tablet per day Abilify (aripiprazole) Discmelt 10mg, 15mg tabs Minimum age = 6; Maximum of 15mg per day for ages = 6 - 11; Maximum of 30mg per day for ages = 12-17; Maximum of 2 tablets per day Abilify (aripiprazole) 1mg/ml solution Minimum age = 6; Maximum of 15ml per day for ages = 6 - 11; Maximum of 30ml per day for ages = 12-17; Maximum of 30ml per day for ages =/> 18 Abilify Maintena (aripiprazole) syringe/vial Minimum age = 18; Maximum of 1 syringe or vial every 28 days Absorica (isotretinoin) 10mg, 20mg, 25mg,30mg, 35mg, & Minimum age = 12 40mg capsules Abstral (fentanyl citrate) sublingual tablets Minimum age = 18; Maximum of 4 sublingual tablets per day Acanya (benzoyl peroxide/clindamycin)Gel, gel pump Minimum Age= 12 Accolate (zafirlukast) tablets Maximum of 3 tablets per day Aciphex (rabeprazole) 5mg, 10mg sprinkle capsules Minimum age = 1; Maximum age = 11; Maximum of 1 capsule per day Aciphex (rabeprazole) 20mg tablets Minimum age = 1; Maximum of 2 tablets per day Actemra (tocilizumab) 80mg/4ml, 200mg/10ml, Minimum age= 2 400mg/20ml Vials, & 162mg/0.9ml Syringe Actimmune (Interferon Gamma-1b) Maximum of 6ml every 28days Actiq (fentanyl citrate) Lozenges Minimum age = 18; Maximum of 4 lozenges per day Activella (estradiol/norethindrone) tablets Minimum age = 18 Updated 02/28/2019 1 RON DESANTIS GOVERNOR SUMMARY OF DRUG LIMITATIONS MARY C. -

Performance of the Insulin-Only Ilet Bionic Pancreas and The
e118 Diabetes Care Volume 44, June 2021 Performance of the Insulin-Only Luz E. Castellanos,1 Courtney A. Balliro,1 Jordan S. Sherwood,1 Rabab Jafri,1 iLet Bionic Pancreas and the Mallory A. Hillard,1 Evelyn Greaux,1 Rajendranath Selagamsetty,2 Hui Zheng,3 Bihormonal iLet Using Firas H. El-Khatib,2 Edward R. Damiano,2,4 and Dasiglucagon in Adults With Type Steven J. Russell1 1 Diabetes in a Home-Use Setting Diabetes Care 2021;44:e118–e120 | https://doi.org/10.2337/dc20-1086 Reductions in blood glucose levels in with insulin lispro (Eli Lilly) or aspart (Table 1). The mean CGM glucose and people with diabetes are often achieved (Novo Nordisk), the bihormonal iLet for time in range (70–180 mg/dL) were 149 at the expense of increased hypoglyce- 7dayswithdasiglucagon(4mg/mL) ±13mg/dLand72±8%,respectively,in mia. A novel approach is to automati- and insulin lispro or aspart, or both, us- the insulin-only period, and 139 ± 11 cally deliver microdose glucagon when ing the same glucose target (110 mg/ mg/dL and 79 ± 9%, respectively, in the automation of insulin delivery alone is dL), in random order. There were no re- bihormonal period. The mean daily car- not sufficient to prevent hypoglycemia. strictions on diet or exercise. The prima- bohydrates consumed to prevent or The approach requires a bihormonal de- ry outcomes were prespecified iLet treat hypoglycemia were 16 ± 13 g and vice and a stable form of glucagon or operational thresholds. The key second- 18 ± 21 g in the insulin-only and bihor- glucagon analog. -

XERMELO™ (Telotristat Ethyl)
PHARMACY COVERAGE GUIDELINES ORIGINAL EFFECTIVE DATE: 5/18/2017 SECTION: DRUGS LAST REVIEW DATE: 5/20/2021 LAST CRITERIA REVISION DATE: 5/20/2021 ARCHIVE DATE: XERMELO™ (telotristat ethyl) Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy Coverage Guideline must be read in its entirety to determine coverage eligibility, if any. This Pharmacy Coverage Guideline provides information related to coverage determinations only and does not imply that a service or treatment is clinically appropriate or inappropriate. The provider and the member are responsible for all decisions regarding the appropriateness of care. Providers should provide BCBSAZ complete medical rationale when requesting any exceptions to these guidelines. The section identified as “Description” defines or describes a service, procedure, medical device or drug and is in no way intended as a statement of medical necessity and/or coverage. The section identified as “Criteria” defines criteria to determine whether a service, procedure, medical device or drug is considered medically necessary or experimental or investigational. State or federal mandates, e.g., FEP program, may dictate that any drug, device or biological product approved by the U.S. Food and Drug Administration (FDA) may not be considered experimental or investigational and thus the drug, device or biological product may be assessed only on the basis of medical necessity. Pharmacy Coverage Guidelines are subject to change as new information becomes available. For purposes of this Pharmacy Coverage Guideline, the terms "experimental" and "investigational" are considered to be interchangeable. BLUE CROSS®, BLUE SHIELD® and the Cross and Shield Symbols are registered service marks of the Blue Cross and Blue Shield Association, an association of independent Blue Cross and Blue Shield Plans. -

(CHMP) Agenda for the Meeting on 22-25 February 2021 Chair: Harald Enzmann – Vice-Chair: Bruno Sepodes
22 February 2021 EMA/CHMP/107904/2021 Human Medicines Division Committee for medicinal products for human use (CHMP) Agenda for the meeting on 22-25 February 2021 Chair: Harald Enzmann – Vice-Chair: Bruno Sepodes 22 February 2021, 09:00 – 19:30, room 1C 23 February 2021, 08:30 – 19:30, room 1C 24 February 2021, 08:30 – 19:30, room 1C 25 February 2021, 08:30 – 19:30, room 1C Disclaimers Some of the information contained in this agenda is considered commercially confidential or sensitive and therefore not disclosed. With regard to intended therapeutic indications or procedure scopes listed against products, it must be noted that these may not reflect the full wording proposed by applicants and may also vary during the course of the review. Additional details on some of these procedures will be published in the CHMP meeting highlights once the procedures are finalised and start of referrals will also be available. Of note, this agenda is a working document primarily designed for CHMP members and the work the Committee undertakes. Note on access to documents Some documents mentioned in the agenda cannot be released at present following a request for access to documents within the framework of Regulation (EC) No 1049/2001 as they are subject to on- going procedures for which a final decision has not yet been adopted. They will become public when adopted or considered public according to the principles stated in the Agency policy on access to documents (EMA/127362/2006). Official address Domenico Scarlattilaan 6 ● 1083 HS Amsterdam ● The Netherlands Address for visits and deliveries Refer to www.ema.europa.eu/how-to-find-us Send us a question Go to www.ema.europa.eu/contact Telephone +31 (0)88 781 6000 An agency of the European Union © European Medicines Agency, 2021.