New Jersey State Cancer Registry List of Reportable Diseases and Conditions Revised June 2018
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Gonadal (Testicular and Ovarian Tumors)
Gonadal (Testicular and Ovarian Tumors) Gonadal (Testicular and Ovarian Tumors) Authors: Ayda G. Nambayan, DSN, RN, St. Jude Children’s Research Hospital Erin Gafford, Pediatric Oncology Education Student, St. Jude Children’s Research Hospital; Nursing Student, School of Nursing, Union University Content Reviewed by: Guillermo L. Chantada, MD, Hospital JP Garrahan, Buenos Aires, Argentina Cure4Kids Release Date: 1 September 2006 At 4 weeks gestation, germ cells begin to develop in the yolk sac in an undifferentiated state. These primordial germ cells migrate to the gonadal ridge by the 6th week of gestation, and descend into the pelvis or scrotal sac.This migratory route explains the midline location of most extra-gonadal germ cell tumors (intracranial, mediastinal, retroperitoneal or sacrococcygeal). (A -1 ) Germ cell neoplasms arise either from the primordial germ cells (gonadal) or indirectly through embryonic or extra-embryonic differentiation (extra-gonadal). The stromal tumors arise from the primitive sex cords of either the ovary or the testicles, and the rare epithelial tumors arise from the coelomic epithelium that have undergone neoplastic transformations. Though the morphology of each type of germ cell tumor is similar in all locations (whether gonadal or extragonadal), the morphologic type and biological characteristics vary depending on the site of origin and age of the patient. There are three (A – 2) biologically distinct subsets of germ cell tumors: - tumors of the adolescent testis and ovary - extragonadal germ cell tumors of older children - tumors of infants and young children Testicular Germ Cell Tumors: Approximately 7% of all germ cell tumors are testicular and 75% of all (A – 3) testicular tumors have a germ cell origin. -

Heart Tumors in Domestic Animals
HEART TUMORS IN DOMESTIC ANIMALS Marko Hohšteter Department of veterinary pathology, Veterinary Faculty University of Zagreb Neoplasms of the heart are rare diseases in domestic animals. Among all domestic animals heart neoplasm are most common in dogs. Most of the canine heart tumors are primary what is contrary to other domestic animals, in which most of cardiac tumors are metastatic. Primary tumors of the heart represent 0,69% of the canine tumors. Among all primary neoplasms canine hemangiosarcoma of the right atrium is the most common. Other primary cardiac tumors in domestic animals include rhabdomyoma, rhabdomyosarcoma, myxoma, myxosarcoma, chondrosarcoma, osteosarcoma, granular cell tumor, fibroma, fibrosarcoma, lipoma, pericardial mesothelioma and undifferentiated sarcoma. Aortic and carotid body tumors are usually classified under primary heart neoplasm but are actually tumors which arise in adventitia or periarterial adipose tissue of the aorta, carotid artery or pulmonary artery, and can extend to heart base. Hemangiosarcoma is the most important and most frequent cardiac neoplasm of dogs. This tumor develops primary from the blood vessels that line the heart or can matastasize from sites such as spleen, skin or liver. It is most commonly reported in mid to large breeds, such as boxers, German shepherds, golden retrievers, and in older dogs (six years and older). Aortic and carotide body adenoma and adenocarcinoma belong into the group of chemoreceptor tumors („chemodectomas“) and are morphologicaly similar. In animals, incidence of aortic body neoplasm is higher than that of the carotide body. Both tumors mostly develop in dogs (brachyocephalic breed: boxers, Boston teriers), and are rare in cats and cattle. -

Acinic Cell Carcinoma with Extensive Neuroendocrine Differentiation: a Diagnostic Challenge
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by PubMed Central Head and Neck Pathol (2009) 3:163–168 DOI 10.1007/s12105-009-0114-5 CASE REPORT Acinic Cell Carcinoma with Extensive Neuroendocrine Differentiation: A Diagnostic Challenge Somak Roy Æ Kajal Kiran Dhingra Æ Parul Gupta Æ Nita Khurana Æ Bulbul Gupta Æ Ravi Meher Received: 30 January 2009 / Accepted: 11 March 2009 / Published online: 26 March 2009 Ó Humana 2009 Abstract Primary salivary gland carcinoma with neuro- Keywords Neuroendocrine Á Acinic cell Á Warthin’s Á endocrine differentiation is of rare occurrence, especially Chromogranin Á Carcinoma Á Parotid so in the parotid gland. Amongst the various reported pri- mary tumors with neuroendocrine differentiation, acinic cell carcinoma (ACC) one such tumor. A 48 year old lady Introduction presented with a gradually increasing right infra-auricular swelling for a period of 1 year which enlarged suddenly in Primary salivary gland carcinomas with neuroendocrine a short period. Contrast Enhanced Computed Tomography differentiation are rare accounting for 3.5% of all malig- (CECT) suggested diagnosis of Pleomorphic Adenoma. nant tumors and less than 1% of all carcinomas of parotid Fine Needle Aspiration Cytology (FANC) yielded a cystic gland [1]. Nicod reported the first case of carcinoid tumor fluid suggesting a possibility of Warthin’s tumor or of the parotid gland in a 51 year old lady [2]. Following Oncocytic lesion. Intraoperative findings were suggestive this there have been occasional reports of round cell tumors of a Warthin’s tumor. Initial histopathological examination of the parotid gland and minor salivary glands with very of the tumor was suggestive of neuroendocrine carcinoma. -

CANINE INSULINOMA: DIAGNOSIS, TREATMENT, & STAGING Eliza Reiss Grant, DVM, and Kristine E
Peer Reviewed PRACTICAL ONCOLOGY CANINE INSULINOMA: DIAGNOSIS, TREATMENT, & STAGING Eliza Reiss Grant, DVM, and Kristine E. Burgess, DVM, Diplomate ACVIM (Oncology) Tufts University An insulinoma is a malignant pancreatic tumor that DIAGNOSIS inappropriately secretes excessive insulin, resulting in Aside from a histologic confirmation of insulinoma, profound hypoglycemia.1 no currently available diagnostic test provides a de- Pancreatic tumors are classified as: finitive diagnosis of insulinoma. Existing techniques • Exocrine, which includes adenocarcinomas of may help increase suspicion for an insulin-secreting ductular or acinar origin tumor but, with most diagnostic testing, it is im- • Endocrine, which arise from the islets of perative to interpret all results in the context of the Langerhans. coexisting clinical signs. Insulinomas are functional neuroendocrine tumors that originate in the beta cells of the islets Differential Diagnosis of Langerhans.1 A complete work-up, including careful patient history, physical examination, bloodwork, and PRESENTATION diagnostic imaging tests, should be performed to Signalment rule out other causes of hypoglycemia, such as Any breed of dog can be affected, but large sepsis, hepatic failure, adrenal cortical insufficiency, breeds tend to be overrepresented.1 While, in toxin ingestion, and other forms of neoplasia. humans, insulinomas affect females far more frequently than males, there is no apparent sex Laboratory Tests predilection in dogs.1-3 Dogs also commonly Blood Glucose present with a malignant variant, while humans A simple fasting blood glucose level of less than often have a benign adenoma (80%).1 Insulino- 40 mg/dL can suggest hyperinsulinemia, although ma is rare in cats.4 careful monitoring of a fasted dog with suspected insulinoma is strongly recommended due to high Clinical Signs risk for seizure activity. -

Endocrine Tumors of the Pancreas
Friday, November 4, 2005 8:30 - 10:30 a. m. Pancreatic Tumors, Session 2 Chairman: R. Jensen, Bethesda, MD, USA 9:00 - 9:30 a. m. Working Group Session Pathology and Genetics Group leaders: J.–Y. Scoazec, Lyon, France Questions to be answered: 12 Medicine and Clinical Pathology Group leader: K. Öberg, Uppsala, Sweden Questions to be answered: 17 Surgery Group leader: B. Niederle, Vienna, Austria Questions to be answered: 11 Imaging Group leaders: S. Pauwels, Brussels, Belgium; D.J. Kwekkeboom, Rotterdam, The Netherlands Questions to be answered: 4 Color Codes Pathology and Genetics Medicine and Clinical Pathology Surgery Imaging ENETS Guidelines Neuroendocrinology 2004;80:394–424 Endocrine Tumors of the Pancreas - gastrinoma Epidemiology The incidence of clinically detected tumours has been reported to be 4-12 per million inhabitants, which is much lower than what is reported from autopsy series (about 1%) (5,13). Clinicopathological staging (12, 14, 15) Well-differentiated tumours are the large majority of which the two largest fractions are insulinomas (about 40% of cases) and non-functioning tumours (30-35%). When confined to the pancreas, non-angioinvasive, <2 cm in size, with <2 mitoses per 10 high power field (HPF) and <2% Ki-67 proliferation index are classified as of benign behaviour (WHO group 1) and, with the notable exception of insulinomas, are non-functioning. Tumours confined to the pancreas but > 2 cm in size, with angioinvasion and /or perineural space invasion, or >2mitoses >2cm in size, >2 mitoses per 20 HPF or >2% Ki-67 proliferation index, either non-functioning or functioning (gastrinoma, insulinoma, glucagonoma, somastatinoma or with ectopic syndromes, such as Cushing’s syndrome (ectopic ACTH syndrome), hypercaliemia (PTHrpoma) or acromegaly (GHRHoma)) still belong to the (WHO group 1) but are classified as tumours with uncertain behaviour. -

PROPOSED REGULATION of the STATE BOARD of HEALTH LCB File No. R057-16
PROPOSED REGULATION OF THE STATE BOARD OF HEALTH LCB File No. R057-16 Section 1. Chapter 457 of NAC is hereby amended by adding thereto the following provision: 1. The Division may impose an administrative penalty of $5,000 against any person or organization who is responsible for reporting information on cancer who violates the provisions of NRS 457. 230 and 457.250. 2. The Division shall give notice in the manner set forth in NAC 439.345 before imposing any administrative penalty 3. Any person or organization upon whom the Division imposes an administrative penalty pursuant to this section may appeal the action pursuant to the procedures set forth in NAC 439.300 to 439. 395, inclusive. Section 2. NAC 457.010 is here by amended to read as follows: As used in NAC 457.010 to 457.150, inclusive, unless the context otherwise requires: 1. “Cancer” has the meaning ascribed to it in NRS 457.020. 2. “Division” means the Division of Public and Behavioral Health of the Department of Health and Human Services. 3. “Health care facility” has the meaning ascribed to it in NRS 457.020. 4. “[Malignant neoplasm” means a virulent or potentially virulent tumor, regardless of the tissue of origin. [4] “Medical laboratory” has the meaning ascribed to it in NRS 652.060. 5. “Neoplasm” means a virulent or potentially virulent tumor, regardless of the tissue of origin. 6. “[Physician] Provider of health care” means a [physician] provider of health care licensed pursuant to chapter [630 or 633] 629.031 of NRS. 7. “Registry” means the office in which the Chief Medical Officer conducts the program for reporting information on cancer and maintains records containing that information. -

The Health-Related Quality of Life of Sarcoma Patients and Survivors In
Cancers 2020, 12 S1 of S7 Supplementary Materials The Health-Related Quality of Life of Sarcoma Patients and Survivors in Germany—Cross-Sectional Results of A Nationwide Observational Study (PROSa) Martin Eichler, Leopold Hentschel, Stephan Richter, Peter Hohenberger, Bernd Kasper, Dimosthenis Andreou, Daniel Pink, Jens Jakob, Susanne Singer, Robert Grützmann, Stephen Fung, Eva Wardelmann, Karin Arndt, Vitali Heidt, Christine Hofbauer, Marius Fried, Verena I. Gaidzik, Karl Verpoort, Marit Ahrens, Jürgen Weitz, Klaus-Dieter Schaser, Martin Bornhäuser, Jochen Schmitt, Markus K. Schuler and the PROSa study group Includes Entities We included sarcomas according to the following WHO classification. - Fletcher CDM, World Health Organization, International Agency for Research on Cancer, editors. WHO classification of tumours of soft tissue and bone. 4th ed. Lyon: IARC Press; 2013. 468 p. (World Health Organization classification of tumours). - Kurman RJ, International Agency for Research on Cancer, World Health Organization, editors. WHO classification of tumours of female reproductive organs. 4th ed. Lyon: International Agency for Research on Cancer; 2014. 307 p. (World Health Organization classification of tumours). - Humphrey PA, Moch H, Cubilla AL, Ulbright TM, Reuter VE. The 2016 WHO Classification of Tumours of the Urinary System and Male Genital Organs—Part B: Prostate and Bladder Tumours. Eur Urol. 2016 Jul;70(1):106–19. - World Health Organization, Swerdlow SH, International Agency for Research on Cancer, editors. WHO classification of tumours of haematopoietic and lymphoid tissues: [... reflects the views of a working group that convened for an Editorial and Consensus Conference at the International Agency for Research on Cancer (IARC), Lyon, October 25 - 27, 2007]. 4. ed. -

Klatskin Tumors and “Klatskin-Mimicking Lesions”: Our 22- Year Experience
Title: Klatskin tumors and “Klatskin-mimicking lesions”: our 22- year experience. Authors: Konstantinos Tsalis, Styliani Parpoudi, Dimitrios Kyziridis, Orestis Ioannidis, Natalia Antigoni Savvala, Nikolaos Antoniou, Savvas Symeonidis, Dimitrios Konstantaras, Ioannis Mantzoros, Manousos-Georgios Pramateftakis, Efstathios Kotidis, Stamatios Angelopoulos DOI: 10.17235/reed.2018.5749/2018 Link: PubMed (Epub ahead of print) Please cite this article as: Tsalis Konstantinos, Parpoudi Styliani, Kyziridis Dimitrios, Ioannidis Orestis, Savvala Natalia Antigoni , Antoniou Nikolaos , Symeonidis Savvas, Konstantaras Dimitrios , Mantzoros Ioannis, Pramateftakis Manousos-Georgios, Kotidis Efstathios, Angelopoulos Stamatios. Klatskin tumors and “Klatskin-mimicking lesions”: our 22-year experience. Rev Esp Enferm Dig 2018. doi: 10.17235/reed.2018.5749/2018. This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain. OR 5749 Klatskin tumors and “Klatskin-mimicking lesions”: our 22-year experience Konstantinos Tsalis, Styliani Parpoudi, Dimitrios Kyziridis, Orestis Ioannidis, Natalia Antigoni-Savvala, Nikolaos Antoniou, Savvas Symeonidis, Dimitrios Konstantaras, Ioannis Mantzoros, Pramateftakis Manousos-George, Kotidis Efstathios and Stamatios Angelopoulos Fourth Surgical Department. Medical School. Aristotle University of Thessaloniki. Thessaloniki, Greece. General Hospital “George Papanikoalou”. Thessaloniki, Greece Received: 04/06/2018 Accepted: 04/09/2018 Correspondence: Orestis Ioannidis. Fourth Surgical Department. Medical School. Aristotle University of Thessaloniki. Thessaloniki, Greece. General Hospital “G. -

Bilateral Giant Juvenile Fibroadenomas of Breasts: a Case Report
SAGE-Hindawi Access to Research Pathology Research International Volume 2011, Article ID 482046, 4 pages doi:10.4061/2011/482046 Case Report Bilateral Giant Juvenile Fibroadenomas of Breasts: A Case Report D. B. Nikumbh, S. R. Desai, P. S. Madan, N. J. Patil, and J. V. Wader Department of Pathology, Krishna Institute of Medical Sciences, Karad, District Satara, Maharashtra 415110, India Correspondence should be addressed to D. B. Nikumbh, drdhirajnikumbh@rediffmail.com Received 9 October 2010; Revised 4 April 2011; Accepted 7 April 2011 Academic Editor: Elizabeth Wiley Copyright © 2011 D. B. Nikumbh et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Juvenile fibroadenoma constitutes only 4% of the total fibroadenomas. The incidence of giant juvenile fibroadenomas is found to be only 0.5% of all the fibroadenomas. Bilateral giant juvenile fibroadenomas are extremely rare, and only four cases have been reported in the literature. Tothe best of our knowledge, we are presenting the fifth case of bilateral giant juvenile fibroadenomas in a 12-year-old prepubertal girl. The diagnosis was made on fine-needle aspiration cytology which was confirmed on histopathology. In this paper, we present this rare case to illustrate the diagnosis and management of this tumour and to emphasize that these tumours are almost always benign and should be treated with breast-conserving surgery to provide a healthy physical and social life to the patient. 1. Introduction both the breasts were seen, which were firm in consistency. -
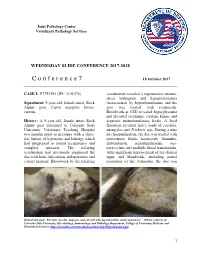
C O N F E R E N C E 7 18 October 2017
Joint Pathology Center Veterinary Pathology Services WEDNESDAY SLIDE CONFERENCE 2017-2018 C o n f e r e n c e 7 18 October 2017 CASE I: F1753191 (JPC 4101076). veterinarian revealed a regenerative anemia, stress leukogram and hypoproteinemia Signalment: 9-year-old, female intact, Rock characterized by hypoalbuminemia and the Alpine goat, Capra aegagrus hircus, goat was treated with ivermectin. caprine. Bloodwork at CSU revealed hyperglycemia and elevated creatinine, creatine kinase and History: A 9-year-old, female intact Rock aspartate aminotransferase levels. A fecal Alpine goat presented to Colorado State floatation revealed heavy loads of coccidia, University Veterinary Teaching Hospital strongyles and Trichuris spp. During a nine two months prior to necropsy with a three- day hospitalization, the doe was treated with day history of hyporexia and lethargy which intravenous fluids, kaopectate, thiamine, had progressed to lateral recumbency and fenbendazole, sulfadimethoxine, oxy- complete anorexia. The referring tetracycline and multiple blood transfusions. veterinarian had previously diagnosed the After significant improvement of her clinical doe with louse infestation, endoparasites and signs and bloodwork, including partial a heart murmur. Bloodwork by the referring resolution of the dermatitis, the doe was Haired skin goat. The skin was dry, alopecia, and covered with hyperkeratotic crusts and ulcers. (Photo courtesy of: Colorado State University, Microbiology, Immunology, and Pathology Department, College of Veterinary Medicine and Biomedical Sciences, http://csucvmbs.colostate.edu/academics/mip/Pages/default.aspx) 1 discharged. exfoliating epithelial crusts which were often tangled within scant remaining hairs. Two months later, the goat presented with a This lesion most severely affected the skin one month history of progressive scaling and over the epaxials, the ventral abdomen and ulceration over the withers, dew claws, and teats, coronary bands and dew claws. -

Life Expectancy and Incidence of Malignant Disease Iv
LIFE EXPECTANCY AND INCIDENCE OF MALIGNANT DISEASE IV. CARCINOMAOF THE GENITO-URINARYTRACT CLAUDE E. WELCH,' M.D., AND IRA T. NATHANSON,? MS., M.D. (Front the Collis P. Huntington Memorial Hospital of Harvard University, and the Pondville State Hospitul, Wre~ztham,Mass.) In previous communications the life expectancy of patients with cancer of the breast (I), oral cavity (2), and gastro-intestinal tract (3) has been discussed. In the present paper the life expectancy of patients with carci- noma of the genito-urinary tract will be considered. The discussion will include cancer of the vulva, vagina, cervix and fundus uteri, ovary, penis, testicle, prostate, bladder, and kidney. All cases of cancer of these organs admitted to the Collis P. Huntington Memorial and Pondville Hospitals in the years 1912-1933 have been reviewed personally. It must again be stressed that these hospitals are organized strictly for the care of cancer patients. All those with cancer that apply are admitted for treatment; many of them have only terminal care. Only those cases in which a definite history of the date of onset could not be determined or in which the diagnosis was uncertain have been omitted in the present study. In compiling statistics on age and sex incidence all cases entering the hospitals before Jan. 1, 1936, have been included. The method of calculation of the life expectancy curves was fully described in the first paper (1). No at- tempt to evaluate the number of five-year survivals has been made, since many of the patients did not receive their initial treatment in these hospitals. -

Soft Tissue Sarcoma Classifications
Soft Tissue Sarcoma Classifications Contents: 1. Introduction 2. Summary of SSCRG’s decisions 3. Issue by issue summary of discussions A: List of codes to be included as Soft Tissue Sarcomas B: Full list of codes discussed with decisions C: Sarcomas of neither bone nor soft tissue D: Classifications by other organisations 1. Introduction We live in an age when it is increasingly important to have ‘key facts’ and ‘headline messages’. The national registry for bone and soft tissue sarcoma want to be able to produce high level factsheets for the general public with statements such as ‘There are 2000 soft tissue sarcomas annually in England’ or ‘Survival for soft tissue sarcomas is (eg) 75%’ It is not possible to write factsheets and data briefings like this, without a shared understanding from the SSCRG about which sarcomas we wish to include in our headline statistics. The registry accepts that soft tissue sarcomas are a very complex and heterogeneous group of cancers which do not easily reduce to headline figures. We will still strive to collect all data from cancer registries about anything that is ‘like a sarcoma’. We will also produce focussed data briefings on sites such as dermatofibrosarcomas and Kaposi’s sarcomas – the aim is not to forget any sites we exclude! The majority of soft tissue sarcomas have proved fairly uncontroversial in discussions with individual members of the SSCRG, but there were 7 particular issues it was necessary to make a group decision on. This paper records the decisions made and the rationale behind these decisions. 2. Summary of SSCRG’s decisions: Include all tumours with morphology codes as listed in Appendix A for any cancer site except C40 and C41 (bone).