Midterm Survey Protocol
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Districts of Ethiopia
Region District or Woredas Zone Remarks Afar Region Argobba Special Woreda -- Independent district/woredas Afar Region Afambo Zone 1 (Awsi Rasu) Afar Region Asayita Zone 1 (Awsi Rasu) Afar Region Chifra Zone 1 (Awsi Rasu) Afar Region Dubti Zone 1 (Awsi Rasu) Afar Region Elidar Zone 1 (Awsi Rasu) Afar Region Kori Zone 1 (Awsi Rasu) Afar Region Mille Zone 1 (Awsi Rasu) Afar Region Abala Zone 2 (Kilbet Rasu) Afar Region Afdera Zone 2 (Kilbet Rasu) Afar Region Berhale Zone 2 (Kilbet Rasu) Afar Region Dallol Zone 2 (Kilbet Rasu) Afar Region Erebti Zone 2 (Kilbet Rasu) Afar Region Koneba Zone 2 (Kilbet Rasu) Afar Region Megale Zone 2 (Kilbet Rasu) Afar Region Amibara Zone 3 (Gabi Rasu) Afar Region Awash Fentale Zone 3 (Gabi Rasu) Afar Region Bure Mudaytu Zone 3 (Gabi Rasu) Afar Region Dulecha Zone 3 (Gabi Rasu) Afar Region Gewane Zone 3 (Gabi Rasu) Afar Region Aura Zone 4 (Fantena Rasu) Afar Region Ewa Zone 4 (Fantena Rasu) Afar Region Gulina Zone 4 (Fantena Rasu) Afar Region Teru Zone 4 (Fantena Rasu) Afar Region Yalo Zone 4 (Fantena Rasu) Afar Region Dalifage (formerly known as Artuma) Zone 5 (Hari Rasu) Afar Region Dewe Zone 5 (Hari Rasu) Afar Region Hadele Ele (formerly known as Fursi) Zone 5 (Hari Rasu) Afar Region Simurobi Gele'alo Zone 5 (Hari Rasu) Afar Region Telalak Zone 5 (Hari Rasu) Amhara Region Achefer -- Defunct district/woredas Amhara Region Angolalla Terana Asagirt -- Defunct district/woredas Amhara Region Artuma Fursina Jile -- Defunct district/woredas Amhara Region Banja -- Defunct district/woredas Amhara Region Belessa -- -

Challenges of Clinical Chemistry Analyzers Utilization in Public Hospital Laboratories of Selected Zones of Oromia Region, Ethiopia: a Mixed Methods Study
Research Article ISSN: 2574 -1241 DOI: 10.26717/BJSTR.2021.34.005584 Challenges of Clinical Chemistry Analyzers Utilization in Public Hospital Laboratories of Selected Zones of Oromia Region, Ethiopia: A Mixed Methods Study Rebuma Belete1*, Waqtola Cheneke2, Aklilu Getachew2 and Ahmedmenewer Abdu1 1Department of Medical Laboratory Sciences, College of Health and Medical Sciences, Haramaya University, Harar, Ethiopia 2School of Medical Laboratory Sciences, Faculty of Health Sciences, Institute of Health, Jimma University, Jimma, Ethiopia *Corresponding author: Rebuma Belete, Department of Medical Laboratory Sciences, College of Health and Medical Sciences, Haramaya University, Harar, Ethiopia ARTICLE INFO ABSTRACT Received: March 16, 2021 Background: The modern practice of clinical chemistry relies ever more heavily on automation technologies. Their utilization in clinical laboratories in developing countries Published: March 22, 2021 is greatly affected by many factors. Thus, this study was aimed to identify challenges affecting clinical chemistry analyzers utilization in public hospitals of selected zones of Oromia region, Ethiopia. Citation: Rebuma Belete, Waqtola Cheneke, Aklilu Getachew, Ahmedmenew- Methods: A cross-sectional study using quantitative and qualitative methods er Abdu. Challenges of Clinical Chemistry was conducted in 15 public hospitals from January 28 to March 15, 2019. Purposively Analyzers Utilization in Public Hospital selected 68 informants and 93 laboratory personnel working in clinical chemistry section Laboratories of Selected Zones of Oromia were included in the study. Data were collected by self-administered questionnaires, Region, Ethiopia: A Mixed Methods Study. in-depth interviews and observational checklist. The quantitative data were analyzed Biomed J Sci & Tech Res 34(4)-2021. by descriptive statistics using SPSS 25.0 whereas qualitative data was analyzed by a BJSTR. -
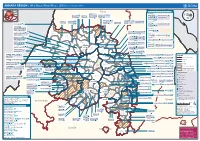
AMHARA REGION : Who Does What Where (3W) (As of 13 February 2013)
AMHARA REGION : Who Does What Where (3W) (as of 13 February 2013) Tigray Tigray Interventions/Projects at Woreda Level Afar Amhara ERCS: Lay Gayint: Beneshangul Gumu / Dire Dawa Plan Int.: Addis Ababa Hareri Save the fk Save the Save the df d/k/ CARE:f k Save the Children:f Gambela Save the Oromia Children: Children:f Children: Somali FHI: Welthungerhilfe: SNNPR j j Children:l lf/k / Oxfam GB:af ACF: ACF: Save the Save the af/k af/k Save the df Save the Save the Tach Gayint: Children:f Children: Children:fj Children:l Children: l FHI:l/k MSF Holand:f/ ! kj CARE: k Save the Children:f ! FHI:lf/k Oxfam GB: a Tselemt Save the Childrenf: j Addi Dessie Zuria: WVE: Arekay dlfk Tsegede ! Beyeda Concern:î l/ Mirab ! Concern:/ Welthungerhilfe:k Save the Children: Armacho f/k Debark Save the Children:fj Kelela: Welthungerhilfe: ! / Tach Abergele CRS: ak Save the Children:fj ! Armacho ! FHI: Save the l/k Save thef Dabat Janamora Legambo: Children:dfkj Children: ! Plan Int.:d/ j WVE: Concern: GOAL: Save the Children: dlfk Sahla k/ a / f ! ! Save the ! Lay Metema North Ziquala Children:fkj Armacho Wegera ACF: Save the Children: Tenta: ! k f Gonder ! Wag WVE: Plan Int.: / Concern: Save the dlfk Himra d k/ a WVE: ! Children: f Sekota GOAL: dlf Save the Children: Concern: Save the / ! Save: f/k Chilga ! a/ j East Children:f West ! Belesa FHI:l Save the Children:/ /k ! Gonder Belesa Dehana ! CRS: Welthungerhilfe:/ Dembia Zuria ! î Save thedf Gaz GOAL: Children: Quara ! / j CARE: WVE: Gibla ! l ! Save the Children: Welthungerhilfe: k d k/ Takusa dlfj k -

Ethiopia: West Guji – Gedeo Conflict Displacement Flash Update 2
Ethiopia: West Guji – Gedeo Conflict Displacement Flash Update 2 22 May 2018 Highlights • A rapid assessment conducted in Gedeo zone (SNNPR) found that at least 274,5481 people were displaced from West Guji (Oromia) to Gedeo zone following the violence that erupted along the regional boundary in mid-April. Some 84,000 people were also displaced in West Guji zone. More than 4,000 houses were reportedly burnt down or damaged in West Guji and livelihoods destroyed. • Official reports indicate that as of early May, 102,593 people of the 274,548 people displaced in Gedeo were returned to their villages in West Guji zone • The Government, the local community and civil society were the first and main responders to date, with sup- port from few partners. Significant gaps in food, shelter, NFI and WaSH are reported • Although there were no reported health outbreaks so far, AWD, scabies and measles are potential health risks due to the use of water from unsafe sources, open defecation, overcrowded shelter and sharing of clothes. The overcrowded shelter conditions within hosting households also present protection concerns. Dara Sidama Dila I. Displacement overview ! 12,176 452 Bore Chichu A rapid assessment conducted in Gedeo zone ! 3,772 (SNNPR) from 2 to 8 May found that at least Dila Zuria stite eturns 274,548 people (139,494 male; 135,104 female) Wenago einin ! were displaced from West Guji (Oromia) to Gedeo Bule isceent 4,844 ! Koti ! zone, following the inter-communal violence that 8,198 Ilalcha ! erupted in mid-April 2018 along the borders of the Wenago Bule Abaya two zones. -

Grain Market Research Project
Grain Market Research Project PROMOTING FERTILIZER USE IN ETHIOPIA: THE IMPLICATIONS OF IMPROVING GRAIN MARKET PERFORMANCE, INPUT MARKET EFFICIENCY, AND FARM MANAGEMENT Mulat Demeke Ali Said T.S. Jayne WORKING PAPER 5 GRAIN MARKET RESEARCH PROJECT MINISTRY OF ECONOMIC DEVELOPMENT AND COOPERATION ADDIS ABABA MARCH 1997 PROMOTING FERTILIZER USE IN ETHIOPIA: THE IMPLICATIONS OF IMPROVING GRAIN MARKET PERFORMANCE, INPUT MARKET EFFICIENCY, AND FARM MANAGEMENT MULAT DEMEKE ALI SAID T.S. JAYNE MARCH 1997 This is a revised and expanded version of a paper presented at the Grain Market Research Project Discussion Forum, November 8-9, 1996, Sodere, Ethiopia, sponsored by the Ministry of Economic Development and Cooperation, Government of Ethiopia. Mulat Demeke is Lecturer, Addis Ababa University, Ali Said is Research Scholar, Ministry of Economic Development and Cooperation; and T.S. Jayne is Visiting Associate Professor, Michigan State University. The authors thank Aklu Girgre, Daniel Molla, Asres Workneh, Steven Franzel, Valerie Kelly, and Jim Shaffer for comments on a previous draft. TABLE OF CONTENTS 1. BACKGROUND ...................................................... 1 2. THE PROFITABILITY OF FERTILIZER USE .............................. 7 2.1. Factors Influencing Fertilizer Use .................................. 7 2.2. Measuring the Profitability of Fertilizer .............................. 7 (a) The value-cost ratio (VCR)................................ 8 (b) The reservation price of fertilizer........................... 10 3. THE EFFECTS OF IMPROVING FERTILIZER MARKET .................... 14 3.1. Implications for Fertilizer Prices .................................. 14 3.2. The Impact on Fertilizer Profitability ............................... 21 4. THE IMPLICATIONS OF IMPROVING THE OUTPUT MARKET.............. 23 5. IMPROVING THE YIELD RESPONSE TO FERTILIZERS.................... 26 5.1. Constraints to Improved Yield Response ............................ 26 5.2. The Implications of Improving Output Response ...................... 31 5.3. -

Aalborg Universitet Restructuring State and Society Ethnic
Aalborg Universitet Restructuring State and Society Ethnic Federalism in Ethiopia Balcha, Berhanu Publication date: 2007 Document Version Publisher's PDF, also known as Version of record Link to publication from Aalborg University Citation for published version (APA): Balcha, B. (2007). Restructuring State and Society: Ethnic Federalism in Ethiopia. SPIRIT. Spirit PhD Series No. 8 General rights Copyright and moral rights for the publications made accessible in the public portal are retained by the authors and/or other copyright owners and it is a condition of accessing publications that users recognise and abide by the legal requirements associated with these rights. ? Users may download and print one copy of any publication from the public portal for the purpose of private study or research. ? You may not further distribute the material or use it for any profit-making activity or commercial gain ? You may freely distribute the URL identifying the publication in the public portal ? Take down policy If you believe that this document breaches copyright please contact us at [email protected] providing details, and we will remove access to the work immediately and investigate your claim. Downloaded from vbn.aau.dk on: November 29, 2020 SPIRIT Doctoral Programme Aalborg University Kroghstraede 3-3.237 DK-9220 Aalborg East Phone: +45 9940 9810 Mail: [email protected] Restructuring State and Society: Ethnic Federalism in Ethiopia Berhanu Gutema Balcha SPIRIT PhD Series Thesis no. 8 ISSN: 1903-7783 © 2007 Berhanu Gutema Balcha Restructuring State and Society: Ethnic Federalism in Ethiopia SPIRIT – Doctoral Programme Aalborg University Denmark SPIRIT PhD Series Thesis no. -
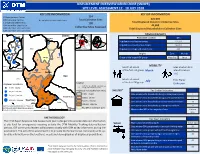
Displacement Overview Gedeo Zone (Snnpr)
DISPLACEMENT OVERVIEW GEDEO ZONE (SNNPR) SITE LEVEL ASSESSMENT 12 - 18 JULY 2018 KEY SITE INFORMATION KEY IDP INFORMATION 23 Spontaneous Camps 134 106 Collective Centres 4 Completely Inaccesible Sites Total Collective Sites 276,939 1 Dispersed Settlements 130 Total Displaced People In Collective Sites 19 Inaccesible Sites By Car 44,005 Collective Sites Assessed 123 Collective Sites with SMC Total Displaced Households In Collective Sites 127 Collective Sites with SMA Sidama Hadiya Arsi KTAlaba DEMOGRAPHICS Dila Town Sidama Hadiya ! Dila Town Wolayita West Arsi Population Location IDPs D!ila Zuria Sidama Abaya ÔÔ Bale Population in collective centres 217,971 Wenago Ô Gamo GofaGedio Bule Guji Population in spontaneous camps 58,518 ! Ô West Guji Abaya Yirgachefe Town Borena Liben Population in dispersed settlements 450 ! Dila Zuria ÔÔ Yirgachefe Ô Origins Zone Woreda Ô Ô ! Wenago Bule Ô Origin of the largest IDP group West Guji Kerca Ô Kochere ! Ô WGeestd eGbuji Ô Gelana MOBILITY Kercha Month of arrival Sites at which IDPs ÔÔ Yirgachefe Bule Hora Ô Ô Ô of the first IDP group March intend to return ÔÔ Yirgachefe Town Gedeo ÔÔ 116 Ô Ô Guji Ô Ô Gelana ÔÔ Ô Ô Month of arrival Time Frame Ô July ÔÔ Legend of the last IDP group Unknown Displaced individuals Ô Ô ÔKochere ÔÔ Collective sites (includes spontaneous ÔÔÔ Ô ÔÔ Ô ! 7,705 - 10,000 ÔÔÔ ÔÔ camps and collective centers) ÔÔ Ô Ô Displaced individuals (from Sites) SHELTER* Key Shelter Indicators ! 10,001 - 50,000 Ô Ô 7,705 - 10,000 Sites where >50% households living outside/open spaces 7 50,001 - 100,000 Ô Ô ! ÔÔÔÔ Ô ÔÔ ÔÔ ÔÔÔ Hambela Wamena ÔÔÔÔ Ô ÔÔÔ 10,001 - 50,000 Sites where >50% households living in permanent shelter 67 ! 100,001 - 129,629 West Guji Gedeb 50,001 - 100,000 Ô Kercha Sites where >50% households in below standard shelters 18 Ô This map is for illustration purposes only. -

English-Full (0.5
Enhancing the Role of Forestry in Building Climate Resilient Green Economy in Ethiopia Strategy for scaling up effective forest management practices in Amhara National Regional State with particular emphasis on smallholder plantations Wubalem Tadesse Alemu Gezahegne Teshome Tesema Bitew Shibabaw Berihun Tefera Habtemariam Kassa Center for International Forestry Research Ethiopia Office Addis Ababa October 2015 Copyright © Center for International Forestry Research, 2015 Cover photo by authors FOREWORD This regional strategy document for scaling up effective forest management practices in Amhara National Regional State, with particular emphasis on smallholder plantations, was produced as one of the outputs of a project entitled “Enhancing the Role of Forestry in Ethiopia’s Climate Resilient Green Economy”, and implemented between September 2013 and August 2015. CIFOR and our ministry actively collaborated in the planning and implementation of the project, which involved over 25 senior experts drawn from Federal ministries, regional bureaus, Federal and regional research institutes, and from Wondo Genet College of Forestry and Natural Resources and other universities. The senior experts were organised into five teams, which set out to identify effective forest management practices, and enabling conditions for scaling them up, with the aim of significantly enhancing the role of forests in building a climate resilient green economy in Ethiopia. The five forest management practices studied were: the establishment and management of area exclosures; the management of plantation forests; Participatory Forest Management (PFM); agroforestry (AF); and the management of dry forests and woodlands. Each team focused on only one of the five forest management practices, and concentrated its study in one regional state. -

Oromia Region Administrative Map(As of 27 March 2013)
ETHIOPIA: Oromia Region Administrative Map (as of 27 March 2013) Amhara Gundo Meskel ! Amuru Dera Kelo ! Agemsa BENISHANGUL ! Jangir Ibantu ! ! Filikilik Hidabu GUMUZ Kiremu ! ! Wara AMHARA Haro ! Obera Jarte Gosha Dire ! ! Abote ! Tsiyon Jars!o ! Ejere Limu Ayana ! Kiremu Alibo ! Jardega Hose Tulu Miki Haro ! ! Kokofe Ababo Mana Mendi ! Gebre ! Gida ! Guracha ! ! Degem AFAR ! Gelila SomHbo oro Abay ! ! Sibu Kiltu Kewo Kere ! Biriti Degem DIRE DAWA Ayana ! ! Fiche Benguwa Chomen Dobi Abuna Ali ! K! ara ! Kuyu Debre Tsige ! Toba Guduru Dedu ! Doro ! ! Achane G/Be!ret Minare Debre ! Mendida Shambu Daleti ! Libanos Weberi Abe Chulute! Jemo ! Abichuna Kombolcha West Limu Hor!o ! Meta Yaya Gota Dongoro Kombolcha Ginde Kachisi Lefo ! Muke Turi Melka Chinaksen ! Gne'a ! N!ejo Fincha!-a Kembolcha R!obi ! Adda Gulele Rafu Jarso ! ! ! Wuchale ! Nopa ! Beret Mekoda Muger ! ! Wellega Nejo ! Goro Kulubi ! ! Funyan Debeka Boji Shikute Berga Jida ! Kombolcha Kober Guto Guduru ! !Duber Water Kersa Haro Jarso ! ! Debra ! ! Bira Gudetu ! Bila Seyo Chobi Kembibit Gutu Che!lenko ! ! Welenkombi Gorfo ! ! Begi Jarso Dirmeji Gida Bila Jimma ! Ketket Mulo ! Kersa Maya Bila Gola ! ! ! Sheno ! Kobo Alem Kondole ! ! Bicho ! Deder Gursum Muklemi Hena Sibu ! Chancho Wenoda ! Mieso Doba Kurfa Maya Beg!i Deboko ! Rare Mida ! Goja Shino Inchini Sululta Aleltu Babile Jimma Mulo ! Meta Guliso Golo Sire Hunde! Deder Chele ! Tobi Lalo ! Mekenejo Bitile ! Kegn Aleltu ! Tulo ! Harawacha ! ! ! ! Rob G! obu Genete ! Ifata Jeldu Lafto Girawa ! Gawo Inango ! Sendafa Mieso Hirna -

World Journal of Engineering Research and Technology WJERT
wjert, 2018, Vol. 4, Issue 2, 126-167. Original Article ISSN 2454-695X Reta et al. World Journal of Engineering Research and Technology World Journal of Engineering Research and Technology WJERT www.wjert.org SJIF Impact Factor: 5.218 EXPERIMENTAL STUDY ON THE USE OF RECLAIMED ASPHALT PAVEMENT AS BASE COURSE MATERIALS THROUGH BLENDING WITH CRUSHED STONE AGGREGATES *Yomiyu Reta (MSc)1, Prof. Emer Tucay Quezon2 and Tarekegn Kumela (MSc)3 1Graduated MSc Degree in Highway Engineering at Jimma Institute of Technology, Jimma University, Jimma, Ethiopia. 2Professor, Department of Civil Engineering, Jimma Institute of Technology, Jimma University, and Affiliated with the Institute of Technology, Ambo University, Ambo, Ethiopia. 3Lecturer and Chairholder, Highway Engineering Stream, Jimma Institute of Technology, Jimma University, Jimma, Ethiopia. Article Received on 22/12/2017 Article Revised on 12/01/2018 Article Accepted on 02/02/2018 ABSTRACT *Corresponding Author Yomiyu Reta Overlay and maintenance resolve medium distress, but reconstruction MSc Degree in Highway may feasible and economical while Asphalt pavement are badly Engineering at Jimma deteriorated with time and traffic. This requires the removal of existing Institute of Technology, pavement surfaces. Recycling such construction waste has benefited Jimma University, Jimma, from economic to sustainability point of view and reduce the Ethiopia. exploitation of natural resources. The shortage of virgin aggregate supplies along with the increase in processing and hauling cost have encouraged the use of reclaimed material from the old structure as base course construction materials, and involved in regular practice in various countries around the world. Unfortunately, using Reclaimed asphalt pavement (RAP) is to take off in Ethiopia despite the current ambitions of road building program ongoing. -

Ethiopia: Amhara Region Administrative Map (As of 05 Jan 2015)
Ethiopia: Amhara region administrative map (as of 05 Jan 2015) ! ! ! ! ! ! ! ! ! ! Abrha jara ! Tselemt !Adi Arikay Town ! Addi Arekay ! Zarima Town !Kerakr ! ! T!IGRAY Tsegede ! ! Mirab Armacho Beyeda ! Debark ! Debarq Town ! Dil Yibza Town ! ! Weken Town Abergele Tach Armacho ! Sanja Town Mekane Berhan Town ! Dabat DabatTown ! Metema Town ! Janamora ! Masero Denb Town ! Sahla ! Kokit Town Gedebge Town SUDAN ! ! Wegera ! Genda Wuha Town Ziquala ! Amba Giorges Town Tsitsika Town ! ! ! ! Metema Lay ArmachoTikil Dingay Town ! Wag Himra North Gonder ! Sekota Sekota ! Shinfa Tomn Negade Bahr ! ! Gondar Chilga Aukel Ketema ! ! Ayimba Town East Belesa Seraba ! Hamusit ! ! West Belesa ! ! ARIBAYA TOWN Gonder Zuria ! Koladiba Town AMED WERK TOWN ! Dehana ! Dagoma ! Dembia Maksegnit ! Gwehala ! ! Chuahit Town ! ! ! Salya Town Gaz Gibla ! Infranz Gorgora Town ! ! Quara Gelegu Town Takusa Dalga Town ! ! Ebenat Kobo Town Adis Zemen Town Bugna ! ! ! Ambo Meda TownEbinat ! ! Yafiga Town Kobo ! Gidan Libo Kemkem ! Esey Debr Lake Tana Lalibela Town Gomenge ! Lasta ! Muja Town Robit ! ! ! Dengel Ber Gobye Town Shahura ! ! ! Wereta Town Kulmesk Town Alfa ! Amedber Town ! ! KUNIZILA TOWN ! Debre Tabor North Wollo ! Hara Town Fogera Lay Gayint Weldiya ! Farta ! Gasay! Town Meket ! Hamusit Ketrma ! ! Filahit Town Guba Lafto ! AFAR South Gonder Sal!i Town Nefas mewicha Town ! ! Fendiqa Town Zege Town Anibesema Jawi ! ! ! MersaTown Semen Achefer ! Arib Gebeya YISMALA TOWN ! Este Town Arb Gegeya Town Kon Town ! ! ! ! Wegel tena Town Habru ! Fendka Town Dera -

Administrative Region, Zone and Woreda Map of Oromia a M Tigray a Afar M H U Amhara a Uz N M
35°0'0"E 40°0'0"E Administrative Region, Zone and Woreda Map of Oromia A m Tigray A Afar m h u Amhara a uz N m Dera u N u u G " / m r B u l t Dire Dawa " r a e 0 g G n Hareri 0 ' r u u Addis Ababa ' n i H a 0 Gambela m s Somali 0 ° b a K Oromia Ü a I ° o A Hidabu 0 u Wara o r a n SNNPR 0 h a b s o a 1 u r Abote r z 1 d Jarte a Jarso a b s a b i m J i i L i b K Jardega e r L S u G i g n o G A a e m e r b r a u / K e t m uyu D b e n i u l u o Abay B M G i Ginde e a r n L e o e D l o Chomen e M K Beret a a Abe r s Chinaksen B H e t h Yaya Abichuna Gne'a r a c Nejo Dongoro t u Kombolcha a o Gulele R W Gudetu Kondole b Jimma Genete ru J u Adda a a Boji Dirmeji a d o Jida Goro Gutu i Jarso t Gu J o Kembibit b a g B d e Berga l Kersa Bila Seyo e i l t S d D e a i l u u r b Gursum G i e M Haro Maya B b u B o Boji Chekorsa a l d Lalo Asabi g Jimma Rare Mida M Aleltu a D G e e i o u e u Kurfa Chele t r i r Mieso m s Kegn r Gobu Seyo Ifata A f o F a S Ayira Guliso e Tulo b u S e G j a e i S n Gawo Kebe h i a r a Bako F o d G a l e i r y E l i Ambo i Chiro Zuria r Wayu e e e i l d Gaji Tibe d lm a a s Diga e Toke n Jimma Horo Zuria s e Dale Wabera n a w Tuka B Haru h e N Gimbichu t Kutaye e Yubdo W B Chwaka C a Goba Koricha a Leka a Gidami Boneya Boshe D M A Dale Sadi l Gemechis J I e Sayo Nole Dulecha lu k Nole Kaba i Tikur Alem o l D Lalo Kile Wama Hagalo o b r Yama Logi Welel Akaki a a a Enchini i Dawo ' b Meko n Gena e U Anchar a Midega Tola h a G Dabo a t t M Babile o Jimma Nunu c W e H l d m i K S i s a Kersana o f Hana Arjo D n Becho A o t