Maxart Early Access to ART for All. Implementation Study (2014-2018). Final Report
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

11010329.Pdf
THE RISE, CONSOLIDATION AND DISINTEGRATION OF DLAMINI POWER IN SWAZILAND BETWEEN 1820 AND 1889. A study in the relationship of foreign affairs to internal political development. Philip Lewis Bonner. ProQuest Number: 11010329 All rights reserved INFORMATION TO ALL USERS The quality of this reproduction is dependent upon the quality of the copy submitted. In the unlikely event that the author did not send a com plete manuscript and there are missing pages, these will be noted. Also, if material had to be removed, a note will indicate the deletion. uest ProQuest 11010329 Published by ProQuest LLC(2018). Copyright of the Dissertation is held by the Author. All rights reserved. This work is protected against unauthorized copying under Title 17, United States C ode Microform Edition © ProQuest LLC. ProQuest LLC. 789 East Eisenhower Parkway P.O. Box 1346 Ann Arbor, Ml 48106- 1346 ABSTRACT The Swazi kingdom grew out of the pressures associated with competition for trade and for the rich resources of Shiselweni. While centred on this area it acquired some of its characteristic features - notably a regimental system, and the dominance of a Dlamini aristocracy. Around 1815 the Swazi came under pressure from the South, and were forced to colonise the land lying north of the Lusutfu. Here they remained for some years a nation under arms, as they plundered local peoples, and were themselves swept about by the currents of the Mfecane. In time a more settled administration emerged, as the aristocracy spread out from the royal centres at Ezulwini, and this process accelerated under Mswati as he subdued recalcitrant chiefdoms, and restructured the regiments. -

Strengthening Community Systems. for HIV Treatment Scale-Up
Strengthening Community Systems. for HIV Treatment Scale-up. A case study on MaxART community. interventions in Swaziland. Colophon Strengthening Community Systems for HIV Treatment Scale-up A case study on MaxART community interventions in Swaziland Published: June 2015 Author: Françoise Jenniskens Photos: Adriaan Backer Design: de Handlangers For more information on the MaxART programme visit: www.stopaidsnow.org/treatment-prevention MINISTRY OF HEALTH KINGDOM OF SWAZILAND The Swaziland Ministry of Health, STOP AIDS NOW!, and the Clinton Health Access Initiative (CHAI) initiated the MaxART project in Swaziland. The programme partners include the Swaziland Network of People Living with HIV and AIDS (SWANNEPHA) and the Global Network of People Living with HIV (GNP+), the National Emergency Response Council on HIV/AIDS (NERCHA), national and international non-governmental organisations including the Southern Africa HIV & AIDS Information Dissemination Service (SAfAIDS), social scientists from the University of Amsterdam and researchers from the South African Centre for Epidemiological Modelling and Analysis (SACEMA). 2 Strengthening Community Systems for HIV Treatment Scale-up Acknowledgements Without the support of all the different partners in Swaziland it would not have been possible to draft this case study report. I would like to thank the respondents from the MoH and NERCHA for their extremely helpful insights in community systems strengthening issues in Swaziland and availing their time to talk to me within their busy time schedules. Furthermore I would like to express my gratitude to both Margareth Thwala-Tembe of SAfAIDS and Charlotte Lejeune of CHAI for their continuous support during my visit and for arranging all the appointments; dealing with logistics and providing transport for visiting the regions and key informants. -

2019/20 Annual Report
Vision: Vision: Partner Partner of choice of choice in alleviating in alleviating human human suffering suffering in Eswatini in Swaziland i Baphalali Eswatini Red Cross Society 2019/20 ANNUAL REPORT Mission: Saving lives, changing minds Mission: Saving lives, changing minds ii TABLE OF CONTENTS TABLE OF CONTENTS ............................................................................................................................... II PRESIDENT’S REMARKS ........................................................................................................................... 1 SECRETARY GENERAL’S SUMMARY ..................................................................................................... 4 INTRODUCTION .......................................................................................................................................... 5 ACHIEVEMENTS ......................................................................................................................................... 5 1.0 HEALTH AND SOCIAL SERVICES ............................................................................................... 5 1.1 PRIMARY HEALTH CARE: MOTHER, INFANT, CHILD HEALTH, CURATIVE, AND HIV/TB .. 5 2.0 FIRST AID ......................................................................................................................................... 9 3.0 DISASTER MANAGEMENT ................................................................................................................ 11 3.1 FIRE AND WINDSTORMS .................................................................................................................. -
Swaziland-VMMC-And-EIMC-Strategy
T ABLE OF C ONTENTS Table of Contents .........................................................................................................................................................................................i List of Tables ............................................................................................................................................................................................. iii List of Figures ............................................................................................................................................................................................ iii List of Boxes .............................................................................................................................................................................................. iii List of Acronyms ......................................................................................................................................................................................... iv Foreword ..................................................................................................................................................................................................... vi Acknowledgements.................................................................................................................................................................................... vii EXECUTIVE SUMMARY ...................................................................................................................................................................... -

Baphalali Swaziland Red Cross Society Clinics & Divisions Performance
BAPHALALI SWAZILAND RED CROSS SOCIETY CLINICS & DIVISIONS PERFORMANCE 2013 PREPARED BY: ELLIOT JELE PROGRAMMES MANAGER DATE: 8TH AUGUST, 2014 i TABLE OF CONTENTS TABLE OF CONTENTS ........................................................................................................................................ II 1. INTRODUCTION ............................................................................................................................................ 1 2. PROGRAMMES DESCRIPTION ....................................................................................................................... 2 3. ACHIEVEMENTS IN 2013 ............................................................................................................................... 2 3.1. HEALTH AND SOCIAL SERVICES ................................................................................................................. 2 3.1.1. GOAL- HEALTH & SOCIAL SERVICES ........................................................................................................ 2 3.1.2. OBJECTIVES - HEALTH & SOCIAL SERVICES .............................................................................................. 3 3.1.3. OVERALL HEALTH & SOCIAL SERVICES ACHIEVEMENTS .......................................................................... 3 3.1.4. ACHIEVEMENT PER PROGRAME COMPONENT, & OUTCOME LEVEL ....................................................... 3 ORPHANED AND VULNERABLE CHILDREN ....................................................................................................... -
2018 Annual Report
Vision: Vision: Partner Partner of choice of choice in alleviating in alleviating human human suffering suffering in Swaziland in Swaziland i Baphalali Eswatini Red Cross Society 2018 ANNUAL REPORT Baphalali demonstrates to a drought hit Lavumisa, Etjeni Chiefdom Community member on how to practice conservation agriculture (CA) using a seed driller. Photographer: BERCS Communications Department Mission: Saving lives, changing minds Mission: Saving lives, changing minds ii TABLE OF CONTENTS TABLE OF CONTENTS .................................................................................................................................... II PRESIDENT’S REMARKS ................................................................................................................................ 1 SECRETARY GENERAL’S SUMMARY ......................................................................................................... 4 INTRODUCTION ................................................................................................................................................ 5 ACHIEVEMENTS ............................................................................................................................................... 5 1.0 HEALTH AND SOCIAL SERVICES ................................................................................................... 5 1.1 PRIMARY HEALTH CARE: MOTHER, INFANT, CHILD HEALTH, CURATIVE, AND HIV/TB . 5 2.0 FIRST AID .............................................................................................................................................. -

UJOE Vol. 3 No 2 (DECEMBER, 2020) the IMPACT OF
UJOE Vol. 3 No 2 (DECEMBER, 2020) THE IMPACT OF NTFONJENI RURAL EDUCATION CENTRE’S ELECTRICAL INSTALLATION PROGRAMME ON PROMOTION OF SELF-RELIANCE AMONG GRADUATES Zandile Tsabedze* University of Eswatini Eswatini Nomazulu Ngozwana University of Eswatini . Eswatini David Jele University of Eswatini Eswatini ABSTRACT This study assessed the impact of Ntfonjeni Rural Education Centre’s (REC) electrical installation programme on promotion of self-reliance among out-of-school youth and adults in Eswatini, Hhohho Region. The objectives of the study were to: establish whether the electrical installation programme objectives were met, determine the electrical installation programme activities undertaken by graduates; and determine the engagement with learning by graduates in promoting self-reliance as a result of the electrical installation programme offered at Ntfonjeni REC. This was a small-scale study that used the evaluation research design with qualitative research methods. Data were collected using interviews, observation, and documents. Participants were graduates from the electrical installation programme, electrical installation instructor and community members that were chosen using convenient, purposive, and snowballing sampling techniques, respectively. Seventeen participants were individually interviewed using structured interviews. Data were analyzed qualitatively through thematic analysis. The findings revealed that the goal of the electrical installation programme of promoting self-reliance among its graduates was partially met. -

Delegation of the European Commission to Swaziland
This project is funded by the European Union Delegation of the European Commission to Swaziland Framework Contract Beneficiaries EuropeAid/119860/C/SV/multi Lot N° 2: Transport and Infrastructures Specific Contract No 2007/133128 Identification Mission for an Infrastructure Improvement Programme in the Sugar Sector in Swaziland Draft Final Report October 2007 The contents of this report is the sole responsibility of Parsons Brinckerhoff Consortium and can in no ways be taken to reflect the views of the European Union. This report is prepared solely for the use and benefit of the Contracting Authority. It is the result of an independent review, and neither Parsons Brinckerhoff Consortium, nor the authors accept or assume any responsibility or duty of care to any third party. ECORYS Nederland BV P.O. Box 4175 3006 AD Rotterdam Watermanweg 44 3067 GG Rotterdam The Netherlands T +31 (0)10 453 88 00 F +31 (0)10 453 07 68 E [email protected] W www.ecorys.com Registration no. 24316726 ECORYS Macro & Sector Policies T +31 (0)31 (0)10 453 87 53 F +31 (0)10 452 36 60 DaK/FG95509rap01 Table of contents List of Abbreviations 7 Executive Summary 9 Background 9 Needs Assessment 10 Project costing 11 Prioritization 11 Budgeting 11 Conclusions and Recommendations 12 1 Background 17 1.1 Country Information 17 1.2 European Union and Swaziland 18 2 Transport Infrastructure 21 2.1 Air Transport 21 2.2 Rail Transport 21 2.3 Roads Transport 22 2.4 Roads Department - Ministry of Public Works and Transport 23 3 Review of Government Development Policies -
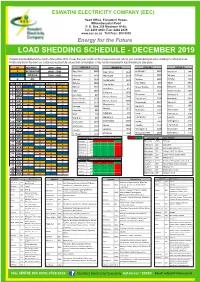
Load Shedding Schedule - December 2019
ESWATINI ELECTRICITY COMPANY (EEC) Head Office, Eluvatsini House, Mhlambanyatsi Road P. O. Box 258 Mbabane H100, Tel: 2409 4000, Fax: 2404 2335 www.eec.co.sz Toll Free: 800 9000 Energy for the Future LOAD SHEDDING SCHEDULE - DECEMBER 2019 Possible load shedding for the month of December 2019. Please find your location in the groups below and refer to your load shedding schedule detailing the affected areas. Kindly note that in the event our customers successfully reduce their consumption, it may not be necessary for load shedding to take place. M MORNING 10h00 - 14h00 GROUP A GROUP B GROUP C GROUP D A AFTERNOON 14h00 - 17h00 Pigg's Peak 3480 Pigg's Peak 3440 Endzingeni 3810 Mayiwane 3940 E EVENING 17h00 - 21h00 Mayiwane 3950 Mayiwane 3970 Sihhoye 2660 Sihhoye 2670 Nkhaba 3890 O OFF Sihhoye 2690 Dvokolwako 1320 Nkhaba 3860 Nkhaba 3880 Pine Valley 830 Mpisi 5640 DATE DAY GROUP A GROUP B GROUP C GROUP D Pine Valley 810 1 SUN E O M A Nkhaba 3870 Moses Hlophe 5350 Balegane 2610 Kent Rock 824 2 MON A E O M Mpisi 5650 Siteki 1230 Moses Hlophe 5360 3 TUE M A E O Balegane 2620 Kent Rock 827 Thompson 622 Siphocosini 925 4 WED O M A E Moses Hlophe 5340 5 THU E O M A Moses Hlophe 5330 Siphofaneni 5740 Riverbank 5090 Moses Hlophe 5380 6 FRI A E O M Moses Hlophe 5370 Thabankulu 3977 Manzini 1 508 7 SAT M A E O Magwabayi 542 KaLanga 1240 Big Bend 5014 Usutu 1093 8 SUN O M A E Mpaka 1227 9 MON E O M A Lobamba 950 Matsapha 2300 Sidvokodvo 630 10 TUE A E O M SPM 108 Edwaleni 104 Usutu 1094 Hlathikhulu 2180 11 WED M A E O Manzini 1 504 Sidvokodvo 636 Lawuba -

Impact Analysis of Smallholder Irrigation Schemes on Household Poverty Reduction in Swaziland: the Case of Ntfonjeni and Ngwempisi Rural Development Areas
IMPACT ANALYSIS OF SMALLHOLDER IRRIGATION SCHEMES ON HOUSEHOLD POVERTY REDUCTION IN SWAZILAND: THE CASE OF NTFONJENI AND NGWEMPISI RURAL DEVELOPMENT AREAS SITHOLE NOK’PHIWA LAMIE A THESES SUBMITTED TO THE GRADUATE SCHOOL IN PARTIAL FULFILMENT FOR THE REQUIREMENT OF MASTERS OF SCIENCE DEGREE IN AGRICULTURAL AND APPLIED ECONOMICS OF EGERTON UNIVERSITY EGERTON UNIVERSITY NOVEMBER, 2014 DECLARATION AND APPROVAL 1. Declaration This thesis is my original work and has not been submitted for an award of any degree in any other University. Sithole Nok’phiwa Lamie KM17/3372/12 __________ ______________ Signature Date 2. Approval This thesis has been submitted with our approval as Supervisors. Professor J.K. Lagat, PhD Associate Professor of Agricultural Economics Department of Agricultural Economics and Agribusiness Management, Egerton University, Kenya __________________ __________________ Signature Date Professor M. B. Masuku, PhD Head of Department, Agricultural Economics and Management, University of Swaziland _______________ ___________________ Signature Date i COPYRIGHT Copyright © 2014 Sithole Nok’phiwa Lamie No part of this thesis may be reproduced, stored, in any retrieval system or transmitted in any form or by any means, electronic, mechanical, photocopying, and recording without prior written permission of the author or Egerton University on that behalf. All rights Reserved ii DEDICATION To my dear mom Mrs. T.E. Sithole for her hard work, prayer, the role of a model and an inspiring Mother. My beloved Father, my brothers and sisters. iii ACKNOWLEDGEMENTS I give my sincere gratitude to Egerton University for allowing me to pursue Master of Science degree in Agricultural and Applied Economics, the German Academic Exchange Service – Deutscher Akadamischer Austauscdienst (DAAD) for providing me with a scholarship through the African Economic Research Consortium (AERC) / Collaborative Master of Science in Agricultural and Applied Economics (CMAAE) Programme. -

Swaziland Technology Needs Assessment Report 1
SWAZILAND TECHNOLOGY NEEDS ASSESSMENT REPORT 1 CLIMATE CHANGE ADAPTATION Revised Draft 15 June 2016 Prepared by Deepa Pullanikkatil (PhD), CANGO Table of Contents Chapter 1 Introduction ................................................................................................................................ 6 1.1 Background of TNA project ........................................................................................................................ 6 1.2 Existing national policies related to technological innovation, adaptation to climate change and development priorities ............................................................................................................................................. 7 1.3 Vulnerability assessments in the country .................................................................................................. 11 1.4 Sector selection ......................................................................................................................................... 14 1.4.1 An Overview of Expected Climate Change and its Impacts in Sectors Vulnerable to Climate Change ... 14 1.4.2 Process and results of sector selection .................................................................................................. 24 Chapter 2 Institutional arrangement for the TNA and the stakeholder involvement ................................. 26 2.1 National TNA team .................................................................................................................................. -

Swaziland Government Gazette Extraordinary
Swaziland Government Gazette Extraordinary VOL. XLVI] MBABANE, Friday, MAY 16th 2008 [No. 67 CONTENTS No. Page PART C - LEGAL NOTICE 104. Registration Centres For the 2008 General Elections................................................... SI PUBLISHED BY AUTHORITY 442 GENERAL NOTICE NO. 25 OF 2008 VOTERS REGISTRATION ORDER, 1992 (King’s Order in Council No.3 of 1992) REGISTRATION CENTRES FOR THE 2008 GENERAL ELECTIONS (Under Section 5(4)) Short title and commencement (1) This notice shall be cited as the Registration Centres Notice, 2008. (2) This general notice shall come into force on the date of publication in the Gazette. Registration centres for the 2008general elections It is notified for general information that the registration of all eligible voters for the 2008 general elections shall be held at Imiphakatsi (chiefdoms) and at the registration centres that have been listed in this notice; REGISTRATION CENTRES HHOHHO REGION CODE CODE CODE CHIEFDOM / POLLING Sub polling REGION INKHUNDLA STATION station 01 HHOHHO 01 HHUKWINI 01 Dlangeni 01 HHOHHO 01 HHUKWINI 02 Lamgabhi 01 HHOHHO 02 LOBAMBA 01 Elangeni 01 HHOHHO 02 LOBAMBA 02 Ezabeni 01 HHOHHO 02 LOBAMBA 03 Ezulwini 01 HHOHHO 02 LOBAMBA 04 Lobamba 01 HHOHHO 02 LOBAMBA 05 Nkhanini 01 HHOHHO 03 MADLANGEMPISI 01 Buhlebuyeza 01 HHOHHO 03 MADLANGEMPISI 02 KaGuquka 01 HHOHHO 03 MADLANGEMPISI 03 Kuphakameni/ Dvokolwako 01 HHOHHO 03 MADLANGEMPISI 04 Mzaceni 01 HHOHHO 03 MADLANGEMPISI 05 Nyonyane / KaMaguga 01 HHOHHO 03 MADLANGEMPISI 06 Zandondo 01 HHOHHO 04 MAPHALALENI 01 Edlozini 443