Cultural Responsiveness Framework
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Saskatchewan Discovery Guide
saskatchewan discovery guide OFFICIAL VACATION AND ACCOMMODATION PLANNER CONTENTS 1 Contents Welcome.........................................................................................................................2 Need More Information? ...........................................................................................4 Saskatchewan Tourism Zones..................................................................................5 How to Use the Guide................................................................................................6 Saskatchewan at a Glance ........................................................................................9 Discover History • Culture • Urban Playgrounds • Nature .............................12 Outdoor Adventure Operators...............................................................................22 Regina..................................................................................................................... 40 Southern Saskatchewan.................................................................................... 76 Saskatoon .............................................................................................................. 158 Central Saskatchewan ....................................................................................... 194 Northern Saskatchewan.................................................................................... 276 Events Guide.............................................................................................................333 -

An Indian Chief, an English Tourist, a Doctor, a Reverend, and a Member of Ppparliament: the Journeys of Pasqua’S’S’S Pictographs and the Meaning of Treaty Four
The Journeys of Pasqua’s Pictographs 109 AN INDIAN CHIEF, AN ENGLISH TOURIST, A DOCTOR, A REVEREND, AND A MEMBER OF PPPARLIAMENT: THE JOURNEYS OF PASQUA’S’S’S PICTOGRAPHS AND THE MEANING OF TREATY FOUR Bob Beal 7204 76 Street Edmonton, Alberta Canada, T6C 2J5 [email protected] Abstract / Résumé Indian treaties of western Canada are contentious among historians, First Nations, governments, and courts. The contemporary written docu- mentation about them has come from one side of the treaty process. Historians add information from such disciplines as First Nations Tradi- tional Knowledge and Oral History to draw as complete a picture as possible. Now, we have an additional source of written contemporary information, Chief Pasqua’s recently rediscovered pictographs showing the nature of Treaty Four and its initial implementation. Pasqua’s ac- count, as contextualized here, adds significantly to our knowledge of the western numbered treaty process. The pictographs give voice to Chief Pasqua’s knowledge. Les traités conclus avec les Indiens de l’Ouest canadien demeurent liti- gieux pour les historiens, les Premières nations, les gouvernements et les tribunaux. Les documents contemporains qui discutent des traités ne proviennent que d’une seule vision du processus des traités. Les historiens ajoutent des renseignements provenant de disciplines telles que les connaissances traditionnelles et l’histoire orale des Autochto- nes. Ils bénéficient désormais d’une nouvelle source écrite contempo- raine, les pictogrammes récemment redécouverts du chef Pasqua, qui illustrent la nature du Traité n° 4 et les débuts de son application. Le compte rendu du chef, tel que replacé dans son contexte, est un ajout important à notre connaissance du processus des traités numérotés dans l’Ouest canadien. -
In Saskatchewan
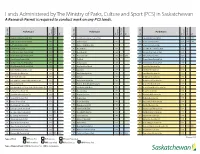
Lands Administered by The Ministry of Parks, Culture and Sport (PCS) in Saskatchewan A Research Permit is required to conduct work on any PCS lands. Park Name Park Name Park Name Type of Park Type Year Designated Amendment Year of Park Type Year Designated Amendment Year of Park Type Year Designated Amendment Year HP Cannington Manor Provincial Park 1986 NE Saskatchewan Landing Provincial Park 1973 RP Crooked Lake Provincial Park 1986 PAA 2018 HP Cumberland House Provincial Park 1986 PR Anderson Island 1975 RP Danielson Provincial Park 1971 PAA 2018 HP Fort Carlton Provincial Park 1986 PR Bakken - Wright Bison Drive 1974 RP Echo Valley Provincial Park 1960 HP Fort Pitt Provincial Park 1986 PR Besant Midden 1974 RP Great Blue Heron Provincial Park 2013 HP Last Mountain House Provincial Park 1986 PR Brockelbank Hill 1992 RP Katepwa Point Provincial Park 1931 HP St. Victor Petroglyphs Provincial Park 1986 PR Christopher Lake 2000 PAA 2018 RP Pike Lake Provincial Park 1960 HP Steele Narrows Provincial Park 1986 PR Fort Black 1974 RP Rowan’s Ravine Provincial Park 1960 HP Touchwood Hills Post Provincial Park 1986 PR Fort Livingstone 1986 RP The Battlefords Provincial Park 1960 HP Wood Mountain Post Provincial Park 1986 PR Glen Ewen Burial Mound 1974 RS Amisk Lake Recreation Site 1986 HS Buffalo Rubbing Stone Historic Site 1986 PR Grasslands 1994 RS Arm River Recreation Site 1966 HS Chimney Coulee Historic Site 1986 PR Gray Archaeological Site 1986 RS Armit River Recreation Site 1986 HS Fort Pelly #1 Historic Site 1986 PR Gull Lake 1974 RS Beatty -

Last Mountain-Touchwood
E-101 Form C The Election Act, 1996 Sections 34 and 138 SASKATCHEWAN Proclamation of the Returning Officer Declaring the Time and Place for the Nomination of Candidates and the Day of Opening the Polling Place Proclamation Constituency of Last Mountain-Touchwood Her Majesty’s Writ bearing the date September 29, 2020, having been directed to me, public notice is now given: 1. That I am commanded to cause an election, to be held according to law, of a member to serve in the Legislative Assembly of Saskatchewan for the above-mentioned constituency. 2. That I will, on October 10th, 2020, from 9:00 a.m. until 2:00 p.m. attend at 503 Main Street, Ituna, to receive nominations. 3. That in case voting of voters is required, polling places will be open on October 26, 2020, from 9:00 a.m. until 8:00 p.m. as follows: THEODORE 15 Poll Polling Place SEMANS RAYMORE 25 1, 2 Punnichy Community Hall 6 QUINTON 02 EDENWOLD EDGELEY 609 - 6th Avenue, Punnichy 35 PUNNICHY 27 MSDEN 640 MUSKOWEKWAN 310 85 3 George Gordon First Nation Arena 11 04 LESTOCK Last Mountain-Touchwood364 GOVAN 5 01 George Gordon First Nation 1020 GORDON 734 LEROSS 06 86 617 QU'APPELLE KELLIHER 26 4 Muskowekwan Band Hall ARLINGTON BEACH 1 10 1 03 15 ConstituencyMCLEAN 05 07 Muskowekwan First Nation 624 52 BALGONIE PILOT BUTTE 46 ST JOSEPH'S 5 Lestock Community Hall 731 322 Touchwood Hills Avenue, Lestock 35 08-09 731 ITUNA 25 DUVAL 731 HUBBARD 6 Kelliher School 6 205 2nd Avenue, Kelliher WEST OF THE SECOND MERIDIAN 24 07 STRASBOURG 11 10 08 7, 8, 9 Sacred Heart Parish Centre 27-28 731 -

2021 Saskatchewan Provincial Parks Guide
Saskatchewan SERVICES AT A GLANCE Boat Launch Boat Camping Seasonal Camping Camp-Easy Fishing Golfing Washrooms Showers Area Picnic Trails Online Reservations Provincial Parks NORTHERN Athabasca Sand Dunes * Bronson Forest * * * * * * * Guide Candle Lake * * * * * * * * * * Clarence-Steepbank Lakes * Clearwater River * * * * Cumberland House Fort Pitt * * * Great Blue Heron * * * * * * * * * * Lac La Ronge * * * * * * * * * Athabasca Makwa Lake * * * * * * * * * * Sand Dunes Meadow Lake * * * * * * * * * * Northern Narrow Hills * * * * * * * * * * Clearwater Steele Narrows * * * River Wildcat Hill * CENTRAL The Battlefords * * * * * * * * * * Blackstrap * * * * * * * * * Duck Mountain * * * * * * * * * * * Fort Carlton * * * * * La Ronge Good Spirit Lake * * * * * * * * * * * Lac La Ronge Meadow Greenwater Lake Lake * * * * * * * * * Clarence- Steepbank Pike Lake Lakes * * * * * * * * * * Cumberland Steele Narrows Narrow Porcupine Hills Hills House * * * * * Bronson Makwa Forest Lake SOUTHERN Great Blue Candle Lake Fort Pitt GreatHeron Blue Candle Lake Buffalo Pound * * * * * * * * * * Fort Pitt Heron The Cannington Manor Lloydminster Wildcat Hill * * Battlefords Prince Albert Melfort Fort Carlton Crooked Lake North * * * * * * * * * * * Battleford Greenwater Lake Cypress Hills * * * * * * * * * * Humboldt Central Duck Danielson * * * * * * * * * Saskatoon Mountain Pike Lake Good Pike Lake Spirit Douglas Blackstrap Touchwood SLakpirite * * * * * * * * * * Blackstrap HillsTouchwood Post Lake Hills Post Echo Valley Kindersley * * * * * -

Shopping in the Late Nineteenth Century: the Hudson’S Bay Company and Its Transition from the Fur Trade to Retailing
SHOPPING IN THE LATE NINETEENTH CENTURY: THE HUDSON’S BAY COMPANY AND ITS TRANSITION FROM THE FUR TRADE TO RETAILING A Thesis Submitted to the College of Graduate Studies and Research In Partial Fulfillment of the Requirements For the Degree of Master of Arts In the Department of Archaeology and Anthropology University of Saskatchewan Saskatoon By Jennifer Anne Schmidt ©Jennifer Schmidt, December, 2011. All rights reserved. Permission to Use In presenting this thesis in partial fulfilment of the requirements for a Postgraduate degree from the University of Saskatchewan, I agree that the Libraries of this University may make it freely available for inspection. I further agree that permission for copying of this thesis in any manner, in whole or in part, for scholarly purposes may be granted by the professor or professors who supervised my thesis work or, in their absence, by the Head of the Department or the Dean of the College in which my thesis work was done. It is understood that any copying, publication, or use of this thesis or parts thereof for financial gain shall not be allowed without my written permission. It is also understood that due recognition shall be given to me and to the University of Saskatchewan in any scholarly use which may be made of any material in my thesis. Requests for permission to copy or to make other use of material in this thesis in whole or part should be addressed to: Head of the Department of Archaeology and Anthropology University of Saskatchewan Saskatoon, Saskatchewan S7N 5B1 Canada i Abstract The South Battleford Project began in 1972 with salvage excavations in the historic town of Battleford, Saskatchewan. -

Muskowekwan Project Terms of Reference for the Environmental Impact Statement Table of Contents
Muskowekwan Project Terms of Reference for the Environmental Impact Statement July 2013 Prepared for: Saskatchewan Ministry of Environment, Environmental Assessment Branch, Regina, SK Prepared by: First Potash Ventures Muskowekwan Project Terms of Reference for the Environmental Impact Statement Table of Contents Table of Contents 1 INTRODUCTION ........................................................................................................................... 1-1 1.1 INTRODUCTION ........................................................................................................................... 1-1 1.2 BACKGROUND ABOUT THE MUSKOWEKWAN PROJECT ...................................................... 1-1 1.3 REGULATORY FRAMEWORK APPLICABLE TO THE ENVIRONMENTAL ASSESSMENT OF THE PROJECT ............................................................................................. 1-4 1.3.1 Provincial Environmental Assessment Requirements .................................................. 1-4 1.3.2 Federal Environmental Assessment Requirements ..................................................... 1-5 1.4 ORGANIZATION OF THE TERMS OF REFERENCE ................................................................. 1-6 2 SCOPE OF THE ASSESSMENT ................................................................................................. 2-1 2.1 SCOPE OF THE PROJECT ......................................................................................................... 2-1 2.2 FACTORS TO BE CONSIDERED IN THE EIS ........................................................................... -
A Teaching Guide to Saskatchewan Archaeology
A Teaching Guide to Saskatchewan Archaeology: Companion Document to Incorporating Archaeology into Lesson Plans: Educational Outcomes from the Saskatchewan Curriculum – Grades Four through Nine #1-1730 Quebec Avenue Saskatoon, SK CANADA S7K 1V9 Ph: (306) 664-4124 Fax: (306) 665-1928 [email protected] www.saskarchsoc.ca November 2010 Table of Contents Chapter 1: Archaeology in the Classroom...................................................................................1 1.1 What is Archaeology?......................................................................................................1 1.2 Incorporating Archaeology into the Saskatchewan Curriculum .......................................1 Chapter 2: Saskatchewan Archaeology ........................................................................................4 2.1 Introduction ....................................................................................................................4 2.2 First Nations Perspective ................................................................................................4 2.3 Archaeology Background Information ............................................................................4 2.3.1 Archaeology as a Discipline ...................................................................................2 2.3.2 Context ..................................................................................................................3 2.3.3 Archaeological Methods ........................................................................................5 -

2021 Saskatchewan Travel Guide
2021 SASKATCHEWAN TRAVEL GUIDE tourismsaskatchewan.com Stay open making new your own Grasslands National Park to discoveries in backyard. tourismsaskatchewan.com 2 CONTENTS Need More Information?........................2 Saskatchewan Tourism Areas ................3 Safe Travels ...............................................4 Southern Saskatchewan.........................5 Central Saskatchewan ..........................13 Northern Saskatchewan.......................19 Regina......................................................27 Saskatoon ...............................................31 Traveller Index........................................35 Saskatchewan at a Glance ...................41 Waskesiu Lake NEED MORE INFORMATION? Let our friendly travel counsellors help you plan your Saskatchewan FREE SASKATCHEWAN vacation. With one toll-free call or click of the mouse, you can receive TRAVEL RESOURCES travel information and trip planning assistance. Saskatchewan Fishing & Hunting Map Service is offered in Canada’s two official languages This colourful map offers – English and French. information about Saskatchewan’s great Le service est disponible dans les deux langues officielles du Canada – fishing and hunting opportunities. l'anglais et le français. CALL TOLL-FREE: 1-877-237-2273 Saskatchewan Official Road Map This fully detailed navigator is a handy tool for touring the province. IMPORTANT NUMBERS CALL 911 in an emergency Travellers experiencing a serious health-related situation, illness or injury should call 911 immediately. Available -

Saskatchewan Official Road
PRINCE ALBERT MELFORT MEADOW LAKE Population MEADOW LAKE PROVINCIAL PARK Population 35,926 Population 40 km 5,992 5,344 Prince Albert Visitor Information Centre Visitor Information 4 3700 - 2nd Avenue West Prince Albert National Park / Waskesieu Nipawin 142 km Northern Lights Palace Meadow Lake Tourist Information Centre Phone: 306-682-0094 La Ronge 88 km Choiceland and Hanson Lake Road Open seasonally 110 Mcleod Avenue W 79 km Hwy 4 and 9th Ave W GREEN LAKE 239 km 55 Phone: 306-752-7200 Phone: 306-236-4447 ve E 49 km Flin Flon t A Chamber of Commerce 6 RCMP 1s 425 km Open year-round 2nd Ave W 3700 - 2nd Avenue West t r S P.O. Phone: 306-764-6222 3 e iv M e R 5th Ave W r e Prince Albert . t Open year-round e l e n c f E v o W ru e t p 95 km r A 7th Ave W t S C S t y S d Airport 3 Km 9th Ave W H a 5 r w 3 Little Red 55 d ? R North Battleford T River Park a Meadow Lake C CANAM o Radio Stations: r HIGHWAY Lions Regional Park 208 km 15th St. N.W. 15th St. N.E. Veteran’s Way B McDonald Ave. C CJNS-Q98-FM e RCMP v 3 Mall r 55 . A e 3 e Meadow Lake h h v RCMP ek t St. t 5 km Northern 5 A Golf Club 8 AN P W Lights H ark . E Airport e e H Ave. -

George Gordon First Nations Women
GEORGE GORDON FIRST NATIONS WOMEN: PARTNERS IN SURVIVAL A Thesis Submitted to the College of Graduate and Postdoctoral Studies In Partial Fulfillment of the Requirements For the Degree of Doctor of Philosophy In the Program of Interdisciplinary Studies University of Saskatchewan Saskatoon By MIRIAM McNAB © Miriam McNab, December 2016. All rights reserved. PERMISSION TO USE In presenting this dissertation in partial fulfillment of the requirements for a Postgraduate degree from the University of Saskatchewan, I agree that the Libraries of this University may make it freely available for inspection. I further agree that permission for copying of this dissertation in any manner, in whole or in part, for scholarly purposes may be granted by the professor or professors who supervised my dissertation work or, in their absence, by the Head of the Department or the Dean of the College in which my thesis work was done. It is understood that any copying or publication or use of this dissertation or parts thereof for financial gain shall not be allowed without my written permission. It is also understood that due recognition shall be given to me and to the University of Saskatchewan in any scholarly use which may be made of any material in my dissertation. Requests for permission to copy or to make other uses of materials in this thesis/dissertation in whole or part should be addressed to: Head of the Program of Interdisciplinary Studies University of Saskatchewan 107 Administration Place Saskatoon, Saskatchewan S7N 5A2 Canada OR Dean College of Graduate Studies and Research University of Saskatchewan 107 Administration Place Saskatoon, Saskatchewan S7N 5A2 Canada i ABSTRACT This dissertation examines the work of the women of George Gordon First Nation in southern Saskatchewan from the earliest historical references until about the end of World War II. -
2019 Sctc 3 Date: 20190730
FILE NO.: SCT-5001-13 CITATION: 2019 SCTC 3 DATE: 20190730 SPECIFIC CLAIMS TRIBUNAL TRIBUNAL DES REVENDICATIONS PARTICULIÈRES BETWEEN: KAWACATOOSE FIRST NATION, PASQUA FIRST NATION, PIAPOT David Knoll, for the Claimants FIRST NATION, MUSCOWPETUNG FIRST NATION, GEORGE GORDON FIRST NATION, MUSKOWEKWAN FIRST NATION AND DAY STAR FIRST NATION Claimants – and – STAR BLANKET FIRST NATION Aaron B. Starr, Galen Richardson and Dusty Ernewein, for the Claimant Claimant – and – LITTLE BLACK BEAR FIRST NATION Ryan Lake, Aron Taylor and Aaron Christoff, for the Claimant Claimant – and – STANDING BUFFALO DAKOTA FIRST Mervin C. Phillips and Leane Phillips, for NATION the Claimant Claimant – and – PEEPEEKISIS FIRST NATION Michelle Brass and Tom Waller, for the Claimant Claimant – and – HER MAJESTY THE QUEEN IN RIGHT OF CANADA Lauri M. Miller and Donna Harris, for the As represented by the Minister of Indian Respondent Affairs and Northern Development Respondent HEARD: June 20-23, 2016, July 24-25, 2017, October 10-12, 2018 REASONS FOR DECISION Honourable W. L. Whalen 2 NOTE: This document is subject to editorial revision before its reproduction in final form. Cases Cited: Ross River Dena Council Band v Canada, 2002 SCC 54, 2002 CarswellYukon 58 (WL Can); Wewaykum Indian Band v Canada, 2002 SCC 79, [2002] 4 SCR 245; Williams Lake Indian Band v Canada (Aboriginal Affairs and Northern Development), 2018 SCC 4, 417 DLR (4th) 239; Lac La Ronge Indian Band v Canada, 2001 SKCA 109, 2001 CarswellSask 662 (WL Can); Canada (AG) v Anishnabe of Wauzhushk Onigum Band,