Mutations in Both SAMD9 and SLC19A2 Genes Caused Complex
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

WO 2014/135655 Al 12 September 2014 (12.09.2014) P O P C T
(12) INTERNATIONAL APPLICATION PUBLISHED UNDER THE PATENT COOPERATION TREATY (PCT) (19) World Intellectual Property Organization International Bureau (10) International Publication Number (43) International Publication Date WO 2014/135655 Al 12 September 2014 (12.09.2014) P O P C T (51) International Patent Classification: (81) Designated States (unless otherwise indicated, for every C12Q 1/68 (2006.01) kind of national protection available): AE, AG, AL, AM, AO, AT, AU, AZ, BA, BB, BG, BH, BN, BR, BW, BY, (21) International Application Number: BZ, CA, CH, CL, CN, CO, CR, CU, CZ, DE, DK, DM, PCT/EP2014/054384 DO, DZ, EC, EE, EG, ES, FI, GB, GD, GE, GH, GM, GT, (22) International Filing Date: HN, HR, HU, ID, IL, IN, IR, IS, JP, KE, KG, KN, KP, KR, 6 March 2014 (06.03.2014) KZ, LA, LC, LK, LR, LS, LT, LU, LY, MA, MD, ME, MG, MK, MN, MW, MX, MY, MZ, NA, NG, NI, NO, NZ, (25) Filing Language: English OM, PA, PE, PG, PH, PL, PT, QA, RO, RS, RU, RW, SA, (26) Publication Language: English SC, SD, SE, SG, SK, SL, SM, ST, SV, SY, TH, TJ, TM, TN, TR, TT, TZ, UA, UG, US, UZ, VC, VN, ZA, ZM, (30) Priority Data: ZW. 13305253.0 6 March 2013 (06.03.2013) EP (84) Designated States (unless otherwise indicated, for every (71) Applicants: INSTITUT CURIE [FR/FR]; 26 rue d'Ulm, kind of regional protection available): ARIPO (BW, GH, F-75248 Paris cedex 05 (FR). CENTRE NATIONAL DE GM, KE, LR, LS, MW, MZ, NA, RW, SD, SL, SZ, TZ, LA RECHERCHE SCIENTIFIQUE [FR/FR]; 3 rue UG, ZM, ZW), Eurasian (AM, AZ, BY, KG, KZ, RU, TJ, Michel Ange, F-75016 Paris (FR). -

SAMD9 and SAMD9L in Inherited Predisposition to Ataxia, Pancytopenia, and Myeloid Malignancies
Leukemia (2018) 32:1106–1115 https://doi.org/10.1038/s41375-018-0074-4 REVIEW ARTICLE Myelodysplastic syndrome SAMD9 and SAMD9L in inherited predisposition to ataxia, pancytopenia, and myeloid malignancies 1,2 3 1 2 4 5,6 Josef Davidsson ● Andreas Puschmann ● Ulf Tedgård ● David Bryder ● Lars Nilsson ● Jörg Cammenga Received: 17 October 2017 / Revised: 25 January 2018 / Accepted: 31 January 2018 / Published online: 25 February 2018 © The Author(s) 2018. This article is published with open access Abstract Germline mutations in the SAMD9 and SAMD9L genes, located in tandem on chromosome 7, are associated with a clinical spectrum of disorders including the MIRAGE syndrome, ataxia–pancytopenia syndrome and myelodysplasia and leukemia syndrome with monosomy 7 syndrome. Germline gain-of-function mutations increase SAMD9 or SAMD9L’s normal antiproliferative effect. This causes pancytopenia and generally restricted growth and/or specific organ hypoplasia in non- hematopoietic tissues. In blood cells, additional somatic aberrations that reverse the germline mutation’s effect, and give rise to the clonal expansion of cells with reduced or no antiproliferative effect of SAMD9 or SAMD9L include complete or partial chromosome 7 loss or loss-of-function mutations in SAMD9 or SAMD9L. Furthermore, the complete or partial loss of chromosome 7q may cause myelodysplastic syndrome in these patients. SAMD9 mutations appear to associate with a more 1234567890();,: severe disease phenotype, including intrauterine growth restriction, developmental delay and hypoplasia of adrenal glands, testes, ovaries or thymus, and most reported patients died in infancy or early childhood due to infections, anemia and/or hemorrhages. SAMD9L mutations have been reported in a few families with balance problems and nystagmus due to cerebellar atrophy, and may lead to similar hematological disease as seen in SAMD9 mutation carriers, from early childhood to adult years. -

Master Thesis
Mutagenic Interrogation of SAMD9 and SAMD9L Function Master Thesis For the attainment of the academic degree Master of Science From the University of Applied Sciences FH Campus Wien Submitted by: Tamara Szattler Personal identity code 1510544055 Supervisor: Yenan Bryceson Karolinska Institutet Stockholm Sweden Submitted on: 29.03.2018 1. Abstract in English Heterozygous gain - of - function m utations in SAMD9 and SAMD9L , two homologues on human chromosome 7, a re associated with severe clinical mani festations such as early onset bone marrow failure, cytopenia and monosomy 7 with high risk of progression to myelodysplastic syndrome (MDS) or acute myeloid leukemia (AML) . Additionally, biallelic SAMD9 mutations have been associated with normophosphatemi c tumoral calcinosis ( NFTC ) . SAMD9 and SAMD9L inhibit cell proliferation and are characterized as tumor suppressors. However, t he physiological function and regulation of SAMD9 and SAMD9L remains unclear . To identify the mechanisms through which mutated SA MD9/SAMD9L cause pathogenesis , it is instrumental to evaluate and characterize novel variants in functional assays. Additionally, targeting specific sites for mutagenesis and evaluate the effects on protein function can provide understanding of how individ ual domains in SAMD9/SAMD9L function . A ssessment of new variants requires a robust method . I have optimized a protocol for the evaluation of SAMD9/SAMD9L variants. In this context, I tested effects of several disease - associated as well as designed mutation s in SAMD9 and SAMD9L on cell proliferation and cell cycle progression. The presented data on SAMD9/SAMD9L variants associated with myeloid malignancies correlate with previous findings of others and suggest that these mutations enhance the function of the tumor suppressors . -

Downloaded Via Ensembl While Using HISAT2
viruses Article Interactions of Viral Proteins from Pathogenic and Low or Non-Pathogenic Orthohantaviruses with Human Type I Interferon Signaling Giulia Gallo 1,2, Grégory Caignard 3, Karine Badonnel 4, Guillaume Chevreux 5, Samuel Terrier 5, Agnieszka Szemiel 6, Gleyder Roman-Sosa 7,†, Florian Binder 8, Quan Gu 6, Ana Da Silva Filipe 6, Rainer G. Ulrich 8 , Alain Kohl 6, Damien Vitour 3 , Noël Tordo 1,9 and Myriam Ermonval 1,* 1 Unité des Stratégies Antivirales, Institut Pasteur, 75015 Paris, France; [email protected] (G.G.); [email protected] (N.T.) 2 Ecole Doctorale Complexité du Vivant, Sorbonne Université, 75006 Paris, France 3 UMR 1161 Virologie, Anses-INRAE-EnvA, 94700 Maisons-Alfort, France; [email protected] (G.C.); [email protected] (D.V.) 4 BREED, INRAE, Université Paris-Saclay, 78350 Jouy-en-Josas, France; [email protected] 5 Institut Jacques Monod, CNRS UMR 7592, ProteoSeine Mass Spectrometry Plateform, Université de Paris, 75013 Paris, France; [email protected] (G.C.); [email protected] (S.T.) 6 MRC-University of Glasgow Centre for Virus Research, Glasgow G61 1QH, UK; [email protected] (A.S.); [email protected] (Q.G.); ana.dasilvafi[email protected] (A.D.S.F.); [email protected] (A.K.) 7 Unité de Biologie Structurale, Institut Pasteur, 75015 Paris, France; [email protected] 8 Friedrich-Loeffler-Institut, Institute of Novel and Emerging Infectious Diseases, 17493 Greifswald-Insel Riems, Germany; binderfl[email protected] (F.B.); rainer.ulrich@fli.de (R.G.U.) Citation: Gallo, G.; Caignard, G.; 9 Institut Pasteur de Guinée, BP 4416 Conakry, Guinea Badonnel, K.; Chevreux, G.; Terrier, S.; * Correspondence: [email protected] Szemiel, A.; Roman-Sosa, G.; † Current address: Institut Für Virologie, Justus-Liebig-Universität, 35390 Giessen, Germany. -

Downloaded from Bioscientifica.Com at 09/30/2021 09:04:02PM Via Free Access
177:2 AUTHOR COPY ONLY N Amano and others Pediatric-onset adrenal 177:2 187–194 Clinical Study insufficiency Genetic defects in pediatric-onset adrenal insufficiency in Japan Naoko Amano1,2, Satoshi Narumi1,3, Mie Hayashi1, Masaki Takagi1,4, Kazuhide Imai5, Toshiro Nakamura6, Rumi Hachiya1,4, Goro Sasaki1,7, Keiko Homma8, Tomohiro Ishii1 and Tomonobu Hasegawa1 1Department of Pediatrics, Keio University School of Medicine, Tokyo, Japan, 2Department of Pediatrics, Tokyo Saiseikai Central Hospital, Tokyo, Japan, 3Department of Molecular Endocrinology, National Research Institute for Child Health and Development, Tokyo, Japan, 4Department of Endocrinology and Metabolism, Tokyo Metropolitan Children’s Medical Center, Tokyo, Japan, 5Department of Pediatrics, Nishibeppu National Hospital, Oita, Japan, Correspondence 6Department of Pediatrics, Kumamoto Chuo Hospital, Kumamoto, Japan, 7Department of Pediatrics, should be addressed Tokyo Dental College Ichikawa General Hospital, Chiba, Japan, and 8Clinical Laboratory, to T Hasegawa Keio University Hospital, Tokyo, Japan Email [email protected] Abstract Context: Most patients with pediatric-onset primary adrenal insufficiency (PAI), such as 21-hydroxylase deficiency, can be diagnosed by measuring the urine or serum levels of steroid metabolites. However, the etiology is often difficult to determine in a subset of patients lacking characteristic biochemical findings. Objective: To assess the frequency of genetic defects in Japanese children with biochemically uncharacterized PAI and characterize the phenotypes of mutation-carrying patients. Methods: We enrolled 63 Japanese children (59 families) with biochemically uncharacterized PAI, and sequenced 12 PAI-associated genes. The pathogenicities of rare variants were assessed based on in silico analyses and structural modeling. We calculated the proportion of mutation-carrying patients according to demographic characteristics. -

Somatic Mutations and Progressive Monosomy Modify SAMD9-Related Phenotypes in Humans
Downloaded from http://www.jci.org on June 26, 2017. https://doi.org/10.1172/JCI91913 RESEARCH ARTICLE The Journal of Clinical Investigation Somatic mutations and progressive monosomy modify SAMD9-related phenotypes in humans Federica Buonocore,1 Peter Kühnen,2 Jenifer P. Suntharalingham,1 Ignacio Del Valle,1 Martin Digweed,3 Harald Stachelscheid,4 Noushafarin Khajavi,2 Mohammed Didi,5 Angela F. Brady,6 Oliver Blankenstein,2 Annie M. Procter,7 Paul Dimitri,8 Jerry K.H. Wales,9 Paolo Ghirri,10 Dieter Knöbl,11 Brigitte Strahm,12 Miriam Erlacher,12,13 Marcin W. Wlodarski,12,13 Wei Chen,14 George K. Kokai,15 Glenn Anderson,16 Deborah Morrogh,17 Dale A. Moulding,18 Shane A. McKee,19 Charlotte M. Niemeyer,12,13 Annette Grüters,2 and John C. Achermann1 1Genetics and Genomic Medicine, University College London (UCL) Great Ormond Street Institute of Child Health, London, United Kingdom. 2Institute of Experimental Pediatric Endocrinology and Department of Pediatric Endocrinology, Charité, Berlin, Germany. 3Department of Human and Medical Genetics, Charité, Berlin, Germany. 4Berlin Institute of Health, Berlin, Germany, and Berlin-Brandenburg Centrum for Regenerative Therapies, Charité, Berlin, Germany. 5Department of Paediatric Endocrinology, Alder Hey Children’s NHS Foundation Trust, Liverpool, United Kingdom. 6North West Thames Regional Genetics Service, Northwick Park Hospital, Harrow, United Kingdom. 7Institute of Medical Genetics, University Hospital of Wales, Cardiff, United Kingdom. 8Academic Unit of Child Health, University of Sheffield, Sheffield, United Kingdom. 9Department of Endocrinology, Children’s Health Queensland Clinical Unit, University of Queensland, Brisbane, Australia. 10Department of Neonatology, University of Pisa, Pisa, Italy. 11Pediatric Endocrinology, Karlsruhe, Germany. -

Unique Genetic and Clinical Features of GATA2 Deficiency and SAMD9/ SAMD9L Syndromes
Best Practice & Research Clinical Haematology 33 (2020) 101197 Contents lists available at ScienceDirect Best Practice & Research Clinical Haematology journal homepage: www.elsevier.com/locate/issn/15216926 Germline predisposition in myeloid neoplasms: Unique genetic and clinical features of GATA2 deficiency and SAMD9/ SAMD9L syndromes Sushree S. Sahoo a, Emilia J. Kozyra b,c, Marcin W. Wlodarski a,b,* a Department of Hematology, St. Jude Children’s Research Hospital, Memphis, USA b Division of Pediatric Hematology and Oncology, Department of Pediatrics and Adolescent Medicine, Medical Center, Faculty of Medicine, University of Freiburg, Germany c Faculty of Biology, University of Freiburg, Freiburg, Germany ARTICLE INFO ABSTRACT Keywords: Increasing awareness about germline predisposition and the widespread application of unbiased Germline predisposition whole exome sequencing contributed to the discovery of new clinical entities with high risk for Hereditary MDS the development of haematopoietic malignancies. The revised 2016 WHO classification intro GATA2 duced a novel category of “myeloid neoplasms with germline predisposition” with GATA2, SAMD9 CEBPA, DDX41, RUNX1, ANKRD26 and ETV6 genes expanding the spectrum of hereditary SAMD9L myeloid neoplasms (MN). Since then, more germline causes of MN were identified, including SAMD9, SAMD9L, and ERCC6L2. This review describes the genetic and clinical spectrum of predisposition to MN. The main focus lies in delineation of phenotypes, genetics and management of GATA2 deficiency and the novel SAMD9/SAMD9L-related disorders. Combined, GATA2 and SAMD9/SAMD9L (SAMD9/9L) syndromes are recognized as most frequent causes of primary paediatric myelodysplastic syndromes, particularly in setting of monosomy 7. To date, ~550 cases with germline GATA2 mutations, and ~130 patients with SAMD9/9L mutations had been reported in literature. -
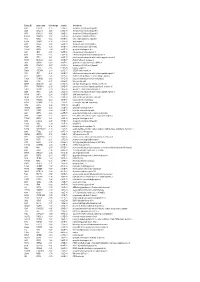
Entrez ID Gene Name Fold Change Q-Value Description
Entrez ID gene name fold change q-value description 4283 CXCL9 -7.25 5.28E-05 chemokine (C-X-C motif) ligand 9 3627 CXCL10 -6.88 6.58E-05 chemokine (C-X-C motif) ligand 10 6373 CXCL11 -5.65 3.69E-04 chemokine (C-X-C motif) ligand 11 405753 DUOXA2 -3.97 3.05E-06 dual oxidase maturation factor 2 4843 NOS2 -3.62 5.43E-03 nitric oxide synthase 2, inducible 50506 DUOX2 -3.24 5.01E-06 dual oxidase 2 6355 CCL8 -3.07 3.67E-03 chemokine (C-C motif) ligand 8 10964 IFI44L -3.06 4.43E-04 interferon-induced protein 44-like 115362 GBP5 -2.94 6.83E-04 guanylate binding protein 5 3620 IDO1 -2.91 5.65E-06 indoleamine 2,3-dioxygenase 1 8519 IFITM1 -2.67 5.65E-06 interferon induced transmembrane protein 1 3433 IFIT2 -2.61 2.28E-03 interferon-induced protein with tetratricopeptide repeats 2 54898 ELOVL2 -2.61 4.38E-07 ELOVL fatty acid elongase 2 2892 GRIA3 -2.60 3.06E-05 glutamate receptor, ionotropic, AMPA 3 6376 CX3CL1 -2.57 4.43E-04 chemokine (C-X3-C motif) ligand 1 7098 TLR3 -2.55 5.76E-06 toll-like receptor 3 79689 STEAP4 -2.50 8.35E-05 STEAP family member 4 3434 IFIT1 -2.48 2.64E-03 interferon-induced protein with tetratricopeptide repeats 1 4321 MMP12 -2.45 2.30E-04 matrix metallopeptidase 12 (macrophage elastase) 10826 FAXDC2 -2.42 5.01E-06 fatty acid hydroxylase domain containing 2 8626 TP63 -2.41 2.02E-05 tumor protein p63 64577 ALDH8A1 -2.41 6.05E-06 aldehyde dehydrogenase 8 family, member A1 8740 TNFSF14 -2.40 6.35E-05 tumor necrosis factor (ligand) superfamily, member 14 10417 SPON2 -2.39 2.46E-06 spondin 2, extracellular matrix protein 3437 -

Novel Biomarkers of Resistance of Pancreatic Cancer Cells to Oncolytic Vesicular Stomatitis Virus
www.impactjournals.com/oncotarget/ Oncotarget, Vol. 7, No. 38 Research Paper Novel biomarkers of resistance of pancreatic cancer cells to oncolytic vesicular stomatitis virus Eric Hastie1,*, Marcela Cataldi1,*, Megan J. Moerdyk-Schauwecker1,*, Sébastien A. Felt1,*, Nury Steuerwald2, Valery Z. Grdzelishvili1 1Department of Biological Sciences, University of North Carolina at Charlotte, Charlotte, NC, USA 2Cannon Research Center, Carolinas Healthcare System, Charlotte, NC, USA *These authors have contributed equally to this work Correspondence to: Valery Z. Grdzelishvili, email: [email protected] Keywords: pancreatic cancer, oncolytic virus, vesicular stomatitis virus, interferon-stimulated gene, biomarker of resistance Received: March 13, 2016 Accepted: July 27, 2016 Published: August 11, 2016 ABSTRACT Vesicular stomatitis virus (VSV) based recombinant viruses (such as VSV-ΔM51) are effective oncolytic viruses (OVs) against a majority of pancreatic ductal adenocarcinoma (PDAC) cell lines. However, some PDAC cell lines are highly resistant to VSV-ΔM51. We recently showed that treatment of VSV-resistant PDAC cells with ruxolitinib (JAK1/2 inhibitor) or TPCA-1 (IKK-β inhibitor) breaks their resistance to VSV-ΔM51. Here we compared the global effect of ruxolitinib or TPCA-1 treatment on cellular gene expression in PDAC cell lines highly resistant to VSV-ΔM51. Our study identified a distinct subset of 22 interferon-stimulated genes (ISGs) downregulated by both ruxolitinib and TPCA-1. Further RNA and protein analyses demonstrated that 4 of these genes (MX1, EPSTI1, XAF1, and GBP1) are constitutively co-expressed in VSV-resistant, but not in VSV-permissive PDACs, thus serving as potential biomarkers to predict OV therapy success. Moreover, shRNA-mediated knockdown of one of such ISG, MX1, showed a positive effect on VSV-ΔM51 replication in resistant PDAC cells, suggesting that at least some of the identified ISGs contribute to resistance of PDACs to VSV-ΔM51. -

Content Based Search in Gene Expression Databases and a Meta-Analysis of Host Responses to Infection
Content Based Search in Gene Expression Databases and a Meta-analysis of Host Responses to Infection A Thesis Submitted to the Faculty of Drexel University by Francis X. Bell in partial fulfillment of the requirements for the degree of Doctor of Philosophy November 2015 c Copyright 2015 Francis X. Bell. All Rights Reserved. ii Acknowledgments I would like to acknowledge and thank my advisor, Dr. Ahmet Sacan. Without his advice, support, and patience I would not have been able to accomplish all that I have. I would also like to thank my committee members and the Biomed Faculty that have guided me. I would like to give a special thanks for the members of the bioinformatics lab, in particular the members of the Sacan lab: Rehman Qureshi, Daisy Heng Yang, April Chunyu Zhao, and Yiqian Zhou. Thank you for creating a pleasant and friendly environment in the lab. I give the members of my family my sincerest gratitude for all that they have done for me. I cannot begin to repay my parents for their sacrifices. I am eternally grateful for everything they have done. The support of my sisters and their encouragement gave me the strength to persevere to the end. iii Table of Contents LIST OF TABLES.......................................................................... vii LIST OF FIGURES ........................................................................ xiv ABSTRACT ................................................................................ xvii 1. A BRIEF INTRODUCTION TO GENE EXPRESSION............................. 1 1.1 Central Dogma of Molecular Biology........................................... 1 1.1.1 Basic Transfers .......................................................... 1 1.1.2 Uncommon Transfers ................................................... 3 1.2 Gene Expression ................................................................. 4 1.2.1 Estimating Gene Expression ............................................ 4 1.2.2 DNA Microarrays ...................................................... -

Transcriptomic Response of Breast Cancer Cells to Anacardic Acid David J
www.nature.com/scientificreports OPEN Transcriptomic response of breast cancer cells to anacardic acid David J. Schultz1, Abirami Krishna2, Stephany L. Vittitow2, Negin Alizadeh-Rad2, Penn Muluhngwi2, Eric C. Rouchka 3 & Carolyn M. Klinge 2 Received: 5 December 2017 Anacardic acid (AnAc), a potential dietary agent for preventing and treating breast cancer, inhibited Accepted: 10 May 2018 the proliferation of estrogen receptor α (ERα) positive MCF-7 and MDA-MB-231 triple negative Published: xx xx xxxx breast cancer cells. To characterize potential regulators of AnAc action, MCF-7 and MDA-MB-231 cells were treated for 6 h with purifed AnAc 24:1n5 congener followed by next generation transcriptomic sequencing (RNA-seq) and network analysis. We reported that AnAc-diferentially regulated miRNA transcriptomes in each cell line and now identify AnAc-regulated changes in mRNA and lncRNA transcript expression. In MCF-7 cells, 80 AnAc-responsive genes were identifed, including lncRNA MIR22HG. More AnAc-responsive genes (886) were identifed in MDA-MB-231 cells. Only six genes were commonly altered by AnAc in both cell lines: SCD, INSIG1, and TGM2 were decreased and PDK4, GPR176, and ZBT20 were increased. Modeling of AnAc-induced gene changes suggests that AnAc inhibits monounsaturated fatty acid biosynthesis in both cell lines and increases endoplasmic reticulum stress in MDA-MB-231 cells. Since modeling of downregulated genes implicated NFκB in MCF-7, we confrmed that AnAc inhibited TNFα-induced NFκB reporter activity in MCF-7 cells. These data identify new targets and pathways that may account for AnAc’s anti-proliferative and pro-apoptotic activity. -

Transcriptional Profile of Human Anti-Inflamatory Macrophages Under Homeostatic, Activating and Pathological Conditions
UNIVERSIDAD COMPLUTENSE DE MADRID FACULTAD DE CIENCIAS QUÍMICAS Departamento de Bioquímica y Biología Molecular I TESIS DOCTORAL Transcriptional profile of human anti-inflamatory macrophages under homeostatic, activating and pathological conditions Perfil transcripcional de macrófagos antiinflamatorios humanos en condiciones de homeostasis, activación y patológicas MEMORIA PARA OPTAR AL GRADO DE DOCTOR PRESENTADA POR Víctor Delgado Cuevas Directores María Marta Escribese Alonso Ángel Luís Corbí López Madrid, 2017 © Víctor Delgado Cuevas, 2016 Universidad Complutense de Madrid Facultad de Ciencias Químicas Dpto. de Bioquímica y Biología Molecular I TRANSCRIPTIONAL PROFILE OF HUMAN ANTI-INFLAMMATORY MACROPHAGES UNDER HOMEOSTATIC, ACTIVATING AND PATHOLOGICAL CONDITIONS Perfil transcripcional de macrófagos antiinflamatorios humanos en condiciones de homeostasis, activación y patológicas. Víctor Delgado Cuevas Tesis Doctoral Madrid 2016 Universidad Complutense de Madrid Facultad de Ciencias Químicas Dpto. de Bioquímica y Biología Molecular I TRANSCRIPTIONAL PROFILE OF HUMAN ANTI-INFLAMMATORY MACROPHAGES UNDER HOMEOSTATIC, ACTIVATING AND PATHOLOGICAL CONDITIONS Perfil transcripcional de macrófagos antiinflamatorios humanos en condiciones de homeostasis, activación y patológicas. Este trabajo ha sido realizado por Víctor Delgado Cuevas para optar al grado de Doctor en el Centro de Investigaciones Biológicas de Madrid (CSIC), bajo la dirección de la Dra. María Marta Escribese Alonso y el Dr. Ángel Luís Corbí López Fdo. Dra. María Marta Escribese