Downloaded from Bioscientifica.Com at 09/30/2021 09:04:02PM Via Free Access
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

View Eposter
Combined glucocorticoid and mineralocorticoid deficiency related to a new NNT mutation : a case report E.Doye 1, CL.Gay 1, S.Castets 1, F.Roucher-Boulez 2, Y.Morel 2, I.Plotton 2, M.Nicolino 1 1 CHU Hospices Civils de Lyon, Service d’Endocrinologie Pédiatrique, Lyon, France ; 2 Hospices Civils de Lyon, Laboratoire d’Endocrinologie Moléculaire et Maladies Rares, Lyon, France BACKGROUND OBJECTIVE Familial glucocorticoid deficiency is an autosomal recessive disorder To describe a new case of familial characterized by specific failure of adrenocortical glucocorticoid glucocorticoid deficiency with combined production in response to adrenocorticotropic hormone (ACTH). mineralocorticoid insufficiency and extra Mutations of the NNT (nicotinamide nucleotide transhydrogenase) adrenal manifestations. gene have recently been implicated in familial glucocorticoid deficiency. RESULTS Suffering from a febrile viral respiratory Diagnosis : during At one month At six months disease, an eight-month-old boy presented hypoglycémia and with status epilepticus caused by severe hypotension hypoglycemia. Multiple medical complications occurred, and invasive ventilation was Natremia (mmol/L) 135 126 136 required for 18 days. The results of blood tests performed during hypoglycemia revealed ACTH (ng/L) 1382 >2000 >2000 adrenal insufficiency. Renin and aldosterone Cortisol (nmol/L) <20 - <20 levels were high but considered consistent Renin (ng/L) 2880 278 177 with the mild hyponatremia and severe hypotension. Subsequent measurements Aldosterone (pmol/L) - 179 72 -

WO 2014/135655 Al 12 September 2014 (12.09.2014) P O P C T
(12) INTERNATIONAL APPLICATION PUBLISHED UNDER THE PATENT COOPERATION TREATY (PCT) (19) World Intellectual Property Organization International Bureau (10) International Publication Number (43) International Publication Date WO 2014/135655 Al 12 September 2014 (12.09.2014) P O P C T (51) International Patent Classification: (81) Designated States (unless otherwise indicated, for every C12Q 1/68 (2006.01) kind of national protection available): AE, AG, AL, AM, AO, AT, AU, AZ, BA, BB, BG, BH, BN, BR, BW, BY, (21) International Application Number: BZ, CA, CH, CL, CN, CO, CR, CU, CZ, DE, DK, DM, PCT/EP2014/054384 DO, DZ, EC, EE, EG, ES, FI, GB, GD, GE, GH, GM, GT, (22) International Filing Date: HN, HR, HU, ID, IL, IN, IR, IS, JP, KE, KG, KN, KP, KR, 6 March 2014 (06.03.2014) KZ, LA, LC, LK, LR, LS, LT, LU, LY, MA, MD, ME, MG, MK, MN, MW, MX, MY, MZ, NA, NG, NI, NO, NZ, (25) Filing Language: English OM, PA, PE, PG, PH, PL, PT, QA, RO, RS, RU, RW, SA, (26) Publication Language: English SC, SD, SE, SG, SK, SL, SM, ST, SV, SY, TH, TJ, TM, TN, TR, TT, TZ, UA, UG, US, UZ, VC, VN, ZA, ZM, (30) Priority Data: ZW. 13305253.0 6 March 2013 (06.03.2013) EP (84) Designated States (unless otherwise indicated, for every (71) Applicants: INSTITUT CURIE [FR/FR]; 26 rue d'Ulm, kind of regional protection available): ARIPO (BW, GH, F-75248 Paris cedex 05 (FR). CENTRE NATIONAL DE GM, KE, LR, LS, MW, MZ, NA, RW, SD, SL, SZ, TZ, LA RECHERCHE SCIENTIFIQUE [FR/FR]; 3 rue UG, ZM, ZW), Eurasian (AM, AZ, BY, KG, KZ, RU, TJ, Michel Ange, F-75016 Paris (FR). -

NNT Mutations: a Cause of Primary Adrenal Insufficiency, Oxidative Stress and Extra- Adrenal Defects
175:1 F Roucher-Boulez and others NNT, adrenal and extra-adrenal 175:1 73–84 Clinical Study defects NNT mutations: a cause of primary adrenal insufficiency, oxidative stress and extra- adrenal defects Florence Roucher-Boulez1,2, Delphine Mallet-Motak1, Dinane Samara-Boustani3, Houweyda Jilani1, Asmahane Ladjouze4, Pierre-François Souchon5, Dominique Simon6, Sylvie Nivot7, Claudine Heinrichs8, Maryline Ronze9, Xavier Bertagna10, Laure Groisne11, Bruno Leheup12, Catherine Naud-Saudreau13, Gilles Blondin13, Christine Lefevre14, Laetitia Lemarchand15 and Yves Morel1,2 1Molecular Endocrinology and Rare Diseases, Lyon University Hospital, Bron, France, 2Claude Bernard Lyon 1 University, Lyon, France, 3Pediatric Endocrinology, Gynecology and Diabetology, Necker University Hospital, Paris, France, 4Pediatric Department, Bab El Oued University Hospital, Alger, Algeria, 5Pediatric Endocrinology and Diabetology, American Memorial Hospital, Reims, France, 6Pediatric Endocrinology, Robert Debré Hospital, Paris, France, 7Department of Pediatrics, Rennes Teaching Hospital, Rennes, France, 8Pediatric Endocrinology, Queen Fabiola Children’s University Hospital, Brussels, Belgium, 9Endocrinology Department, L.-Hussel Hospital, Vienne, France, 10Endocrinology Department, Cochin University Hospital, Paris, France, 11Endocrinology Department, Lyon University Hospital, Bron-Lyon, France, 12Paediatric and Clinical Genetic Department, Correspondence Nancy University Hospital, Vandoeuvre les Nancy, France, 13Pediatric Endocrinology and Diabetology, should be -

SAMD9 and SAMD9L in Inherited Predisposition to Ataxia, Pancytopenia, and Myeloid Malignancies
Leukemia (2018) 32:1106–1115 https://doi.org/10.1038/s41375-018-0074-4 REVIEW ARTICLE Myelodysplastic syndrome SAMD9 and SAMD9L in inherited predisposition to ataxia, pancytopenia, and myeloid malignancies 1,2 3 1 2 4 5,6 Josef Davidsson ● Andreas Puschmann ● Ulf Tedgård ● David Bryder ● Lars Nilsson ● Jörg Cammenga Received: 17 October 2017 / Revised: 25 January 2018 / Accepted: 31 January 2018 / Published online: 25 February 2018 © The Author(s) 2018. This article is published with open access Abstract Germline mutations in the SAMD9 and SAMD9L genes, located in tandem on chromosome 7, are associated with a clinical spectrum of disorders including the MIRAGE syndrome, ataxia–pancytopenia syndrome and myelodysplasia and leukemia syndrome with monosomy 7 syndrome. Germline gain-of-function mutations increase SAMD9 or SAMD9L’s normal antiproliferative effect. This causes pancytopenia and generally restricted growth and/or specific organ hypoplasia in non- hematopoietic tissues. In blood cells, additional somatic aberrations that reverse the germline mutation’s effect, and give rise to the clonal expansion of cells with reduced or no antiproliferative effect of SAMD9 or SAMD9L include complete or partial chromosome 7 loss or loss-of-function mutations in SAMD9 or SAMD9L. Furthermore, the complete or partial loss of chromosome 7q may cause myelodysplastic syndrome in these patients. SAMD9 mutations appear to associate with a more 1234567890();,: severe disease phenotype, including intrauterine growth restriction, developmental delay and hypoplasia of adrenal glands, testes, ovaries or thymus, and most reported patients died in infancy or early childhood due to infections, anemia and/or hemorrhages. SAMD9L mutations have been reported in a few families with balance problems and nystagmus due to cerebellar atrophy, and may lead to similar hematological disease as seen in SAMD9 mutation carriers, from early childhood to adult years. -

Master Thesis
Mutagenic Interrogation of SAMD9 and SAMD9L Function Master Thesis For the attainment of the academic degree Master of Science From the University of Applied Sciences FH Campus Wien Submitted by: Tamara Szattler Personal identity code 1510544055 Supervisor: Yenan Bryceson Karolinska Institutet Stockholm Sweden Submitted on: 29.03.2018 1. Abstract in English Heterozygous gain - of - function m utations in SAMD9 and SAMD9L , two homologues on human chromosome 7, a re associated with severe clinical mani festations such as early onset bone marrow failure, cytopenia and monosomy 7 with high risk of progression to myelodysplastic syndrome (MDS) or acute myeloid leukemia (AML) . Additionally, biallelic SAMD9 mutations have been associated with normophosphatemi c tumoral calcinosis ( NFTC ) . SAMD9 and SAMD9L inhibit cell proliferation and are characterized as tumor suppressors. However, t he physiological function and regulation of SAMD9 and SAMD9L remains unclear . To identify the mechanisms through which mutated SA MD9/SAMD9L cause pathogenesis , it is instrumental to evaluate and characterize novel variants in functional assays. Additionally, targeting specific sites for mutagenesis and evaluate the effects on protein function can provide understanding of how individ ual domains in SAMD9/SAMD9L function . A ssessment of new variants requires a robust method . I have optimized a protocol for the evaluation of SAMD9/SAMD9L variants. In this context, I tested effects of several disease - associated as well as designed mutation s in SAMD9 and SAMD9L on cell proliferation and cell cycle progression. The presented data on SAMD9/SAMD9L variants associated with myeloid malignancies correlate with previous findings of others and suggest that these mutations enhance the function of the tumor suppressors . -

Downloaded Via Ensembl While Using HISAT2
viruses Article Interactions of Viral Proteins from Pathogenic and Low or Non-Pathogenic Orthohantaviruses with Human Type I Interferon Signaling Giulia Gallo 1,2, Grégory Caignard 3, Karine Badonnel 4, Guillaume Chevreux 5, Samuel Terrier 5, Agnieszka Szemiel 6, Gleyder Roman-Sosa 7,†, Florian Binder 8, Quan Gu 6, Ana Da Silva Filipe 6, Rainer G. Ulrich 8 , Alain Kohl 6, Damien Vitour 3 , Noël Tordo 1,9 and Myriam Ermonval 1,* 1 Unité des Stratégies Antivirales, Institut Pasteur, 75015 Paris, France; [email protected] (G.G.); [email protected] (N.T.) 2 Ecole Doctorale Complexité du Vivant, Sorbonne Université, 75006 Paris, France 3 UMR 1161 Virologie, Anses-INRAE-EnvA, 94700 Maisons-Alfort, France; [email protected] (G.C.); [email protected] (D.V.) 4 BREED, INRAE, Université Paris-Saclay, 78350 Jouy-en-Josas, France; [email protected] 5 Institut Jacques Monod, CNRS UMR 7592, ProteoSeine Mass Spectrometry Plateform, Université de Paris, 75013 Paris, France; [email protected] (G.C.); [email protected] (S.T.) 6 MRC-University of Glasgow Centre for Virus Research, Glasgow G61 1QH, UK; [email protected] (A.S.); [email protected] (Q.G.); ana.dasilvafi[email protected] (A.D.S.F.); [email protected] (A.K.) 7 Unité de Biologie Structurale, Institut Pasteur, 75015 Paris, France; [email protected] 8 Friedrich-Loeffler-Institut, Institute of Novel and Emerging Infectious Diseases, 17493 Greifswald-Insel Riems, Germany; binderfl[email protected] (F.B.); rainer.ulrich@fli.de (R.G.U.) Citation: Gallo, G.; Caignard, G.; 9 Institut Pasteur de Guinée, BP 4416 Conakry, Guinea Badonnel, K.; Chevreux, G.; Terrier, S.; * Correspondence: [email protected] Szemiel, A.; Roman-Sosa, G.; † Current address: Institut Für Virologie, Justus-Liebig-Universität, 35390 Giessen, Germany. -

UC Irvine UC Irvine Previously Published Works
UC Irvine UC Irvine Previously Published Works Title The C57BL/6J Mouse Strain Background Modifies the Effect of a Mutation in Bcl2l2 Permalink https://escholarship.org/uc/item/5152r99k Journal G3-Genes|Genomes|Genetics, 2(1) ISSN 2160-1836 Authors Navarro, S. J Trinh, T. Lucas, C. A et al. Publication Date 2012-01-06 DOI 10.1534/g3.111.000778 License https://creativecommons.org/licenses/by/4.0/ 4.0 Peer reviewed eScholarship.org Powered by the California Digital Library University of California INVESTIGATION The C57BL/6J Mouse Strain Background Modifies the Effect of a Mutation in Bcl2l2 Stefanie J. Navarro, Tuyen Trinh, Charlotte A. Lucas, Andrea J. Ross, Katrina G. Waymire, and Grant R. MacGregor1 Department of Developmental and Cell Biology, School of Biological Sciences, and Center for Molecular and Mitochondrial Medicine and Genetics, University of California Irvine, Irvine, California 92697-2300 ABSTRACT Bcl2l2 encodes BCL-W, an antiapoptotic member of the BCL-2 family of proteins. Intercross of KEYWORDS Bcl2l2 +/2 mice on a mixed C57BL/6J, 129S5 background produces Bcl2l2 2/2 animals with the expected –Nnt frequency. In contrast, intercross of Bcl2l2 +/2 mice on a congenic C57BL/6J background produces rela- mutation, genetic tively few live-born Bcl2l2 2/2 animals. Genetic modifiers alter the effect of a mutation. C57BL/6J mice modifier, BCL-W, (Mus musculus) have a mutant allele of nicotinamide nucleotide transhydrogenase (Nnt) that can act as apoptosis a modifier. Loss of NNT decreases the concentration of reduced nicotinamide adenine dinucleotide phos- phate within the mitochondrial matrix. Nicotinamide adenine dinucleotide phosphate is a cofactor for glutathione reductase, which regenerates reduced glutathione, an important antioxidant. -

NNT Is a Key Regulator of Adrenal Redox Homeostasis and Steroidogenesis in Male Mice
236 1 Journal of E Meimaridou et al. NNT is key for adrenal redox 236:1 13–28 Endocrinology and steroid control RESEARCH NNT is a key regulator of adrenal redox homeostasis and steroidogenesis in male mice E Meimaridou1,*, M Goldsworthy2, V Chortis3,4, E Fragouli1, P A Foster3,4, W Arlt3,4, R Cox2 and L A Metherell1 1Centre for Endocrinology, William Harvey Research Institute, John Vane Science Centre, Queen Mary, University of London, London, UK 2MRC Harwell Institute, Genetics of Type 2 Diabetes, Mammalian Genetics Unit, Oxfordshire, UK 3Institute of Metabolism and Systems Research, University of Birmingham, Birmingham, UK 4Centre for Endocrinology, Diabetes and Metabolism, Birmingham Health Partners, Birmingham, UK *(E Meimaridou is now at School of Human Sciences, London Metropolitan University, London, UK) Correspondence should be addressed to E Meimaridou: [email protected] Abstract Nicotinamide nucleotide transhydrogenase, NNT, is a ubiquitous protein of the Key Words inner mitochondrial membrane with a key role in mitochondrial redox balance. NNT f RNA sequencing produces high concentrations of NADPH for detoxification of reactive oxygen species f nicotinamide nucleotide by glutathione and thioredoxin pathways. In humans, NNT dysfunction leads to an transhydrogenase adrenal-specific disorder, glucocorticoid deficiency. Certain substrains of C57BL/6 mice f redox homeostasis contain a spontaneously occurring inactivating Nnt mutation and display glucocorticoid f steroidogenesis Endocrinology deficiency along with glucose intolerance and reduced insulin secretion. To understand f ROS scavengers of the underlying mechanism(s) behind the glucocorticoid deficiency, we performed comprehensive RNA-seq on adrenals from wild-type (C57BL/6N), mutant (C57BL/6J) Journal and BAC transgenic mice overexpressing Nnt (C57BL/6JBAC). -

NADPH Homeostasis in Cancer: Functions, Mechanisms and Therapeutic Implications
Signal Transduction and Targeted Therapy www.nature.com/sigtrans REVIEW ARTICLE OPEN NADPH homeostasis in cancer: functions, mechanisms and therapeutic implications Huai-Qiang Ju 1,2, Jin-Fei Lin1, Tian Tian1, Dan Xie 1 and Rui-Hua Xu 1,2 Nicotinamide adenine dinucleotide phosphate (NADPH) is an essential electron donor in all organisms, and provides the reducing power for anabolic reactions and redox balance. NADPH homeostasis is regulated by varied signaling pathways and several metabolic enzymes that undergo adaptive alteration in cancer cells. The metabolic reprogramming of NADPH renders cancer cells both highly dependent on this metabolic network for antioxidant capacity and more susceptible to oxidative stress. Modulating the unique NADPH homeostasis of cancer cells might be an effective strategy to eliminate these cells. In this review, we summarize the current existing literatures on NADPH homeostasis, including its biological functions, regulatory mechanisms and the corresponding therapeutic interventions in human cancers, providing insights into therapeutic implications of targeting NADPH metabolism and the associated mechanism for cancer therapy. Signal Transduction and Targeted Therapy (2020) 5:231; https://doi.org/10.1038/s41392-020-00326-0 1234567890();,: BACKGROUND for biosynthetic reactions to sustain their rapid growth.5,11 This In cancer cells, the appropriate levels of intracellular reactive realization has prompted molecular studies of NADPH metabolism oxygen species (ROS) are essential for signal transduction and and its exploitation for the development of anticancer agents. cellular processes.1,2 However, the overproduction of ROS can Recent advances have revealed that therapeutic modulation induce cytotoxicity and lead to DNA damage and cell apoptosis.3 based on NADPH metabolism has been widely viewed as a novel To prevent excessive oxidative stress and maintain favorable and effective anticancer strategy. -

Somatic Mutations and Progressive Monosomy Modify SAMD9-Related Phenotypes in Humans
Downloaded from http://www.jci.org on June 26, 2017. https://doi.org/10.1172/JCI91913 RESEARCH ARTICLE The Journal of Clinical Investigation Somatic mutations and progressive monosomy modify SAMD9-related phenotypes in humans Federica Buonocore,1 Peter Kühnen,2 Jenifer P. Suntharalingham,1 Ignacio Del Valle,1 Martin Digweed,3 Harald Stachelscheid,4 Noushafarin Khajavi,2 Mohammed Didi,5 Angela F. Brady,6 Oliver Blankenstein,2 Annie M. Procter,7 Paul Dimitri,8 Jerry K.H. Wales,9 Paolo Ghirri,10 Dieter Knöbl,11 Brigitte Strahm,12 Miriam Erlacher,12,13 Marcin W. Wlodarski,12,13 Wei Chen,14 George K. Kokai,15 Glenn Anderson,16 Deborah Morrogh,17 Dale A. Moulding,18 Shane A. McKee,19 Charlotte M. Niemeyer,12,13 Annette Grüters,2 and John C. Achermann1 1Genetics and Genomic Medicine, University College London (UCL) Great Ormond Street Institute of Child Health, London, United Kingdom. 2Institute of Experimental Pediatric Endocrinology and Department of Pediatric Endocrinology, Charité, Berlin, Germany. 3Department of Human and Medical Genetics, Charité, Berlin, Germany. 4Berlin Institute of Health, Berlin, Germany, and Berlin-Brandenburg Centrum for Regenerative Therapies, Charité, Berlin, Germany. 5Department of Paediatric Endocrinology, Alder Hey Children’s NHS Foundation Trust, Liverpool, United Kingdom. 6North West Thames Regional Genetics Service, Northwick Park Hospital, Harrow, United Kingdom. 7Institute of Medical Genetics, University Hospital of Wales, Cardiff, United Kingdom. 8Academic Unit of Child Health, University of Sheffield, Sheffield, United Kingdom. 9Department of Endocrinology, Children’s Health Queensland Clinical Unit, University of Queensland, Brisbane, Australia. 10Department of Neonatology, University of Pisa, Pisa, Italy. 11Pediatric Endocrinology, Karlsruhe, Germany. -

Unique Genetic and Clinical Features of GATA2 Deficiency and SAMD9/ SAMD9L Syndromes
Best Practice & Research Clinical Haematology 33 (2020) 101197 Contents lists available at ScienceDirect Best Practice & Research Clinical Haematology journal homepage: www.elsevier.com/locate/issn/15216926 Germline predisposition in myeloid neoplasms: Unique genetic and clinical features of GATA2 deficiency and SAMD9/ SAMD9L syndromes Sushree S. Sahoo a, Emilia J. Kozyra b,c, Marcin W. Wlodarski a,b,* a Department of Hematology, St. Jude Children’s Research Hospital, Memphis, USA b Division of Pediatric Hematology and Oncology, Department of Pediatrics and Adolescent Medicine, Medical Center, Faculty of Medicine, University of Freiburg, Germany c Faculty of Biology, University of Freiburg, Freiburg, Germany ARTICLE INFO ABSTRACT Keywords: Increasing awareness about germline predisposition and the widespread application of unbiased Germline predisposition whole exome sequencing contributed to the discovery of new clinical entities with high risk for Hereditary MDS the development of haematopoietic malignancies. The revised 2016 WHO classification intro GATA2 duced a novel category of “myeloid neoplasms with germline predisposition” with GATA2, SAMD9 CEBPA, DDX41, RUNX1, ANKRD26 and ETV6 genes expanding the spectrum of hereditary SAMD9L myeloid neoplasms (MN). Since then, more germline causes of MN were identified, including SAMD9, SAMD9L, and ERCC6L2. This review describes the genetic and clinical spectrum of predisposition to MN. The main focus lies in delineation of phenotypes, genetics and management of GATA2 deficiency and the novel SAMD9/SAMD9L-related disorders. Combined, GATA2 and SAMD9/SAMD9L (SAMD9/9L) syndromes are recognized as most frequent causes of primary paediatric myelodysplastic syndromes, particularly in setting of monosomy 7. To date, ~550 cases with germline GATA2 mutations, and ~130 patients with SAMD9/9L mutations had been reported in literature. -
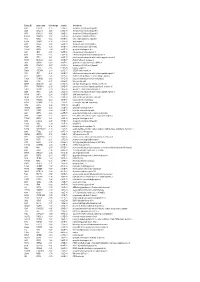
Entrez ID Gene Name Fold Change Q-Value Description
Entrez ID gene name fold change q-value description 4283 CXCL9 -7.25 5.28E-05 chemokine (C-X-C motif) ligand 9 3627 CXCL10 -6.88 6.58E-05 chemokine (C-X-C motif) ligand 10 6373 CXCL11 -5.65 3.69E-04 chemokine (C-X-C motif) ligand 11 405753 DUOXA2 -3.97 3.05E-06 dual oxidase maturation factor 2 4843 NOS2 -3.62 5.43E-03 nitric oxide synthase 2, inducible 50506 DUOX2 -3.24 5.01E-06 dual oxidase 2 6355 CCL8 -3.07 3.67E-03 chemokine (C-C motif) ligand 8 10964 IFI44L -3.06 4.43E-04 interferon-induced protein 44-like 115362 GBP5 -2.94 6.83E-04 guanylate binding protein 5 3620 IDO1 -2.91 5.65E-06 indoleamine 2,3-dioxygenase 1 8519 IFITM1 -2.67 5.65E-06 interferon induced transmembrane protein 1 3433 IFIT2 -2.61 2.28E-03 interferon-induced protein with tetratricopeptide repeats 2 54898 ELOVL2 -2.61 4.38E-07 ELOVL fatty acid elongase 2 2892 GRIA3 -2.60 3.06E-05 glutamate receptor, ionotropic, AMPA 3 6376 CX3CL1 -2.57 4.43E-04 chemokine (C-X3-C motif) ligand 1 7098 TLR3 -2.55 5.76E-06 toll-like receptor 3 79689 STEAP4 -2.50 8.35E-05 STEAP family member 4 3434 IFIT1 -2.48 2.64E-03 interferon-induced protein with tetratricopeptide repeats 1 4321 MMP12 -2.45 2.30E-04 matrix metallopeptidase 12 (macrophage elastase) 10826 FAXDC2 -2.42 5.01E-06 fatty acid hydroxylase domain containing 2 8626 TP63 -2.41 2.02E-05 tumor protein p63 64577 ALDH8A1 -2.41 6.05E-06 aldehyde dehydrogenase 8 family, member A1 8740 TNFSF14 -2.40 6.35E-05 tumor necrosis factor (ligand) superfamily, member 14 10417 SPON2 -2.39 2.46E-06 spondin 2, extracellular matrix protein 3437