Advances in Anesthesia Technology Are Improving Patient Care, but Many Challenges Remain D
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Data Driven Investigation of Bispectral Index Algorithm
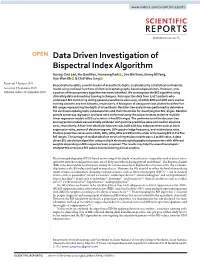
www.nature.com/scientificreports OPEN Data Driven Investigation of Bispectral Index Algorithm Hyung-Chul Lee, Ho-Geol Ryu, Yoonsang Park , Soo Bin Yoon, Seong Mi Yang, Hye-Won Oh & Chul-Woo Jung Received: 7 January 2019 Bispectral index (BIS), a useful marker of anaesthetic depth, is calculated by a statistical multivariate Accepted: 9 September 2019 model using nonlinear functions of electroencephalography-based subparameters. However, only Published: xx xx xxxx a portion of the proprietary algorithm has been identifed. We investigated the BIS algorithm using clinical big data and machine learning techniques. Retrospective data from 5,427 patients who underwent BIS monitoring during general anaesthesia were used, of which 80% and 20% were used as training datasets and test datasets, respectively. A histogram of data points was plotted to defne fve BIS ranges representing the depth of anaesthesia. Decision tree analysis was performed to determine the electroencephalography subparameters and their thresholds for classifying fve BIS ranges. Random sample consensus regression analyses were performed using the subparameters to derive multiple linear regression models of BIS calculation in fve BIS ranges. The performance of the decision tree and regression models was externally validated with positive predictive value and median absolute error, respectively. A four-level depth decision tree was built with four subparameters such as burst suppression ratio, power of electromyogram, 95% spectral edge frequency, and relative beta ratio. Positive predictive values were 100%, 80%, 80%, 85% and 89% in the order of increasing BIS in the fve BIS ranges. The average of median absolute errors of regression models was 4.1 as BIS value. -

The Bispectral Index Response to Tracheal Intubation Is Similar In
458 GENERAL ANESTHESIA The bispectral index response to tracheal intuba- tion is similar in normotensive and hypertensive patients [La réponse de l’index bispectral à l’intubation endotrachéale est similaire chez les patients normotendus et hypertendus] Masayasu Nakayama MD,* Hiromichi Ichinose MD,† Shuji Yamamoto MD,† Noriaki Kanaya MD,* Akiyoshi Namiki MD PhD* Purpose: To compare the hemodynamic and bispectral index (BIS) Conclusion : Les patients hypertendus ou non réagissent par la même responses to tracheal intubation in normotensive and hypertensive réaction d’éveil (mesurée par le BIS) à l’intubation endotrachéale mal- patients. gré l’augmentation de la réponse vasopressive chez les hypertendus. Method: Three minutes after induction of anesthesia with thiamy- lal and fentanyl, tracheal intubation was performed in 24 nor- motensive and 22 hypertensive patients. Heart rate (HR), mean arterial pressure (MAP), and BIS were measured every minute. HE bispectral index (BIS), obtained from Results: Tracheal intubation increased HR, MAP, and BIS in both bispectral analysis of the electroencephalo- normotensive and hypertensive patients. The increase in MAP was gram (EEG), reflects the hypnotic compo- significantly greater in hypertensive patients than in normotensive nent of anesthesia.1–3 Previous studies have patients, but there were no differences in HR or BIS in the two T shown that tracheal intubation is associated with groups of patients. increases in BIS as well as heart rate (HR) and blood Conclusion: Patients with and without hypertension exhibit the pressure.4–6 Therefore, intubation is likely to affect same arousal response (as measured by BIS) to tracheal intubation both the hypnotic and antinociceptive components of despite the enhanced vasopressor response in hypertensive anesthesia. -

The Introduction of Bispectral Index (BIS) in Anesthesia Practice
EDITORIAL VIEW The introduction of bispectral index (BIS) in anesthesia practice Dario Galante, MD, Matteo Melchionda, MD University Department of Anesthesia and Intensive Care University Hospital Ospedali Riuniti, Foggia, Italy Correspondance: Dario Galante, MD, University Department of Anesthesia and Intensive Care, University Hospital Ospedali Riuniti, Foggia (Italy); E-mail: [email protected] SUMMARY During every surgical procedure we must keep the anesthetic level at an appropriate level so that the patient will neither feel pain nor remember the operation. Yet this anesthetic depth must be balanced against the negative effects and consequences of excess anesthetic and the associated potential for delayed wake up. A wide range of monitoring devices allows us to to avoid the risks of pain, unwanted movements, hemodynamic changes as well as awareness. During the past few years processed EEG signals have become available that help gauge the depth of anesthesia by generating a score linked to EEG activity, which becomes depressed as anesthesia deepens. The bispectral index (BIS) represents one of these innovative methods of monitoring in anesthesia, even if more studies are still needed to make it more precise, especially in pediatric patients and neonates where reliability has yet to be well established. Key words: Bispectral index; Neurological monitoring; Awareness; Depth of anesthesia Citation: Galante D, Melchionda M. The introduction of bispectral index (BIS) in anesthesia practice. Anaesth Pain & Intensive Care 2012;16(3):235-236 The Bispectral IndexTM (Aspect Medical Systems Inc., b) It calculates the index of the state of sedation due to Newton, Mass) is a complex EEG parameter that changes induced by anesthetics by an algorithm combines power spectrum analysis, time domain analysis c) It obtains the value that is recorded by means of a and it values their changes over time. -

Recommendations for Standards of Monitoring During Anaesthesia and Recovery 2021 Klein, A
University of Dundee Recommendations for standards of monitoring during anaesthesia and recovery 2021 Klein, A. A.; Meek, T.; Allcock, E.; Cook, T. M.; Mincher, N.; Morris, C. Published in: Anaesthesia DOI: 10.1111/anae.15501 Publication date: 2021 Licence: CC BY-NC-ND Document Version Publisher's PDF, also known as Version of record Link to publication in Discovery Research Portal Citation for published version (APA): Klein, A. A., Meek, T., Allcock, E., Cook, T. M., Mincher, N., Morris, C., Nimmo, A. F., Pandit, J. J., Pawa, A., Rodney, G., Sheraton, T., & Young, P. (2021). Recommendations for standards of monitoring during anaesthesia and recovery 2021: Guideline from the Association of Anaesthetists. Anaesthesia, 76(9), 1212- 1223. https://doi.org/10.1111/anae.15501 General rights Copyright and moral rights for the publications made accessible in Discovery Research Portal are retained by the authors and/or other copyright owners and it is a condition of accessing publications that users recognise and abide by the legal requirements associated with these rights. • Users may download and print one copy of any publication from Discovery Research Portal for the purpose of private study or research. • You may not further distribute the material or use it for any profit-making activity or commercial gain. • You may freely distribute the URL identifying the publication in the public portal. Take down policy If you believe that this document breaches copyright please contact us providing details, and we will remove access to the work immediately and investigate your claim. Download date: 01. Oct. 2021 Anaesthesia 2021 doi:10.1111/anae.15501 Guidelines Recommendations for standards of monitoring during anaesthesia and recovery 2021 Guideline from the Association of Anaesthetists A. -

Bispectral Index Monitoring During General Anesthesia
Name of Blue Advantage Policy: Bispectral Index Monitoring During General Anesthesia Policy #: 262 Latest Review Date: October 2019 Category: Other Policy Grade: Effective March 14, 2012: Active Policy but no longer scheduled for regular literature reviews and updates. BACKGROUND: Blue Advantage medical policy does not conflict with Local Coverage Determinations (LCDs), Local Medical Review Policies (LMRPs) or National Coverage Determinations (NCDs) or with coverage provisions in Medicare manuals, instructions or operational policy letters. In order to be covered by Blue Advantage the service shall be reasonable and necessary under Title XVIII of the Social Security Act, Section 1862(a)(1)(A). The service is considered reasonable and necessary if it is determined that the service is: 1. Safe and effective; 2. Not experimental or investigational*; 3. Appropriate, including duration and frequency that is considered appropriate for the service, in terms of whether it is: • Furnished in accordance with accepted standards of medical practice for the diagnosis or treatment of the patient’s condition or to improve the function of a malformed body member; • Furnished in a setting appropriate to the patient’s medical needs and condition; • Ordered and furnished by qualified personnel; • One that meets, but does not exceed, the patient’s medical need; and • At least as beneficial as an existing and available medically appropriate alternative. *Routine costs of qualifying clinical trial services with dates of service on or after September 19, 2000 which meet the requirements of the Clinical Trials NCD are considered reasonable and necessary by Medicare. Providers should bill Original Medicare for covered services that are related to clinical trials that meet Medicare requirements (Refer to Medicare National Coverage Determinations Manual, Chapter 1, Section 310 and Medicare Claims Processing Manual Chapter 32, Sections 69.0-69.11). -

Title Page Monitoring and Reversal Of
TITLE PAGE MONITORING AND REVERSAL OF NEUROMUSCULAR BLOCKADE: A COMPARISON OF CLINICAL VERSUS QUALITATIVE ASSESSMENTS BY DR AYENI, Olajide O. (M.B.B.S., BENIN) A DISSERTATION SUBMITTED IN PARTIAL FULFILLMENT FOR THE AWARD OF THE FELLOWSHIP OF THE NATIONAL POSTGRADUATE MEDICAL COLLEGE OF NIGERIA, IN THE FACULTY OF ANAESTHESIA (FMCA). NOVEMBER 2015 ATTESTATION We hereby attest that this research titled “MONITORING AND REVERSAL OF NEUROMUSCULAR BLOCKADE: A COMPARISON OF CLINICAL VERSUS QUALITATIVE ASSESSMENTS” was carried out by Dr Olajide O. AYENI. We have reviewed and supervised the conduct of the study. --------------------------------------------------------- PROF O.T KUSHIMO Supervisor Consultant Anaesthetist Lagos University Teaching Hospital (LUTH). -------------------------------------- -------------------------------------- DR A. MAFE DR. AKINTIMEHIN Supervisor Supervisor Consultant Anaesthetist Consultant Anaesthetist Lagos Island General Hospital GbagadaGeneraHospital Hospital Lagos. Lagos. 2 CERTIFICATION I certify that this research titled “MONITORING AND REVERSAL OF NEUROMUSCULAR BLOCKADE: A COMPARISON OF CLINICAL VERSUS QUALITATIVE ASSESSMENTS” by Dr Olajide O. AYENI was conducted in the Department of Anaesthesia, LASUTH. --------------------------------------------------------- DR A.A MAJEKODUNMI Head of Department Department of Anaesthesia, LASUTH. 3 DECLARATION It is hereby declared that this work is original and done by me. I also acknowledge that the work has not been presented to any other College for a Fellowship nor -

Capnography and the Bispectral Index—Their Role in Pediatric Sedation: a Brief Review
Hindawi Publishing Corporation International Journal of Pediatrics Volume 2010, Article ID 828347, 5 pages doi:10.1155/2010/828347 Review Article Capnography and the Bispectral Index—Their Role in Pediatric Sedation: A Brief Review Maria Sammartino,1 Barbara Volpe,2 Fabio Sbaraglia,1 Rossella Garra,1 and Alessandro D’Addessi3 1 Department of Anesthesia and Intensive Care, Catholic University of Sacred Heart, 00168 Rome, Italy 2 Department of Anesthesia and Intensive Care, General Hospital San Giovanni Calibita, IsolaTiberina, 00186 Rome, Italy 3 Urology Department, Catholic University of Sacred Heart, Policlinico A. Gemelli, Largo F. Vito 1, 00168 Rome, Italy Correspondence should be addressed to Alessandro D’Addessi, [email protected] Received 3 December 2009; Revised 5 June 2010; Accepted 20 July 2010 Academic Editor: Savithiri Ratnapalan Copyright © 2010 Maria Sammartino et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Sedation in children is increasingly emerging as a minimally invasive technique that may be associated with local anaesthesia or diagnostic and therapeutic procedures which do not necessarily require general anaesthesia. Standard monitoring requirements are not sufficient to ensure an effective control of pulmonary ventilation and deep sedation. Capnography in pediatric sedation assesses the effect of different drugs on the occurrence of respiratory failure and records early indicators of respiratory impairment. The Bispectral index (BIS) allows the reduction of dose requirements of anaesthetic drugs, the reduction in the time to extubation and eye opening, and the reduction in the time to discharge. -

Optimizing Bispectral Index (BIS) Use in the Intensive Care Unit: Development of a Procedure and Skill Competency Validation for Critical Care Nurses
University of North Dakota UND Scholarly Commons Theses and Dissertations Theses, Dissertations, and Senior Projects 8-1-2005 Optimizing Bispectral Index (BIS) Use in the Intensive Care Unit: Development of a Procedure and Skill Competency Validation for Critical Care Nurses Twyla G. Kouba Follow this and additional works at: https://commons.und.edu/theses Recommended Citation Kouba, Twyla G., "Optimizing Bispectral Index (BIS) Use in the Intensive Care Unit: Development of a Procedure and Skill Competency Validation for Critical Care Nurses" (2005). Theses and Dissertations. 3147. https://commons.und.edu/theses/3147 This Independent Study is brought to you for free and open access by the Theses, Dissertations, and Senior Projects at UND Scholarly Commons. It has been accepted for inclusion in Theses and Dissertations by an authorized administrator of UND Scholarly Commons. For more information, please contact [email protected]. OPTIMIZING BISPECTRAL INDEX (BIS) USE IN THE INTENSIVE CARE UNIT: DEVELOPMENT OF A PROCEDURE AND SKILL COMPETENCY VALIDATION FOR CRITICAL CARE NURSES by Twyla G. Kouba Bachelor of Science, University of North Dakota, 2000 An Independent Study Submitted to the Graduate Faculty of the University of North Dakota in partial fulfillment of the requirements for the degree of Master of Science Grand Forks, North Dakota August 2005 FEB 17 2005 TABLE OF CONTENTS CHAPTER I INTRODUCTION.......................................................................................1 Clinical Problem............................................................................ -
Review Course Lectures
Review Course Lectures presented at the 2010 Annual Meeting of the International Anesthesia Research Society Honolulu, Hawaii March 20-23, 2010 IARS 2009 REVIEW COURSE LECTURES The material included in the publication has not undergone peer review or review by the Editorial Board of Anesthesia and Analgesia for this publication. Any of the material in this publication may have been transmitted by the author to IARS in various forms of electronic medium. IARS has used its best efforts to receive and format electronic submissions for this publication but has not reviewed each abstract for the purpose of textual error correction and is not liable in any way for any formatting, textual, or grammatical error or inaccuracy. ©2010 International Anesthesia Research Society 2 ©International Anesthesia Research Society. Unauthorized Use Prohibited. IARS 2009 REVIEW COURSE LECTURES Table of Contents Ultrasound Guided Regional Anesthesia in Infants, Neuroanesthesia for the Occasional Children and Adolescents Neuroanesthesiologist Santhanam Suresh, MD FAAP .................1 Adrian W. Gelb ............................36 Vice Chairman, Department of Pediatric Anesthesi- Professor & Vice Chair ology, Children’s Memorial Hospital Department of Anesthesia & Perioperative Care Prof. of Anesthesiology & Pediatrics, Northwestern University of California San Francisco University’s Feinberg School of Medicine, Chicago, IL Perioperative Control Of Hypertension: When Does Neuromuscular Blockers and their Reversal in 2010 It Adversely Affect Perioperative Outcome? François Donati, PhD, MD.....................6 John W. Sear, MA, PhD, FFARCS, FANZCA .......39 Professor, Departement of Anesthesiology Nuffield Department of Anesthetics, Université de montréal University of Oxford, John Radcliffe Hospital Montréal, Québec, Canada Oxford, United Kingdom Anaphylactic and Anaphylactoid Perioperative Approach to Patients with Reactions in the Surgical Patient Respiratory Disease: Is There a Role \Jerrold H. -

Analysis 1.1
Cochrane Database of Systematic Reviews Avoidance versus use of neuromuscular blocking agents for improving conditions during tracheal intubation or direct laryngoscopy in adults and adolescents (Review) Lundstrøm LH, Duez CHV, Nørskov AK, Rosenstock CV, Thomsen JL, Møller AM, Strande S, Wetterslev J Lundstrøm LH, Duez CHV, Nørskov AK, Rosenstock CV, Thomsen JL, Møller AM, Strande S, Wetterslev J. Avoidance versus use of neuromuscular blocking agents for improving conditions during tracheal intubation or direct laryngoscopy in adults and adolescents. Cochrane Database of Systematic Reviews 2017, Issue 5. Art. No.: CD009237. DOI: 10.1002/14651858.CD009237.pub2. www.cochranelibrary.com Avoidance versus use of neuromuscular blocking agents for improving conditions during tracheal intubation or direct laryngoscopy in adults and adolescents (Review) Copyright © 2017 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd. TABLE OF CONTENTS HEADER....................................... 1 ABSTRACT ...................................... 1 PLAINLANGUAGESUMMARY . 2 SUMMARY OF FINDINGS FOR THE MAIN COMPARISON . ..... 4 BACKGROUND .................................... 7 OBJECTIVES ..................................... 8 METHODS ...................................... 8 RESULTS....................................... 12 Figure1. ..................................... 13 Figure2. ..................................... 15 Figure3. ..................................... 17 Figure4. ..................................... 18 Figure5. .................................... -

Bispectral Index Monitoring During General Anesthesia
Name of Blue Advantage Policy: Bispectral Index Monitoring During General Anesthesia Policy #: 262 Latest Review Date: January 2010 Category: Other Policy Grade: Effective March 14, 2012: Active Policy but no longer scheduled for regular literature reviews and updates. Background: Blue Advantage medical policy does not conflict with Local Coverage Determinations (LCDs), Local Medical Review Policies (LMRPs) or National Coverage Determinations (NCDs) or with coverage provisions in Medicare manuals, instructions or operational policy letters. In order to be covered by Blue Advantage the service shall be reasonable and necessary under Title XVIII of the Social Security Act, Section 1862(a)(1)(A). The service is considered reasonable and necessary if it is determined that the service is: 1. Safe and effective; 2. Not experimental or investigational*; 3. Appropriate, including duration and frequency that is considered appropriate for the service, in terms of whether it is: • Furnished in accordance with accepted standards of medical practice for the diagnosis or treatment of the patient’s condition or to improve the function of a malformed body member; • Furnished in a setting appropriate to the patient’s medical needs and condition; • Ordered and furnished by qualified personnel; • One that meets, but does not exceed, the patient’s medical need; and • At least as beneficial as an existing and available medically appropriate alternative. *Routine costs of qualifying clinical trial services with dates of service on or after September 19, 2000 which meet the requirements of the Clinical Trials NCD are considered reasonable and necessary by Medicare. Providers should bill Original Medicare for covered services that are related to clinical trials that meet Medicare requirements (Refer to Medicare National Coverage Determinations Manual, Chapter 1, Section 310 and Medicare Claims Processing Manual Chapter 32, Sections 69.0-69.11). -

New Frontiers for Neuromuscular Blockade Use and Reversal
New Frontiers for Neuromuscular Blockade Use and Reversal Presented as a Live Webinar On‐demand Activity Recording of live webinar Thursday, November 7, 2019 Available after March 31, 2020 2:00 p.m. ‐ 3:30 p.m. ET Accreditation Faculty Deborah Wagner, Pharm.D., FASHP, Activity Chair The American Society of Health‐System Clinical Professor of Pharmacy Pharmacists is accredited by the University of Michigan College of Pharmacy Accreditation Council for Pharmacy Clinical Professor of Anesthesiology Education as a provider of continuing Michigan Medicine pharmacy education Ann Arbor, Michigan • ACPE #: 0204‐000‐19‐417‐L01‐P Michael Aziz, M.D. • 1.5 hr, application‐based Professor of Anesthesiology and Perioperative Medicine The American Society of Health System Oregon Health & Science University Pharmacists is accredited by the Portland, Oregon Accreditation Council for Continuing Medical Education to provide continuing Rachel C. Wolfe, Pharm.D., M.H.A., BCCCP medical education for physicians. Clinical Pharmacy Specialist Perioperative and Surgical Critical Care The American Society of Health‐System Pharmacists Barnes‐Jewish Hospital designates this live activity for a maximum of 1.5 St. Louis, Missouri AMA PRA Category 1 Credits™. Physicians should claim only the credit commensurate with the extent View faculty bios at of their participation in the activity. www.ashpadvantage.com/reversal/webinar1/ Webinar Information CE Processing Visit www.ashpadvantage.com/reversal/webinar1 Participants will process CE credit online at to find http://elearning.ashp.org/my‐activities. CPE credit Webinar registration link will be reported directly to CPE Monitor. Per ACPE, Group viewing information and technical CPE credit must be claimed no later than 60 days requirements from the date of the live activity or completion of a home‐study activity.