[Ethiopia] – [Tigray Crisis]
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
20210714 Access Snapshot- Tigray Region June 2021 V2
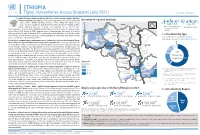
ETHIOPIA Tigray: Humanitarian Access Snapshot (July 2021) As of 31 July 2021 The conflict in Tigray continues despite the unilateral ceasefire announced by the Ethiopian Federal Government on 28 June, which resulted in the withdrawal of the Ethiopian National Overview of reported incidents July Since Nov July Since Nov Defense Forces (ENDF) and Eritrea’s Defense Forces (ErDF) from Tigray. In July, Tigray forces (TF) engaged in a military offensive in boundary areas of Amhara and Afar ERITREA 13 153 2 14 regions, displacing thousands of people and impacting access into the area. #Incidents impacting Aid workers killed Federal authorities announced the mobilization of armed forces from other regions. The Amhara region the security of aid Tahtay North workers Special Forces (ASF), backed by ENDF, maintain control of Western zone, with reports of a military Adiyabo Setit Humera Western build-up on both sides of the Tekezi river. ErDF are reportedly positioned in border areas of Eritrea and in SUDAN Kafta Humera Indasilassie % of incidents by type some kebeles in North-Western and Eastern zones. Thousands of people have been displaced from town Central Eastern these areas into Shire city, North-Western zone. In line with the Access Monitoring and Western Korarit https://bit.ly/3vcab7e May Reporting Framework: Electricity, telecommunications, and banking services continue to be disconnected throughout Tigray, Gaba Wukro Welkait TIGRAY 2% while commercial cargo and flights into the region remain suspended. This is having a major impact on Tselemti Abi Adi town May Tsebri relief operations. Partners are having to scale down operations and reduce movements due to the lack Dansha town town Mekelle AFAR 4% of fuel. -

D.Fig 9.8-1 TRANSMISSION NETWORK STRUCTURE Area-01
D.Fig 9.8-1 TRANSMISSION NETWORK STRUCTURE 1 Area-01 (1/2, 2/2) 2 Area-02 3 Area-03 4 Area-04 5 Area-05 6 Area-06 (1/2, 2/2) 7 Area-07 Jimma 8 Area-07 Nekemte 9 Area-08 (1/2, 2/2) Legend; Link between A station and B station Frequency Band: Transmission Capacity; Expansion Capacity (At the 8th D.P. completion) in the Master Plan AB 7G 2M 7GHz 2M none AB ? 7x2M Not decided 7 x 2M none AB (2M) Not decided none 2M AB 7G 4x2M (+3) 7GHz 4 x 2M 3 x 2M Links among A, B C and D stations A BCD 5G STM-1 (+1) (+1) Frequency Band: Transmission Capacity; Expansion Capacity (At the 8th D.P. completion) in the Master Plan <Link between A and B> 5GHz STM-1 STM-1 <Link between B and C> 5GHz STM-1 none <Link between C and D> 5GHz STM-1 STM-1 1/11 D.Fig9.8-1 NW Structure.xls Sendafa Mt.Furi Mukaturi Chancho Entoto ? 2x2M (2M) ? 4x2M Addis Ababa Sheno South Ankober North Ambalay South Tik Giorgis Gara Guda 2G 8M 5G 3xSTM-1 5G STM-1 (+2) (+2) (+1) (+1) to Dessie to Bahir Dar Fetra Debre Tsige 900M 8M 11G 140M Sheno Town Ankober(Gorebela) (2M) 7G 4x2M (+1) Sululta 2G 2x34M OFC (2M) Gunde Meskel Muger ? 3x2M 2G 4x2M (2x2M) 900M 8M Aleltu Debre Sina Armania Lemi Robit (2M) 900M 2M (2M) (2M) Fitche Alidoro Chacha (+8) Mezezo Debre Tabor Rep Gunde Wein Abafelase (2M) (2M) (2M) 7G 4x2M Meragna Mendida Molale Inchini Kemet Gebrel Gohatsion Gebre Guracha 900M 8M (2x2M) (2M) (2M) ? 2x2M -

Starving Tigray
Starving Tigray How Armed Conflict and Mass Atrocities Have Destroyed an Ethiopian Region’s Economy and Food System and Are Threatening Famine Foreword by Helen Clark April 6, 2021 ABOUT The World Peace Foundation, an operating foundation affiliated solely with the Fletcher School at Tufts University, aims to provide intellectual leadership on issues of peace, justice and security. We believe that innovative research and teaching are critical to the challenges of making peace around the world, and should go hand-in- hand with advocacy and practical engagement with the toughest issues. To respond to organized violence today, we not only need new instruments and tools—we need a new vision of peace. Our challenge is to reinvent peace. This report has benefited from the research, analysis and review of a number of individuals, most of whom preferred to remain anonymous. For that reason, we are attributing authorship solely to the World Peace Foundation. World Peace Foundation at the Fletcher School Tufts University 169 Holland Street, Suite 209 Somerville, MA 02144 ph: (617) 627-2255 worldpeacefoundation.org © 2021 by the World Peace Foundation. All rights reserved. Cover photo: A Tigrayan child at the refugee registration center near Kassala, Sudan Starving Tigray | I FOREWORD The calamitous humanitarian dimensions of the conflict in Tigray are becoming painfully clear. The international community must respond quickly and effectively now to save many hundreds of thou- sands of lives. The human tragedy which has unfolded in Tigray is a man-made disaster. Reports of mass atrocities there are heart breaking, as are those of starvation crimes. -

The Eritrean-Ethiopian Border Dispute
Affairs (1998), 97, 551-565 BRIEFING: THE ERITREAN-ETHIOPIAN BORDER DISPUTE J ABBINK ? * $• • THE VIOLENT Eritrean-Ethiopian border dispute which erupted on 6 May 'this year has taken everybody by surprise, includmg Ethiopian prime minister Mêles Zenawi.1 But on a closer look, this dispute is not so . surprising except for its timing, nor is it only about a border. The 'Wstorical and political context of this widely deplored family quarrel between closely related regimes in Eritrea and Ethiopia makes this clear. , -True, both regimes emerged from armed insurgent movements (EPLF and TPLF)2 which were for many years comrades in arms against the r former Ethiopian government of Lt.-Col. Mengistu Haile Mariam. •; They both shared the same mix of ethno-regionalist/nationalist and l^.'Marxist-Leninist ideology and both their political elites hail from the same .;'•' etfano-linguistic group, the Tigrinya-speakers of northern Ethiopia and , *N '^outhern Eritrea. After they took power m 1991, their leaders were also ?3f,, generously supported by the Western donor-community led by the USA as s 'new-style' African leaders: relatively young, seemingly committed to - > 4emocratization and a new approach to national development, aiming S' at liberal market-economy reforms and at closer intégration with the 3 ,x world community, especially the West. But différences of opinion and 4\ divergent approaches to crucial policy matters existed between the two « iriovements since the late 1970s and have not been resolved since.4 It is more than ironie in this conflict that the policies of these new leaders *< seem to carry the same potential for violence and destabilization m the région as that of old leaders.5 In this respect, the surprise about the fr ' carrent border crisis reveals something of the incomplete historical under- standing and the opportunism of certain donor countries. -

Invest in Ethiopia: Focus MEKELLE December 2012 INVEST in ETHIOPIA: FOCUS MEKELLE
Mekelle Invest in Ethiopia: Focus MEKELLE December 2012 INVEST IN ETHIOPIA: FOCUS MEKELLE December 2012 Millennium Cities Initiative, The Earth Institute Columbia University New York, 2012 DISCLAIMER This publication is for informational This publication does not constitute an purposes only and is meant to be purely offer, solicitation, or recommendation for educational. While our objective is to the sale or purchase of any security, provide useful, general information, product, or service. Information, opinions the Millennium Cities Initiative and other and views contained in this publication participants to this publication make no should not be treated as investment, representations or assurances as to the tax or legal advice. Before making any accuracy, completeness, or timeliness decision or taking any action, you should of the information. The information is consult a professional advisor who has provided without warranty of any kind, been informed of all facts relevant to express or implied. your particular circumstances. Invest in Ethiopia: Focus Mekelle © Columbia University, 2012. All rights reserved. Printed in Canada. ii PREFACE Ethiopia, along with 189 other countries, The challenges that potential investors adopted the Millennium Declaration in would face are described along with the 2000, which set out the millennium devel- opportunities they may be missing if they opment goals (MDGs) to be achieved by ignore Mekelle. 2015. The MDG process is spearheaded in Ethiopia by the Ministry of Finance and The Guide is intended to make Mekelle Economic Development. and what Mekelle has to offer better known to investors worldwide. Although This Guide is part of the Millennium effort we have had the foreign investor primarily and was prepared by the Millennium Cities in mind, we believe that the Guide will be Initiative (MCI), which is an initiative of of use to domestic investors in Ethiopia as The Earth Institute at Columbia University, well. -

The Ethiopia-Eritrea Rapprochement : Peace and Stability in the Horn Of
ETHIOPIA–ERITREA RAPPROCHEMENT: RAPPROCHEMENT: ETHIOPIA–ERITREA THE RECENT RAPPROCHEMENT between Ethiopia and Eritrea has fundamentally reshaped the relation- ship between the two countries. The impact of the resolution of the Ethiopia-Eritrea conflict goes beyond the borders of the two countries, and has indeed AFRICA THE HORN OF IN AND STABILITY PEACE brought fundamental change to the region. Full diplo- The Ethiopia-Eritrea matic relations have been restored between Eritrea and Peace and Stability Somalia; and the leaders of Eritrea and Djibouti have met in Jeddah, Saudi Arabia. The central question the Rapprochement in the Horn of Africa book attempts to address is: what factors led to the resolution of a festering conflict? The book explains and analyses the rapprochement, which it argues was made possible by the maturing of objective and sub- jective conditions in Ethiopia and by the trust factor in Eritrea. REDIE BEREKETEAB is a Senior Researcher and Associate Professor in Sociology at the Nordic Africa Institute in Uppsala, Sweden. His main field of research is conflict and state building in the Horn of Africa, and the regional economic communities (RECs) and peace building in Africa. REDIE BEREKETEAB ISBN 9789171068491 90000 > Policy Dialogue No. 13 Redie Bereketeab 9 789171 068491 POLICY DIALOGUE No. 13 THE ETHIOPIA-ERITREA RAPPROCHEMENT Peace and Stability in the Horn of Africa Author Redie Bereketeab NORDISKA AFRIKAINSITUTET The Nordic Africa Institute UPPSALA 2019 INDEXING TERMS: Ethiopia Eritrea Foreign relations Regional cooperation Regional integration Dispute settlement Political development Peacebuilding Reconciliation The Ethiopia-Eritrea Rapprochement: Peace and Stability in the Horn of Africa Author: Redie Bereketeab ISBN 978-91-7106-849-1 print ISBN 978-91-7106-850-7 pdf © 2019 The author and the Nordic Africa Institute Layout: Henrik Alfredsson, The Nordic Africa Institute and Marianne Engblom, Ateljé Idé. -

ETHIOPIA - TIGRAY REGION HUMANITARIAN UPDATE Situation in Tigray (1 July 2021) Last Updated: 2 Jul 2021
ETHIOPIA - TIGRAY REGION HUMANITARIAN UPDATE Situation in Tigray (1 July 2021) Last updated: 2 Jul 2021 FLASH UPDATE (2 Jul 2021) Situation in Tigray (1 July 2021) The political dynamics have changed dramatically in Ethiopia's Tigray Region following the unilateral ceasefire declaration by the Ethiopian Government on 28 June 2021. Reportedly, the Tigray Defense Forces (TDF) have taken control over most parts of Tigray following the withdrawal of the Ethiopian and Eritrean defense forces from the capital, Mekelle, and other parts of the region, while Western Tigray remains under the control of the Amhara Region. The consequences of the unfolding situation on humanitarian operations in Tigray remain fluid. The breakdown of essential services such as the blackout of electricity, telecommunications, and internet throughout Tigray region will only exacerbate the already dire humanitarian situation. Reported shortages of cash and fuel in the region can compromise the duty of care of aid workers on the ground. Despite the dynamic and uncertain situation, partners report that the security situation in Tigray has been generally calm over the past few days, with limited humanitarian activities being implemented around Mekelle and Shire. Key developments On 28 June, the Federal Government agreed to the request from the Interim Regional Administration in Tigray for a "unilateral ceasefire, until the farming season ends." Subsequently, Ethiopia National Defense Forces (ENDF) withdrew from Mekelle and other main towns in the region, including Shire, Axum, Adwa, and Adigrat. Currently, former Tigray Defense Forces (TDF) are in control of the main cities and roads in Tigray. There were no reports of fighting in Mekelle and other towns. -
![Genotypes for Reaction to Tef Shoot Fly [Atherigona Hyalinipennis Van Emden], at Maysiye, Northern Ethiopia](https://docslib.b-cdn.net/cover/3729/genotypes-for-reaction-to-tef-shoot-fly-atherigona-hyalinipennis-van-emden-at-maysiye-northern-ethiopia-923729.webp)
Genotypes for Reaction to Tef Shoot Fly [Atherigona Hyalinipennis Van Emden], at Maysiye, Northern Ethiopia
Vol. 10(6), pp. 146-152, June 2018 DOI: 10.5897/JPBCS2017.0711 Article Number: AB4F5B556961 ISSN 2006-9758 Copyright © 2018 Journal of Plant Breeding and Crop Author(s) retain the copyright of this article http://www.academicjournals.org/JPBCS Science Full Length Research Paper Genetic variation of tef [Eragrostis tef (Zucc.) Trotter] genotypes for reaction to tef shoot fly [Atherigona hyalinipennis Van Emden], at Maysiye, Northern Ethiopia Chekole Nigus Tigray Agricultural Research Institute, Axum Center, P. O. Box. 230, Axum, Ethiopia. Received 24 November, 2017; Accepted 29 January, 2018 One of the major biotic stresses that limits tef yield is insect pests attack. Of these tef, shoot fly is sporadically important insect pest in various tef growing areas of Ethiopia. Evaluation of diversity of tef germplasm in Ethiopia for the reaction tef shoot fly might give a chance to get host plant resistance. The main objective of this study was to assess the genetic variation among tef genotypes for their reaction to tef shoot fly. Field experiment was conducted in 2015 cropping season at Maysiye, Northern Ethiopia. The genotypes were planted in triple lattice design with three replications category of reaction of the tested tef genotypes for their reaction to shoot fly attack was adopted from the rating scale of the IRRI for rice. The study revealed that acc. 17 WJ was found to be the only genotype evaluated as resistant to tef shoot fly Atherigona hyalinipennis species. While the standard checks Quncho and Kora were grouped under the susceptible category, generally 10 tef genotypes were moderately resistance, 19 genotypes were moderately susceptible, 16 genotypes were susceptible, and three genotypes were highly susceptible to tef shoot fly attack. -

Journal of Ethnobiology and Ethnomedicine
Journal of Ethnobiology and Ethnomedicine This Provisional PDF corresponds to the article as it appeared upon acceptance. Fully formatted PDF and full text (HTML) versions will be made available soon. An ethnobotanical study of medicinal plants used in Kilte Awulaelo District, Tigray Region of Ethiopia Journal of Ethnobiology and Ethnomedicine 2013, 9:65 doi:10.1186/1746-4269-9-65 Abraha Teklay ([email protected]) Balcha Abera ([email protected]) Mirutse Giday ([email protected]) ISSN 1746-4269 Article type Research Submission date 12 March 2013 Acceptance date 4 September 2013 Publication date 8 September 2013 Article URL http://www.ethnobiomed.com/content/9/1/65 This peer-reviewed article can be downloaded, printed and distributed freely for any purposes (see copyright notice below). Articles in Journal of Ethnobiology and Ethnomedicine are listed in PubMed and archived at PubMed Central. For information about publishing your research in Journal of Ethnobiology and Ethnomedicine or any BioMed Central journal, go to http://www.ethnobiomed.com/authors/instructions/ For information about other BioMed Central publications go to http://www.biomedcentral.com/ © 2013 Teklay et al. This is an open access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. An ethnobotanical study of medicinal plants used in Kilte Awulaelo District, Tigray -

ETHIOPIA 22 February 2021 the Pre-Crisis Situation in Tigray PURPOSE and SCOPE
Secondary Data Review ETHIOPIA 22 February 2021 The Pre-crisis situation in Tigray PURPOSE AND SCOPE This report provides baseline, background, and context information on the Tigray region, refer- ring to the situation before the beginning of the conflict that erupted in November 2020. It was compiled to help inform the humanitarian response. OVERVIEW Population: Tigray has an estimated population of nearly 5.7 million people (5.5% of the to- tal population of Ethiopia), predominantly rural, although recent years have seen rapid urba- nisation. Tigrayans constitute the majority ethnic group. Half of the population is under 18 years old. In October 2020, Tigray was hosting over 100,000 IDPs, primarily from Amhara and Oromia regions, and over 5,500 returnee IDPs, as well as more than 95,000 refugees, predomi- nantly from Eritrea, mostly hosted in four camps. Politics & economy: The Tigrayan political elites have played a dominant role in Ethiopia’s po- litics since 1994. This is partly responsible for significant economic growth in the region, with relatively high levels of investment and strong local government capacity. However, Tigray continues to have the highest poverty rate in the country. Humanitarian concerns: Tigray’s economy and livelihoods, centred around agriculture, are highly dependent on rainfall, with some parts of Tigray experiencing only one rainy season per Source: UNOCHA 25/01/2021 year. A decrease in rainfall and increase in the occurrence of droughts due to climate change COVID-19: More than 6,300 cases of COVID-19 had been registered in Tigray until October has had a significant impact on livelihoods and food security in the region. -

Ethiopia: Access
ETHIOPIA Access Map - Tigray Region As of 31 May 2021 ERITREA Ethiopia Adi Hageray Seyemti Egela Zala Ambesa Dawuhan Adi Hageray Adyabo Gerhu Sernay Gulo Mekeda Erob Adi Nebried Sheraro Rama Ahsea Tahtay Fatsi Eastern Tahtay Adiyabo Chila Rama Adi Daero Koraro Aheferom Saesie Humera Chila Bzet Adigrat Laelay Adiabo Inticho Tahtay Selekleka Laelay Ganta SUDAN Adwa Edaga Hamus Koraro Maychew Feresmay Afeshum Kafta Humera North Western Wukro Adwa Hahayle Selekleka Akxum Nebelat Tsaeda Emba Shire Embaseneyti Frewoyni Asgede Tahtay Edaga Arbi Mayechew Endabaguna Central Hawzen Atsbi May Kadra Zana Mayknetal Korarit TIGRAY Naeder Endafelasi Hawzen Kelete Western Zana Semema Awelallo Tsimbla Atsibi Adet Adi Remets Keyhe tekli Geraleta Welkait Wukro May Gaba Dima Degua Tsegede Temben Dima Kola Temben Agulae Awra Tselemti Abi Adi Hagere May Tsebri Selam Dansha Tanqua Dansha Melashe Mekelle Tsegede Ketema Nigus Abergele AFAR Saharti Enderta Gijet AMHARA Mearay South Eastern Adi Gudom Hintalo Samre Hiwane Samre Wajirat Selewa Town Accessible areas Emba Alaje Regional Capital Bora Partially accessible areas Maychew Zonal Capital Mokoni Neqsege Endamehoni Raya Azebo Woreda Capital Hard to reach areas Boundary Accessible roads Southern Chercher International Zata Oa Partially accessible roads Korem N Chercher Region Hard to reach roads Alamata Zone Raya Alamata Displacement trends 50 Km Woreda The boundaries and names shown and the designations used on this map do not imply official endorsement or acceptance by the United Nations. Creation date: 31 May 2021 Sources: OCHA, Tigray Statistical Agency, humanitarian partners Feedback: [email protected] http://www.humanitarianresponse.info/operations/ethiopia www.reliefweb.int. -

Mekelle Investment Profile Investment Profile by Meresa Reda Tigray
Mekelle Investment Profile By Meresa Reda Tigray Investment Office I. TIGRAY IN BRIEF II. INVESTMENT PERFORMANCE III. Investment Potentials In Tigray IV. Investment Incentives V. Why Invest In Tigray ?? VI. List of Industrial Projects PartPart--II TIGRAY AT GLA nnCECE Tigray at a glance 44 TigrayTigray…… cont’d Location: Northern tip of Ethiopia between 12 00 --1515 00 north latitude and 36 003030 ’’--4040 003030 ’ east longitude Area: 53,638 km 22 Population: 4.45 millions as of census 2007 7 zones, 47 Woredas & 673 Kebeles Altitude: 500500--39353935 meters above sea level Agro Ecology: 11.5% temperate ((DegaDega)) 40.5% subtropical ((WoinedegaWoinedega)) 48% Tropical (Kola) 55 TigrayTigray…… cont’d Economy: Predominantly Agriculture The contribution of Agriculture, Industry and Service sector to the regional GDP is 46.75%, 18.89%, 34.36% respectively. (2006/7) Rainfall :: the annual average rainfall is between 650650--980980 mm 66 PartPart--IIII INVESTMENT PERFORMANCE SO FAR Job opportunity 2869 existing Above 100,000 projects permanent and 29%agriculture >>88,824 Temporary 20% construction Capital 14% Hotel & tourism 32.3 billion birr 30% industry 0.01 Real estate 0.07 social servic ee No of Projects 1600 1400 1200 1000 800 No of Projects 600 400 200 0 1984 1985-1990 1991-1995 1996-2000 2001-2003 PartPart--IIIIII Investment Potentials In Tigray •• Economy of the region is based on agriculture •• The region is suitable for crops such as sorghum, sesame, cotton, barley, wheat , teff,teff , and the likes Agriculture About 20,000 and, 100,000 hectares of land is suitable for wild gum and incense The region has wide opportunities for the livestock development.