The Effect of Bromepheniramine on Cough Sensitivity in Normal Volunteers
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Guidelines for the Forensic Analysis of Drugs Facilitating Sexual Assault and Other Criminal Acts
Vienna International Centre, PO Box 500, 1400 Vienna, Austria Tel.: (+43-1) 26060-0, Fax: (+43-1) 26060-5866, www.unodc.org Guidelines for the Forensic analysis of drugs facilitating sexual assault and other criminal acts United Nations publication Printed in Austria ST/NAR/45 *1186331*V.11-86331—December 2011 —300 Photo credits: UNODC Photo Library, iStock.com/Abel Mitja Varela Laboratory and Scientific Section UNITED NATIONS OFFICE ON DRUGS AND CRIME Vienna Guidelines for the forensic analysis of drugs facilitating sexual assault and other criminal acts UNITED NATIONS New York, 2011 ST/NAR/45 © United Nations, December 2011. All rights reserved. The designations employed and the presentation of material in this publication do not imply the expression of any opinion whatsoever on the part of the Secretariat of the United Nations concerning the legal status of any country, territory, city or area, or of its authorities, or concerning the delimitation of its frontiers or boundaries. This publication has not been formally edited. Publishing production: English, Publishing and Library Section, United Nations Office at Vienna. List of abbreviations . v Acknowledgements .......................................... vii 1. Introduction............................................. 1 1.1. Background ........................................ 1 1.2. Purpose and scope of the manual ...................... 2 2. Investigative and analytical challenges ....................... 5 3 Evidence collection ...................................... 9 3.1. Evidence collection kits .............................. 9 3.2. Sample transfer and storage........................... 10 3.3. Biological samples and sampling ...................... 11 3.4. Other samples ...................................... 12 4. Analytical considerations .................................. 13 4.1. Substances encountered in DFSA and other DFC cases .... 13 4.2. Procedures and analytical strategy...................... 14 4.3. Analytical methodology .............................. 15 4.4. -

MSM Cross Reference Antihistamine Decongestant 20100701 Final Posted
MISSISSIPPI DIVISION OF MEDICAID Antihistamine/Decongestant Product and Active Ingredient Cross-Reference List The agents listed below are the antihistamine/decongestant drug products listed in the Mississippi Medicaid Preferred Drug List (PDL). This is a cross-reference between the drug product name and its active ingredients to reference the antihistamine/decongestant portion of the PDL. For more information concerning the PDL, including non- preferred agents, the OTC formulary, and other specifics, please visit our website at www.medicaid.ms.gov. List Effective 07/16/10 Therapeutic Class Active Ingredients Preferred Non-Preferred ANTIHISTAMINES - 1ST GENERATION BROMPHENIRAMINE MALEATE BPM BROMAX BROMPHENIRAMINE MALEATE J-TAN PD BROMSPIRO LODRANE 24 LOHIST 12HR VAZOL BROMPHENIRAMINE TANNATE BROMPHENIRAMINE TANNATE J-TAN P-TEX BROMPHENIRAMINE/DIPHENHYDRAM ALA-HIST CARBINOXAMINE MALEATE CARBINOXAMINE MALEATE PALGIC CHLORPHENIRAMINE MALEATE CHLORPHENIRAMINE MALEATE CPM 12 CHLORPHENIRAMINE TANNATE ED CHLORPED ED-CHLOR-TAN MYCI CHLOR-TAN MYCI CHLORPED PEDIAPHYL TANAHIST-PD CLEMASTINE FUMARATE CLEMASTINE FUMARATE CYPROHEPTADINE HCL CYPROHEPTADINE HCL DEXCHLORPHENIRAMINE MALEATE DEXCHLORPHENIRAMINE MALEATE DIPHENHYDRAMINE HCL ALLERGY MEDICINE ALLERGY RELIEF BANOPHEN BENADRYL BENADRYL ALLERGY CHILDREN'S ALLERGY CHILDREN'S COLD & ALLERGY COMPLETE ALLERGY DIPHEDRYL DIPHENDRYL DIPHENHIST DIPHENHYDRAMINE HCL DYTUSS GENAHIST HYDRAMINE MEDI-PHEDRYL PHARBEDRYL Q-DRYL QUENALIN SILADRYL SILPHEN DIPHENHYDRAMINE TANNATE DIPHENMAX DOXYLAMINE SUCCINATE -

Brompheniramine Maleate, Pseudoephedrine Hydrochloride
BROMPHENIRAMINE MALEATE, PSEUDOEPHEDRINE HYDROCHLORIDE, AND DEXTROMETHORPHAN HYDROBROMIDE- brompheniramine maleate, pseudoephedrine hydrochloride, and dextromethorphan hydrobromide syrup Morton Grove Pharmaceuticals, Inc. ---------- Brompheniramine Maleate, Pseudoephedrine Hydrochloride, and Dextromethorphan Hydrobromide Oral Syrup 2 mg/30 mg/10 mg per 5 mL Rx only DESCRIPTION Brompheniramine Maleate, Pseudoephedrine Hydrochloride and Dextromethorphan Hydrobromide Oral Syrup is a clear, light pink syrup with a butterscotch flavor. Each 5 mL (1 teaspoonful) contains: Brompheniramine Maleate, USP 2 mg Pseudoephedrine Hydrochloride, USP 30 mg Dextromethorphan Hydrobromide, USP 10 mg Alcohol 0.95% v/v In a palatable, aromatic vehicle. Inactive Ingredients: artificial butterscotch flavor, citric acid anhydrous, dehydrated alcohol, FD&C Red No. 40, glycerin, liquid sugar, methylparaben, propylene glycol, purified water and sodium benzoate. It may contain 10% citric acid solution or 10% sodium citrate solution for pH adjustment. The pH range is between 3.0 and 6.0. C16H19BrN2·C4H4O4 M.W. 435.31 Brompheniramine Maleate, USP (±)-2-p-Bromo-α-2-(dimethylamino)ethylbenzylpyridine maleate (1:1) C10H15NO · HCl M.W. 201.69 Pseudoephedrine Hydrochloride, USP (+)-Pseudoephedrine hydrochloride C18H25NO · HBr · H2O M.W. 370.32 Dextromethorphan Hydrobromide, USP 3-Methoxy-17-methyl-9α, 13α, 14α -morphinan hydrobromide monohydrate Antihistamine/Nasal Decongestant/Antitussive syrup for oral administration. CLINICAL PHARMACOLOGY Brompheniramine maleate is a -

Title 16. Crimes and Offenses Chapter 13. Controlled Substances Article 1
TITLE 16. CRIMES AND OFFENSES CHAPTER 13. CONTROLLED SUBSTANCES ARTICLE 1. GENERAL PROVISIONS § 16-13-1. Drug related objects (a) As used in this Code section, the term: (1) "Controlled substance" shall have the same meaning as defined in Article 2 of this chapter, relating to controlled substances. For the purposes of this Code section, the term "controlled substance" shall include marijuana as defined by paragraph (16) of Code Section 16-13-21. (2) "Dangerous drug" shall have the same meaning as defined in Article 3 of this chapter, relating to dangerous drugs. (3) "Drug related object" means any machine, instrument, tool, equipment, contrivance, or device which an average person would reasonably conclude is intended to be used for one or more of the following purposes: (A) To introduce into the human body any dangerous drug or controlled substance under circumstances in violation of the laws of this state; (B) To enhance the effect on the human body of any dangerous drug or controlled substance under circumstances in violation of the laws of this state; (C) To conceal any quantity of any dangerous drug or controlled substance under circumstances in violation of the laws of this state; or (D) To test the strength, effectiveness, or purity of any dangerous drug or controlled substance under circumstances in violation of the laws of this state. (4) "Knowingly" means having general knowledge that a machine, instrument, tool, item of equipment, contrivance, or device is a drug related object or having reasonable grounds to believe that any such object is or may, to an average person, appear to be a drug related object. -

Antihistamine Therapy in Allergic Rhinitis
CLINICAL REVIEW Antihistamine Therapy in Allergic Rhinitis Paul R. Tarnasky, MD, and Paul P. Van Arsdel, Jr, MD Seattle, Washington Allergic rhinitis is a common disorder that is associated with a high incidence of mor bidity and considerable costs. The symptoms of allergic rhinitis are primarily depen dent upon the tissue effects of histamine. Antihistamines are the mainstay of therapy for allergic rhinitis. Recently, a second generation of antihistamines has become available. These agents lack the adverse effect of sedation, which is commonly associated with older antihistamines. Current practice of antihistamine therapy in allergic rhinitis often involves random selection among the various agents. Based upon the available clinical trials, chlorpheniramine appears to be the most reasonable initial antihistaminic agent. A nonsedating antihis tamine should be used initially if a patient is involved in activities where drowsiness is dangerous. In this comprehensive review of allergic rhinitis and its treatment, the cur rent as well as future options in antihistamine pharmacotherapy are emphasized. J Fam Pract 1990; 30:71-80. llergic rhinitis is a common condition afflicting some defined by the period of exposure to those agents to which A where between 15 and 30 million people in the United a patient is sensitive. Allergens in seasonal allergic rhinitis States.1-3 The prevalence of disease among adolescents is consist of pollens from nonflowering plants such as trees, estimated to be 20% to 30%. Two thirds of the adult grasses, and weeds. These pollens generally create symp allergic rhinitis patients are under 30 years of age.4-6 Con toms in early spring, late spring through early summer, sequently, considerable costs are incurred in days lost and fall, respectively. -
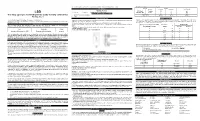
(LSD) Test Dip Card (Urine) • Specimen Collection Container % Agreement 98.8% 99
frozen and stored below -20°C. Frozen specimens should be thawed and mixed before testing. GC/MS. The following results were tabulated: Method GC/MS MATERIALS Total Results Results Positive Negative Materials Provided LSD Rapid Positive 79 1 80 LSD • Test device • Desiccants • Package insert • Urine cups Test Dip card Negative 1 99 100 Materials Required But Not Provided Total Results 80 100 180 One Step Lysergic acid diethylamide (LSD) Test Dip card (Urine) • Specimen collection container % Agreement 98.8% 99. % 98.9% • Timer Package Insert DIRECTIONS FOR USE Analytical Sensitivity This Instruction Sheet is for testing of Lysergic acid diethylamide. Allow the test device, and urine specimen to come to room temperature [15-30°C (59-86°F)] prior to testing. A drug-free urine pool was spiked with LSD at the following concentrations: 0 ng/mL, -50%cutoff, -25%cutoff, cutoff, A rapid, one step test for the qualitative detection of Lysergic acid diethylamide and its metabolites in human urine. 1) Remove the test device from the foil pouch. +25%cutoff and +50%cutoff. The result demonstrates >99% accuracy at 50% above and 50% below the cut-off For forensic use only. 2) Remove the cap from the test device. Label the device with patient or control identifications. concentration. The data are summarized below: INTENDED USE 3) Immerse the absorbent tip into the urine sample for 10-15 seconds. Urine sample should not touch the plastic Lysergic acid diethylamide (LSD) Percent of Visual Result The One Step Lysergic acid diethylamide (LSD) Test Dip card (Urine) is a lateral flow chromatographic device. -

Medicines Classification Committee
Medicines Classification Committee Meeting date 1 May 2017 58th Meeting Title Reclassification of Sedating Antihistamines Medsafe Pharmacovigilance Submitted by Paper type For decision Team Proposal for The Medicines Adverse Reactions Committee (MARC) recommended that the reclassification to committee consider reclassifying sedating antihistamines to prescription prescription medicines when used in children under 6 years of age for the treatment of medicine for some nausea and vomiting and travel sickness [exact wording to be determined by indications the committee]. Reason for The purpose of this document is to provide the committee with an overview submission of the information provided to the MARC about safety concerns associated with sedating antihistamines and reasons for recommendations. Associated March 2013 Children and Sedating Antihistamines Prescriber Update articles February 2010 Cough and cold medicines clarification – antihistamines Medsafe website Safety information: Use of cough and cold medicines in children – new advice Medicines for Alimemazine Diphenhydramine consideration Brompheniramine Doxylamine Chlorpheniramine Meclozine Cyclizine Promethazine Dexchlorpheniramine New Zealand Some oral sedating antihistamines available without exposure to a prescription (pharmacist-only and pharmacy only), sedating therefore usage data is not easily available. antihistamines Table of Contents 1.0 PURPOSE ...................................................................................................................................... -

Evaluation of the ACQUITY UPLC H-Class System With
[ TECHNOLOGY BRIEF ] Evaluation of the ACQUITY UPLC H-Class System with ACQUITY QDa Mass Detector for the Determination of Amphetamine, Methamphetamine, Ketamine, and Norketamine in Human Urine for Forensic Toxicology Nayan S. Mistry, Rob Lee, and Michelle Wood Waters Corporation, Wilmslow, UK The ACQUITY QDa Mass Detector has demonstrated great promise as an alternative technique to immunoassay. GOAL To assess the feasibility of using the Waters™ ACQUITY™ UPLC™ H-Class System with the ACQUITY QDa™ Mass Detector (Figure 1) as an alternate technique to immunoassay for illicit drug analysis and quantification. BACKGROUND Amphetamines (methamphetamine and amphetamine) are among the most commonly abused illicit substances in the world. In 2016, it was estimated that around 35 million adults worldwide used amphetamines.¹ The region with the highest annual use was North America at Figure 1. The ACQUITY UPLC H-Class System and ACQUITY QDa Mass Detector. approximately 2% of the population. In the last few years however, there also appears Forensic laboratories often utilize immunoassay for routine urine analysis. to be a marked increase in consumption While the technique is rapid and simple, there can be some disadvantages, within other geographies, particularly often associated with poor selectivity for example, false positive results for East and Southeast Asia, where the amphetamine or ketamine have been reported for a variety of substances.3-5 amphetamines have been identified as As most positive immunoassay results require a confirmatory test (such as one of the most worrying threats of drug GC or LC-MS), the consequence of false positive identifications, as a result use. Moreover, a rise in the use of Ecstasy of poor assay selectivity, can significantly compromise laboratory efficiency. -

UQ272429 OA.Pdf
Cochrane Database of Systematic Reviews Oral antihistamine-decongestant-analgesic combinations for the common cold (Review) De Sutter AIM, van Driel ML, Kumar AA, Lesslar O, Skrt A De Sutter AIM, van Driel ML, Kumar AA, Lesslar O, Skrt A. Oral antihistamine-decongestant-analgesic combinations for the common cold. Cochrane Database of Systematic Reviews 2012, Issue 2. Art. No.: CD004976. DOI: 10.1002/14651858.CD004976.pub3. www.cochranelibrary.com Oral antihistamine-decongestant-analgesic combinations for the common cold (Review) Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd. TABLE OF CONTENTS HEADER....................................... 1 ABSTRACT ...................................... 1 PLAINLANGUAGESUMMARY . 2 BACKGROUND .................................... 3 OBJECTIVES ..................................... 3 METHODS ...................................... 4 RESULTS....................................... 5 Figure1. ..................................... 7 Figure2. ..................................... 8 DISCUSSION ..................................... 19 AUTHORS’CONCLUSIONS . 20 ACKNOWLEDGEMENTS . 20 REFERENCES ..................................... 21 CHARACTERISTICSOFSTUDIES . 24 DATAANDANALYSES. 64 Analysis 1.1. Comparison 1 Combination 1: Antihistamine-decongestant, Outcome 1 Global evaluation. 66 Analysis 1.2. Comparison 1 Combination 1: Antihistamine-decongestant, Outcome 2 Side effects: all - Combination 1: Antihistamine-decongestant. 67 Analysis 1.3. Comparison 1 Combination 1: Antihistamine-decongestant, -

Could Antihistamines Help in the Treatment and Spread of COVID-19 Via Re-Modulating Cytokines and by Reducing Sneezing?
ACTA SCIENTIFIC NUTRITIONAL HEALTH (ISSN:2582-1423) Volume 4 Issue 4 April 2020 Short Communication Could Antihistamines Help in the Treatment and Spread of COVID-19 Via Re-Modulating Cytokines and by Reducing Sneezing? 1 2 Suna Aydin and Suleyman Aydin * Received: March 20, 2020 1Department of Cardiovascular Surgery, Elazig Fethi Sekin City Hospital, Health Sci- Published: March 27, 2020 ence University, Elazig Campus, Turkey © All rights are reserved by Suna Aydin and 2Department of Medical Biochemistry and Clinical Biochemistry, Medical School, Firat Suleyman Aydin. University, Turkey *Corresponding Author: Suleyman Aydin, Department of Medical Biochemistry and Clinical Biochemistry, Medical School, Firat University, Turkey. E-mail: [email protected] Keywords: COVID-19; Interferon-gamma; Antihistamine; Public Health; Cytokine Coronaviruses are a large family of viruses [1]. The latest mem- ber of this family is termed the SARS-Cov-2 which causes COVID-19 the virus (COVID-19). Antihistamines can exert indirect antiviral etc.) so producing more IFN-γ and controlling the replication of [2]. Outbreaks of SARS-Cov-2 are now pandemic, given the toll of effects on infected cells and neighboring cells and can control anti- infections worldwide and the Covid-19 associated death rate [3]. viral properties by modulating IL-1, IL-2, TNF, and especially IFN-γ. knowing what to do to control COVID-19. No vaccine is currently to an antihistamine supply may have strong antiviral effects for CO- All governments have been taken by surprise and have difficulty in The depletion of IL-10, and then the over production of IFN-γ due available against the virus. -

Brompheniramine Maleate | Medchemexpress
Inhibitors Product Data Sheet Brompheniramine maleate • Agonists Cat. No.: HY-B0480 CAS No.: 980-71-2 Molecular Formula: C₂₀H₂₃BrN₂O₄ • Molecular Weight: 435.31 Screening Libraries Target: Histamine Receptor Pathway: GPCR/G Protein; Immunology/Inflammation; Neuronal Signaling Storage: Powder -20°C 3 years 4°C 2 years In solvent -80°C 6 months -20°C 1 month SOLVENT & SOLUBILITY In Vitro DMSO : 100 mg/mL (229.72 mM; Need ultrasonic) H2O : 100 mg/mL (229.72 mM; Need ultrasonic) Mass Solvent 1 mg 5 mg 10 mg Concentration Preparing 1 mM 2.2972 mL 11.4861 mL 22.9721 mL Stock Solutions 5 mM 0.4594 mL 2.2972 mL 4.5944 mL 10 mM 0.2297 mL 1.1486 mL 2.2972 mL Please refer to the solubility information to select the appropriate solvent. In Vivo 1. Add each solvent one by one: 10% DMSO >> 40% PEG300 >> 5% Tween-80 >> 45% saline Solubility: ≥ 2.5 mg/mL (5.74 mM); Clear solution 2. Add each solvent one by one: 10% DMSO >> 90% (20% SBE-β-CD in saline) Solubility: ≥ 2.5 mg/mL (5.74 mM); Clear solution 3. Add each solvent one by one: 10% DMSO >> 90% corn oil Solubility: ≥ 2.5 mg/mL (5.74 mM); Clear solution BIOLOGICAL ACTIVITY Description Brompheniramine ((±)-Brompheniramine) maleate is a potent and orally active antihistamine of the propylamine class. Brompheniramine maleate is a selective histamine H1 receptor antagonist with a Kd of 6.06 nM. Brompheniramine maleate has anticholinergic, antidepressant and analgesia properties and can be used for allergic rhinitis research[1][2]. -

Brompheniramine Maleate: Summary Report
Brompheniramine maleate: Summary Report Item Type Report Authors Yuen, Melissa V.; Gianturco, Stephanie L.; Pavlech, Laura L.; Storm, Kathena D.; Yoon, SeJeong; Mattingly, Ashlee N. Publication Date 2020-11 Keywords Brompheniramine; Compounding; Food, Drug and Cosmetic Act; Food, Drug and Cosmetic Act, Section 503B; Food and Drug Administration; Outsourcing facility; Drug compounding; Legislation, Drug; United States Food and Drug Administration Rights Attribution-NoDerivatives 4.0 International Download date 02/10/2021 22:26:51 Item License http://creativecommons.org/licenses/by-nd/4.0/ Link to Item http://hdl.handle.net/10713/14918 Summary Report Brompheniramine maleate Prepared for: Food and Drug Administration Clinical use of bulk drug substances nominated for inclusion on the 503B Bulks List Grant number: 5U01FD005946 Prepared by: University of Maryland Center of Excellence in Regulatory Science and Innovation (M-CERSI) University of Maryland School of Pharmacy November 2020 This report was supported by the Food and Drug Administration (FDA) of the U.S. Department of Health and Human Services (HHS) as part of a financial assistance award (U01FD005946) totaling $2,342,364, with 100 percent funded by the FDA/HHS. The contents are those of the authors and do not necessarily represent the official views of, nor an endorsement by, the FDA/HHS or the U.S. Government. 1 Table of Contents INTRODUCTION ........................................................................................................................................ 5