Inquest Finding (PDF)
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Metropolitan Health Service Annual Report 2015-16
Overview of agency < 1 > Vision statement Vision Priorities To deliver a safe, high quality, sustainable health system for all Western Australians. Our strategic priorities are focused on a continuum of care to support and guide health care through integrated service delivery from prevention and health promotion, early Values intervention, primary care through to diagnosis, treatment, rehabilitation and palliation. Ensuring people in Western Australia receive safe, high quality and accessible health WA Health’s Code of Conduct identifies the values that we hold as fundamental in our work services underpins our strategic priorities. This includes delivering health services that are and describes how these values translate into action. patient centred, based on evidence and within a culture of continuous improvement. Our values are: WA Health’s strategic priorities are: 1. Prevention and Community Care Services Quality Care 2. Health Services 3. Chronic Disease Services 4. Aboriginal Health Services. Respect Excellence Integrity Teamwork Leadership < 2 > Executive summary The 2015–16 financial year marked the end of an era for WA Health, as the health system Information and Communications Technology (ICT) service delivery was also improved with made preparations to move away from a centralised governance structure and embrace a the upgrade of more than 90 per cent of WA Health’s computer fleet and the establishment devolved structure as of 1 July 2016. of an Incident Management Triage team to provide a 24-hour a day, seven-day-a-week, on-call facility for hospital staff requiring assistance with an ICT issue. Guided by the WA Health Reform Program 2015–2020, WA Health spent 2015–16 planning for the transition to the new governance arrangements, which will support the ongoing Roll-out of core clinical applications continued and the Psychiatric Online Information System sustainability and performance of the health system, and make it more responsive to was upgraded to support the implementation of changes to the Mental Health Act 2014. -

Better Choices. Better Lives. WESTERN AUSTRALIAN MENTAL HEALTH, ALCOHOL and OTHER DRUG SERVICES PLAN 2015–2025
Better Choices. Better Lives. WESTERN AUSTRALIAN MENTAL HEALTH, ALCOHOL AND OTHER DRUG SERVICES PLAN 2015–2025 cover form, see other file © 2015 State of Western Australia You may copy, distribute, display, download and otherwise freely deal with this work for any purpose, provided that you attribute the Mental Health Commission of Western Australia as the owner. However, you must obtain permission if you wish to (a) charge others for access to the work (other than at cost), (b) include the work in advertising or product for sale, (c) modify the work or (d) publish the work to a website. This document is available on our website: www.mhc.wa.gov.au ISBN: 978-0-9944434-0-3 This document may be cited as: Western Australian Mental Health Commission (2015). Better Choices. Better Lives. Western Australian Mental Health, Alcohol and Other Drug Services Plan 2015–2025. Perth, Western Australian Mental Health Commission. Western Australian Mental Health, Alcohol and Other Drug Services Plan 2015–2025 1 CONTENTS Overview ........................................................................................................................6 Guiding principles and what we hope to achieve .....................................................10 Consultation ................................................................................................................13 The need for change ...................................................................................................16 Age appropriate services across the service spectrum ..........................................24 -

Register of Authorised Hospitals in Western Australia
Register of Authorised Hospitals in Western Australia Mental Health Act 2014 Section 542 Correct as of 4 August 2020 (OCP23859) www.chiefpsychiatrist.wa.gov.au Introduction Section 542 of the Mental Health Act 2014 provides for the Governor, by order published in the Western Australian Government Gazette to authorise a public hospital or part of a public hospital to be an ‘authorised hospital’ for the purposes of reception and admission of patients requiring involuntary treatment and care. Section 541 provides for a private hospital whose license is endorsed under section 26DA(2) of the Hospitals and Health Services Act 1927 to be an ‘authorised hospital’ on the recommendation by/of the Chief Psychiatrist, for the reception and admission of patients requiring involuntary treatment and care. Please Note: Grant of Leave under section 105(1)(a)(ii) of the Mental Health Act 2014 from an Authorised part of a Hospital to a Non-Authorised part of a Hospital Subdivision 2 of Division 6 of Part 7 of the Mental Health Act 2014 provides for the granting of leave for an involuntary detained patient from an authorised hospital. Section 105 (1)(a)(ii) provides specifically for leave to be granted to a General Hospital for a patient who requires medical or surgical treatment or treatment likely to benefit the inpatient’s physical health in some other way. When an authorised hospital is within a general hospital campus and an involuntary inpatient needs to be treated in the general part of the hospital it is as though it is leave being granted from the authorised facility to the general hospital, despite the fact that both hospitals (authorised and general) are within the same grounds. -
Published List of Authorised Disposers
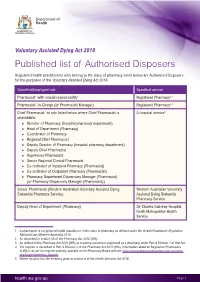
Voluntary Assisted Dying Act 2019 Published list of Authorised Disposers Registered health practitioners who belong to the class of pharmacy listed below are Authorised Disposers for the purposes of the Voluntary Assisted Dying Act 2019. Specified/Employed role Specified service Pharmacist1 with overall responsibility2 Registered Pharmacy3,4 Pharmacist1-in-Charge (or Pharmacist Manager) Registered Pharmacy3,4 Chief Pharmacist1 or role listed below where Chief Pharmacist is A hospital service5 unavailable: * Director of Pharmacy (hospital pharmacy department) * Head of Department (Pharmacy) * Coordinator of Pharmacy * Regional Chief Pharmacist * Deputy Director of Pharmacy (hospital pharmacy department) * Deputy Chief Pharmacist * Supervisor Pharmacist * Senior Regional Clinical Pharmacist * Co-ordinator of Inpatient Pharmacy (Pharmacist) * Co-ordinator of Outpatient Pharmacy (Pharmacist) * Pharmacy Department Dispensary Manager (Pharmacist) (or Pharmacy Dispensary Manager (Pharmacist)) Senior Pharmacist (Western Australian Voluntary Assisted Dying Western Australian Voluntary Statewide Pharmacy Service) Assisted Dying Statewide Pharmacy Service Deputy Head of Department (Pharmacy) Sir Charles Gairdner Hospital, North Metropolitan Health Service 1 A pharmacist is a registered health practitioner in the class of pharmacy as defined under the Health Practitioner Regulation National Law (Western Australia) 2010 2 As described in section 56 of the Pharmacy Act 2010 (WA) 3 As defined in the Pharmacy Act 2010 (WA) as meaning a premises registered -

Graylands: the Evolution of a Suburb
GRAYLANDS: THE EVOLUTION OF A SUBURB PAMELA MIKUS Bachelor of Arts in History STATEMENT OF PRESENTATION This thesis is presented as part of the requirements for the Honours degree of Bachelor of Arts in History at Murdoch University 2013 I declare that this is my own account of my research i COPYRIGHT ACKNOWLEDGMENT I acknowledge that a copy of this thesis will be held at the Murdoch University Library. I understand that, under the provisions of s51.2 of the Copyright Act 1968, all or part of this thesis may be copied without infringement of copyright where such a reproduction is for the purposes of study and research. This statement does not signal any transfer of copyright away from the author. Signed: …………………………………………………………... Full Name of Degree: BACHELOR OF ARTS IN HISTORY WITH HONOURS Thesis Title: GRAYLANDS: THE EVOLUTION OF A SUBURB Author: PAM MIKUS Year: 2013 ii ABSTRACT ‘Where is this Graylands?’ A journalist posed this question in 1950 and answered by pointing out that the bus company misspelled the name as Greylands; the postal address was Claremont; the railway station was Karrakatta; and the area fell under the Nedlands Road Board. This thesis endeavours to answer the question by describing the unrecognised importance of this small, seemingly inconsequential locality and explaining themes relevant to its history. The original colonial owners of land in this area were pioneers in the mid-nineteenth century. The first, Captain Harding, bequeathed it to his wife and it was eventually owned by her sister, Maria Gray, who gave her name to the suburb. However, although Graylands was recognised locally as a name from 1896 when land sales began, only a road was gazetted in 1902 until the postal district was recognised in 1959. -

Resident Medical Officer Streams
Royal Perth Bentley Group Resident Medical Officer Streams Accelerate your career with Royal Perth Bentley Group (RPBG) With an established international reputation for contribution to healthcare, training and research as well as the provision of extensive, tailored career opportunities, RPBG provides an ideal launch pad for your career in the medical profession. RPBG is keenly invested in the personal and professional progression of its staff and their engagement in strategic organisational decisions. With support and active engagement from the medical wellbeing program and peer support services, as well as tailored streams of clinical rotations that provide JMOs with the necessary skills and experience to pursue their desired Key reasons you should career pathway. work for RPBG The streams in the Resident Medical Officer Defined streams of medical rotations tailored program are outlined overleaf, covering rotations to provide doctors with the necessary skills at Royal Perth Hospital, Bentley Health Service, and experience to progress down intended Armadale Health Service, Kalgoorlie Hospital, career pathways. Bunbury Regional Hospital and Hedland Health Expanding medical wellbeing program and Campus, and specialised rotations within the peer support systems. Perth Metropolitan area (SJOG Midland Hospital, Mount Hospital, Perth Children’s Hospital and Opportunities for rotation variations including Joondalup Health Campus). Service Improvement, Perioperative, Anaesthetic ED, Silver Chain and CRP rural rotations. Supportive of part–time/flexible training arrangement negotiations. Doctors have the opportunity to be engaged with the Hospital Executive and Area Board through an active JMO Liasion Committee. More information Postgraduate Medical Education: 9224 7091 Medical Workforce (Recruitment): 9224 1693 MEDICAL STREAM In the medical rotation you will get between one and three terms in an acute/general medicine ward (combination of RPH AMU, AHS General Medicine and SJOG Midland, Medicine Unit), as well as one leave relief or after hours term. -

There Will Be 14 Authorised Mental Health Beds in Broome Regional Resource Centre
US Ie STANDING COMMITTEE ON ESTIMATES AND FINANCIAL OPERATIONS QUESTIONS RELATING TO 2008/09 ONGOING BUDGET ESTIMATES DEPARTMENT OF HEALTH 1. HON. HELEN MORTON MLC ASKED- Page 556 1.1 How many mental health beds will be built in the Broome Regional Resource Centre, and how many will be secured beds? Answer: (1) There will be 14 authorised mental health beds in Broome Regional Resource Centre. (2) There will be three secure beds at Broome Regional Resource Centre. 1.2 What is the Broome Regional Resource Centre, and what will it comprise? Answer: The policy framework for country health services involves a regional network model, based on the concepts of service integration and strategic partnership. The regional network model has five interrelated elements, as follows: Regional Resource Centres. Integrated district health services. Health services for towns. Health services for small communities/settlements. Partner metropolitan health service(s). As the largest town in the Kimberley region, Broome has been identified as the most appropriate town for the regional resource centre. As such, it will provide services and support for the following resident specialist and regional health care programs for the Kimberley: Aged care/rehabilitation. Anaesthetics/high dependency. Dental health. Emergency. General medicine. General surgery. Visiting specialist surgery. Medical imaging. Mental health. Obstetrics. Paediatric. Population health. Estimates and Financial Operations Committee Page 2 1.3 What specific initiatives will the $12.5 million for the redevelopment stage 2 of Kalamunda Hospital be spent on from 2009 until 2013. Answer: Planning for Stage 2 of the Kalamunda Hospital redevelopment has not commenced. Funding of $3.2M has been allocated to the refurbishment of the theatres at Kalamunda Hospital. -

Research Proposal Has Been Approved
The University of Notre Dame Australia ResearchOnline@ND Theses 2016 An investigation of nurse education service models in acute care metropolitan hospitals across Australia Carolyn Keane The University of Notre Dame Australia Follow this and additional works at: http://researchonline.nd.edu.au/theses Part of the Nursing Commons COMMONWEALTH OF AUSTRALIA Copyright Regulations 1969 WARNING The am terial in this communication may be subject to copyright under the Act. Any further copying or communication of this material by you may be the subject of copyright protection under the Act. Do not remove this notice. Publication Details Keane, C. (2016). An investigation of nurse education service models in acute care metropolitan hospitals across Australia (Doctor of Nursing). University of Notre Dame Australia. http://researchonline.nd.edu.au/theses/138 This dissertation/thesis is brought to you by ResearchOnline@ND. It has been accepted for inclusion in Theses by an authorized administrator of ResearchOnline@ND. For more information, please contact [email protected]. Appendices Appendix 1. National Safety and Quality Health Service Standards 276 Appendix 2: UNDA Ethics Approval Letter 277 Appendix 3: SMHS Nursing Research Review Committee Approval Letter Government of Western Australia Department of Health Fremantle Hospital and Health Service 3rd February 2014 Carolyn Keane A/Nursing Director, Corporate Services Fremantle Hospital Professional Doctorate in Nursing student, University of Notre Dame Australia. Professor Selma Alliex Dean of the school of nursing University of Notre Dame Australia. Dear Carolyn and Dr Alliex Project title: An Investigation of Nurse Education Services Models in Acute Care Metropolitan Hospitals across Australia. Thankyou for submitting the above project for review by the South Metro Health Service (SMHS) Nursing Research Review Committee. -

Cancer Care Closer to Home May 2016
Cancer care closer to home May 2016 WA Health has strongly invested in cancer care to support the 11,700 Western Australians diagnosed with cancer every year. The recent opening of Fiona Stanley Hospital and St John of God Midland Public Hospital ensure patients have access to excellent cancer care no matter where they live in the metropolitan area. These services are complemented by existing services at the Comprehensive Cancer Centre at Sir Charles Gairdner Hospital, Royal Perth Hospital, Rockingham General Hospital and Joondalup Health Campus with specialist cancer care at Princess Margaret Hospital and King Edward Memorial Hospital. Fiona Stanley Hospital (FSH) also houses a Comprehensive Cancer Centre which includes 22 consulting/interview rooms for cancer outpatients, a chemotherapy unit, a day therapy unit, a radiation oncology suite, radiation therapy planning and a breast assessment centre. The Cancer Centre has been developed around a private courtyard and features a separate entrance and drop-off area to improve privacy and access for patients and their visitors. What treatment can patients expect? With 80 per cent of FSH's cancer patients treated as outpatients, the cancer service has taken a multidisciplinary approach to treatment. This means several specialties work together, including physicians, radiology, pathology, radiation, medical oncology, nursing, counselling, family support services, and allied health. Patients also have access to services such as physiotherapy, clinical psychology, occupational therapy, social work, pharmacy, dietetics and speech pathology, all in one location. 1 Patients receiving targeted radiation therapies benefit from greatly reduced waiting times and faster treatment with state- of-the- art equipment such as the latest in linear accelerator (linac) technology. -

(Esperance Region) November 2019 Raelene Craft (Including Hopetoun, Norseman & Ravensthorpe) M 0439 276 534 E [email protected]
WA PRIMARY Health Alliance Local Health Service Directory Your local WAPHA contact (Esperance Region) November 2019 Raelene Craft (including Hopetoun, Norseman & Ravensthorpe) M 0439 276 534 E [email protected] General Practitioners - Esperance Hospitals Specialists - Kalgoorlie Phone Fax Phone Fax Specialists (Kalgoorlie Based) Phone Fax Dr Frances Werner – ED Consultant 9080 5888 Banksia Medical Centre 9071 1511 9071 3995 Esperance Health Campus 9079 8000 9079 8077 Dr Rafiq Hemnani – Consultant Physician 9080 5888 Dr Graham Jacobs Ms Margaret Smillie – A/Op Manager Dr Sean George - Consultant Physician 9080 5692 9080 5245 Senior Medical Officer Dr Paddy Glackin – Dr Charles Douglas - Public Health Physician 9080 8200 9080 8201 Esperance Health Campus *Esperance Family Practice 9071 3100 9071 3200 9079 8000 9079 8077 Visiting Specialists (Kalgoorlie) Dr Emma Keeler Dr Nadette Hodge (Visiting Specialists) Dr Graham Furness - Ophthalmologist (GOMED) 9026 1900 9022 8458 Dr Ian Skinner - Orthopaedic Surgeon (GOMED) 9311 4800 - Dr Robyn McIntyre Dr Alex O’Beirne - Orthopaedic Surgeon Dr Mike Davis - Cardiologist Dr Lynette Spooner - Skin Cancer Checks (Collins St.) 9093 1044 9093 2223 Dr Sam Kaiser - Paediatrician Dr Brendan Ricciardo - Orthopaedic * Genpar Medical Services 9071 1956 9071 5105 Perth Shoulder Clinic - (Dr McCallum’s Rooms) 9340 6355 9340 6356 Dr Jackie Scurlock - Paediatrician Professor Mark Thomas - Nephrolgist Dr Andrew Marangou Dr Taya Carter Dr Stephen Wright - Nephrologist (Trinity Medical) 9021 8703 9091 8707 -
Western Australia Emergency Access Target Performance Monthly Report
Western Australia Emergency Access Target Performance Monthly Report February 2019 health.wa.gov.au February 2019 | Western Australia Emergency Access Target Performance Monthly Report What is the WA Emergency Access Target (WEAT)? In February 2016, WA Health system established the WA Emergency Access Target (WEAT) to continue to drive local improvement in patient access to emergency services. This replaced the National Emergency Access Target (NEAT) following the expiry of the Commonwealth National Partnership Agreement on Improving Public Hospital Services in 2015. The WEAT requires 90 per cent of all patients presenting to a hospital emergency department (ED) to be seen and admitted, transferred or discharged within four hours. What hospitals does it cover? Child and Adolescent Health Service (CAHS): Perth Children’s Hospital and Princess Margaret Hospital. East Metropolitan Health Service (EMHS): Royal Perth Hospital, Armadale Health Service and St John of God Midland Public Hospital. North Metropolitan Health Service (NMHS): Sir Charles Gairdner Hospital, King Edward Memorial Hospital and Joondalup Health Campus. South Metropolitan Health Service (SMHS): Fiona Stanley Hospital, Rockingham General Hospital and Peel Health Campus. WA Country Health Service (WACHS): Albany Hospital, Broome Hospital, Bunbury Hospital, Busselton Hospital, Carnarvon Hospital, Derby Hospital, Esperance Hospital, Geraldton Hospital, Hedland Health Campus, Kalgoorlie Hospital, Karratha Health Campus, Kununurra Hospital, Narrogin Hospital and Northam Hospital. Providing the best care All hospitals and Health Service Providers (HSPs) continue to examine and improve processes across the entire patient journey, from ED and the wards through to hospital discharge. In 2017–18, Western Australia was the best performing state for patients treated and admitted, transferred or discharged within four hours. -

LA QON 1238 Tabled Paper Table 1: Number of Obstetric-Related
LA QON 1238 Tabled Paper Table 1: Number of obstetric-related separations that occurred in WA public hospitals between 1 January 2017 and 28 February 2017 (inclusive), by hospital. Number of Obstetric- Hospital related separations Albany Hospital 138 Armadale-Kelmscott Memorial Hospital 448 Bentley Hospital 161 Bridgetown Hospital < 5 Broome Hospital 100 Bunbury Hospital 286 Busselton Hospital 67 Carnarvon Hospital 14 Collie Hospital 18 Derby Hospital 33 Esperance Hospital 52 Exmouth Hospital < 5 Fiona Stanley Hospital 692 Fitzroy Crossing Hospital 7 Fremantle Hospital < 5 Geraldton Hospital 120 Graylands Hospital < 5 Halls Creek Hospital 5 Hedland Health Campus 109 Joondalup Health Campus (public patients) 634 Kalgoorlie Hospital 182 Katanning Hospital 5 Kellerberrin Hospital < 5 King Edward Memorial Hospital 1364 Kununurra Hospital 27 Margaret River Hospital 38 Meekatharra Hospital < 5 Merredin Hospital < 5 Moora Hospital < 5 Narrogin Hospital 23 Newman Hospital < 5 Next Step Drug and Alcohol Services, East Perth < 5 Nickol Bay Karratha Hospital 70 Norseman Hospital < 5 Northam Hospital < 5 Onslow Hospital < 5 Osborne Park Hospital 274 Peel Heel Campus (public patients) 258 Rockingham General Hospital 368 Royal Perth Hospital 23 Sir Charles Gairdner Hospital 26 Sir Charles Gairdner Hospital Mental Health Services < 5 St John Of God Midland (public patients) 404 Tom Price Hospital < 5 Warren Manjimup Hospital < 5 Total 5974 Page 1 of 4 LA QON 1238 Tabled Paper Table 2: Number of babies born at Western Australian public hospitals between