Ambler Road, Alaska Contents
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Intertie Options for Selected AVEC Villages
Intertie Options for Selected AVEC Villages Prepared by consultants and staff of Alaska Village Electric Cooperative August 2014 Intertie Report for Denali Commission Page | i Table of Contents Credits ..................................................................................................................................................... 1 Prologue .................................................................................................................................................. 2 Introduction ............................................................................................................................................ 3 Economies of Scale .............................................................................................................................. 5 What do Rural Alaska Interties Look Like? ............................................................................................ 6 Methods and Assumptions ...................................................................................................................... 7 Replacement ....................................................................................................................................... 7 Inflation ............................................................................................................................................... 8 N-1 Criteria .......................................................................................................................................... 9 AVEC -

Invitation to Bid Invitation Number 2519H037
INVITATION TO BID INVITATION NUMBER 2519H037 RETURN THIS BID TO THE ISSUING OFFICE AT: Department of Transportation & Public Facilities Statewide Contracting & Procurement P.O. Box 112500 (3132 Channel Drive, Suite 350) Juneau, Alaska 99811-2500 THIS IS NOT AN ORDER DATE ITB ISSUED: January 24, 2019 ITB TITLE: De-icing Chemicals SEALED BIDS MUST BE SUBMITTED TO THE STATEWIDE CONTRACTING AND PROCUREMENT OFFICE AND MUST BE TIME AND DATE STAMPED BY THE PURCHASING SECTION PRIOR TO 2:00 PM (ALASKA TIME) ON FEBRUARY 14, 2019 AT WHICH TIME THEY WILL BE PUBLICLY OPENED. DELIVERY LOCATION: See the “Bid Schedule” DELIVERY DATE: See the “Bid Schedule” F.O.B. POINT: FINAL DESTINATION IMPORTANT NOTICE: If you received this solicitation from the State’s “Online Public Notice” web site, you must register with the Procurement Officer listed on this document to receive subsequent amendments. Failure to contact the Procurement Officer may result in the rejection of your offer. BIDDER'S NOTICE: By signature on this form, the bidder certifies that: (1) the bidder has a valid Alaska business license, or will obtain one prior to award of any contract resulting from this ITB. If the bidder possesses a valid Alaska business license, the license number must be written below or one of the following forms of evidence must be submitted with the bid: • a canceled check for the business license fee; • a copy of the business license application with a receipt date stamp from the State's business license office; • a receipt from the State’s business license office for -

List of Airports by IATA Code: a Wikipedia, the Free Encyclopedia List of Airports by IATA Code: a from Wikipedia, the Free Encyclopedia
9/8/2015 List of airports by IATA code: A Wikipedia, the free encyclopedia List of airports by IATA code: A From Wikipedia, the free encyclopedia List of airports by IATA code: A B C D E F G H I J K L M N O P Q R S T U V W X Y Z See also: List of airports by ICAO code A The DST column shows the months in which Daylight Saving Time, a.k.a. Summer Time, begins and ends. A blank DST box usually indicates that the location stays on Standard Time all year, although in some cases the location stays on Summer Time all year. If a location is currently on DST, add one hour to the time in the Time column. To determine how much and in which direction you will need to adjust your watch, first adjust the time offsets of your source and destination for DST if applicable, then subtract the offset of your departure city from the offset of your destination. For example, if you were flying from Houston (UTC−6) to South Africa (UTC+2) in June, first you would add an hour to the Houston time for DST, making it UTC−5, then you would subtract 5 from +2. +2 (5) = +2 + (+5) = +7, so you would need to advance your watch by seven hours. If you were going in the opposite direction, you would subtract 2 from 5, giving you 7, indicating that you would need to turn your watch back seven hours. Contents AA AB AC AD AE AF AG AH AI AJ AK AL AM AN AO AP AQ AR AS AT AU AV AW AX AY AZ https://en.wikipedia.org/wiki/List_of_airports_by_IATA_code:_A 1/24 9/8/2015 List of airports by IATA code: A Wikipedia, the free -

7–28–03 Vol. 68 No. 144 Monday July 28, 2003 Pages 44191–44450
7–28–03 Monday Vol. 68 No. 144 July 28, 2003 Pages 44191–44450 VerDate Jan 31 2003 21:05 Jul 25, 2003 Jkt 200001 PO 00000 Frm 00001 Fmt 4710 Sfmt 4710 E:\FR\FM\28JYWS.LOC 28JYWS 1 II Federal Register / Vol. 68, No. 144 / Monday, July 28, 2003 The FEDERAL REGISTER (ISSN 0097–6326) is published daily, SUBSCRIPTIONS AND COPIES Monday through Friday, except official holidays, by the Office of the Federal Register, National Archives and Records PUBLIC Administration, Washington, DC 20408, under the Federal Register Subscriptions: Act (44 U.S.C. Ch. 15) and the regulations of the Administrative Paper or fiche 202–512–1800 Committee of the Federal Register (1 CFR Ch. I). The Assistance with public subscriptions 202–512–1806 Superintendent of Documents, U.S. Government Printing Office, Washington, DC 20402 is the exclusive distributor of the official General online information 202–512–1530; 1–888–293–6498 edition. Periodicals postage is paid at Washington, DC. Single copies/back copies: The FEDERAL REGISTER provides a uniform system for making Paper or fiche 202–512–1800 available to the public regulations and legal notices issued by Assistance with public single copies 1–866–512–1800 Federal agencies. These include Presidential proclamations and (Toll-Free) Executive Orders, Federal agency documents having general FEDERAL AGENCIES applicability and legal effect, documents required to be published by act of Congress, and other Federal agency documents of public Subscriptions: interest. Paper or fiche 202–741–6005 Documents are on file for public inspection in the Office of the Assistance with Federal agency subscriptions 202–741–6005 Federal Register the day before they are published, unless the issuing agency requests earlier filing. -
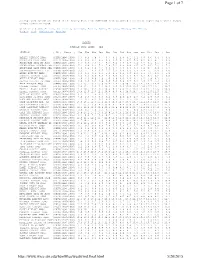
Page 1 of 7 5/20/2015
Page 1 of 7 Average wind speeds are based on the hourly data from 1996-2006 from automated stations at reporting airports (ASOS) unless otherwise noted. Click on a State: Arizona , California , Colorado , Hawaii , Idaho , Montana , Nevada , New Mexico , Oregon , Utah , Washington , Wyoming ALASKA AVERAGE WIND SPEED - MPH STATION | ID | Years | Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec | Ann AMBLER AIRPORT AWOS |PAFM|1996-2006| 6.7 8.5 7.9 7.7 6.7 5.3 4.8 5.1 6.1 6.8 6.6 6.4 | 6.5 ANAKTUVUK PASS AWOS |PAKP|1996-2006| 8.9 9.0 9.1 8.6 8.6 8.5 8.1 8.5 7.6 8.2 9.3 9.1 | 8.6 ANCHORAGE INTL AP ASOS |PANC|1996-2006| 6.7 6.0 7.5 7.7 8.7 8.2 7.8 6.8 7.1 6.6 6.1 6.1 | 7.1 ANCHORAGE-ELMENDORF AFB |PAED|1996-2006| 7.3 6.9 8.1 7.6 7.8 7.2 6.8 6.4 6.5 6.7 6.5 7.2 | 7.1 ANCHORAGE-LAKE HOOD SEA |PALH|1996-2006| 4.9 4.2 5.8 5.7 6.6 6.3 5.8 4.8 5.3 5.2 4.7 4.4 | 5.3 ANCHORAGE-MERRILL FLD |PAMR|1996-2006| 3.2 3.1 4.4 4.7 5.5 5.2 4.8 4.0 3.9 3.8 3.1 2.9 | 4.0 ANIAK AIRPORT AWOS |PANI|1996-2006| 4.9 6.6 6.5 6.4 5.6 4.5 4.2 4.0 4.6 5.5 5.5 4.1 | 5.1 ANNETTE AIRPORT ASOS |PANT|1996-2006| 9.2 8.2 8.9 7.8 7.4 7.0 6.2 6.4 7.2 8.3 8.6 9.8 | 8.0 ANVIK AIRPORT AWOS |PANV|1996-2006| 7.6 7.3 6.9 5.9 5.0 3.9 4.0 4.4 4.7 5.2 5.9 6.3 | 5.5 ARCTIC VILLAGE AP AWOS |PARC|1996-2006| 2.8 2.8 4.2 4.9 5.8 7.0 6.9 6.7 5.2 4.0 2.7 3.3 | 4.6 ATKA AIRPORT AWOS |PAAK|2000-2006| 15.1 15.1 13.1 15.0 13.4 12.4 11.9 10.7 13.5 14.5 14.7 14.4 | 13.7 BARROW AIRPORT ASOS |PABR|1996-2006| 12.2 13.1 12.4 12.1 12.4 11.5 12.6 12.5 12.6 14.0 13.7 13.1 | 12.7 BARTER ISLAND AIRPORT |PABA|1996-2006| -
State of Alaska Itb Number 2518H036 Amendment Number Three (3)
STATE OF ALASKA ITB NUMBER 2518H036 AMENDMENT NUMBER THREE (3) Department of Transportation & Public Facilities Statewide Contracting and Procurement 3132 Channel Drive, Suite 350 Juneau, Alaska 99811-2500 THIS IS NOT AN ORDER DATE AMENDMENT ISSUED: January 24, 2018 ITB TITLE: De-icing Chemicals ITB BID OPENING DATE AND TIME: February 6, 2018 @ 2:00 PM Alaska Time The following change is required: 1. ITB Bid Schedule, page 23, Lot 4, Prilled Urea is amended. The 60 tons for McGrath must be delivered to F.O.B. Point Aniak Dock. The Bid Schedule and Attachment A are amended and attached. Bidders must submit their bid on this Bid Schedule per Amendment 3 or their bid may be considered non-responsive and rejected. ________________________________________________________________________________________ This is a mandatory return Amendment. Your bid may be considered non-responsive if this signed amendment is not received [in addition to your bid] by the date and time bids are due. Becky Gattung Procurement Officer PHONE: (907) 465-8949 FAX: (907) 465-3124 EMAIL: [email protected] Complete the following and return with your bid: NAME OF COMPANY DATE PRINTED NAME SIGNATURE ITB 2518H036 - De-icing Chemicals BID SCHEDULE Per Amendment 3 CENTRAL REGION Lot No. 1(A & B): Sodium Chloride, Type 1, Grade 1 per Specification No. 1 (Delivered in bladders and bags) LOT 1(A) - Delivered in bladders- size selected by Bidder Bidder Selected Quantity Total Extended Deliver Not Deliver No F.O.B. Point Bladder Size in lbs. Mark For (Tons) Price/Tn Price Before Later Than Dillingham Dock Dillingham 60 $__________ $__________________ May 1, 2018 August 15, 2018 Lot 1(A) Totals: Total Tonnage: 60 Total Extended Price Lot 1(A): $__________________ LOT 1(B) - Delivered in 50 - 60# bags ONLY Identify Bag Quantity Total Extended Deliver Not Deliver No F.O.B. -

State of Alaska
INVITATION TO BID MAINTENANCE & OPERATIONS SPECIFICATIONS & BID DOCUMENTS PROJECT: Rural Airport Maintenance Contract – Ambler Airport, Alaska PROJECT NO. 2521N005 STATE OF ALASKA Department of Transportation And Public Facilities Northern Region DATE: August 7, 2020 INVITATION FOR BIDS Reference Project No: 2521N005 Date: August 7, 2020 Name and Location of Project: Department or Agency: Rural Airport Maintenance State of Alaska Ambler Airport Department of Transportation and Public Facilities Ambler, Alaska 99786 Supplies and Services Procurement Officer: Eric Johnson, Northern Region Issuing Office: Supplies & Services, 2301 Peger Road, Fairbanks Alaska 99709 Description of Work: The work shall consist of routine summer and winter maintenance of all runways, taxi-ways, aprons. State-owned equipment and State-owned buildings located on the airport facility, in accordance with the contract specifications. Contract Period: From date of award through June 30, 2021, with the option to renew for five (5) additional (1) one- year periods, at the sole discretion of the State. Sealed bids, in single copy for performing all work required for the above project are hereby invited. Bids will be opened publicly at 10:00 AM local time, at 2301 Peger Road, Fairbanks, Alaska, on Tuesday, August 27, 2020. SUBMISSION OF BIDS ALL BIDS INCLUDING ANY AMENDMENTS OR WITHDRAWALS MUST BE RECEIVED PRIOR TO BID OPENING. BIDS SHALL BE SUBMITTED ON THE FORMS FURNISHED AND MUST BE IN A SEALED ENVELOPE MARKED AS FOLLOWS: YOUR ADDRESS & PHONE NUMBER State of Alaska Project Name & Number: Department of Transportation Rural Airport Maintenance Services & Public Facilities Ambler, Alaska 2301 Peger Road ITB Number: 2521N005 Fairbanks, Alaska 99709-5399 Bids, amendments or withdrawals may be submitted by fax, hand delivered, or mailed in a sealed envelope. -

Ambler Airport Final EA 8-1-2013.Docx
Final Environmental Assessment Ambler Airport Improvements 67º06'04.41" North Latitude and 157º51'33.60" West Longitude Township 20 North, Range 5 East, Sections 19, 20, 21, 29, 30, and 31, Kateel River Meridian August 2013 State Project Number 61303 This page intentionally left blank. This page intentionally left blank. This page intentionally left blank. Ambler Airport Environmental Assessment August 2013 Contents 1 Introduction ............................................................................................................................... 1 1.1 Project Background ................................................................................................................... 1 1.2 Airport Description .................................................................................................................... 1 2 Purpose and Need for Proposed Action ..................................................................................... 3 2.1 Deficient Main Runway and Runway Safety Area Lengths ...................................................... 3 2.2 Reduce Terrain Obstructions ..................................................................................................... 4 2.3 Reduce Drainage issues ............................................................................................................. 4 2.4 Failing Lighting System and Navigational Aids ....................................................................... 4 3 Proposed Action ....................................................................................................................... -

101 Airport Way, Adak, AK. 99546 Innocen
ATTACHMENT A DOT/PF Maintenance Stations SOUTHCOAST REGION F.O.B. POINT Contact Name: Contact Phone: Cell: *Adak: #101 Airport Way, Adak, AK. 99546 Innocent Dushkin 592-8026 572-9960 Atka: Atka, AK 99547 Dale Ruckman 581-1786 359-1786 Chenega Bay: Chenega Bay, AK 99574 John Lunetta 441-5589 n/a Chignik Bay: #101 Airport Way, Chignik, AK. 99565 Kyler Hylton 246-3325 439-1129 Cold Bay: 97 St Louis Ave., Cold Bay, AK 99571 Hap Kremer 532-5000 854-3583 Gustavus: Gustavus Airport, Gustavus, AK 99826 Jeff Jarvis 697-2251 723-8954 Haines: 720 Main St., Haines, AK 99827 Matt Boron 766-2340 314-0334 Hoonah: 700 Airport Way, Hoonah, AK 99829 Ken Meserve 945-3426 723-2375 *Iliamna: #1 Airport Road, Iliamna, AK 99606 Clint Anelon 571-1261 571-7171 Juneau: 6860 Glacier Hwy., Juneau, AK 99801 Casey Walker 465-1787 723-7028 Kalsin Bay: 1500 Anton Larson RD Kodiak, AK 99615 Bruce McNeil 487-4952 539-7072 Ketchikan: 5148 N. Tongass Hwy. Ketchikan, AK 99901 Loren Starr 225-2513 617-7400 King River: MP 66, King River, AK 99645 Andy Weiland 745-2159 355-5116 King Salmon: 123 Main St., King Salmon, AK 99613 Kyler Hylton 246-3325 439-1129 Klawock: 1/4 Mile Airport Rd., Klawock, AK 99921 Tim Lacour 755-2229 401-0240 Kodiak: 1500 Anton Larson Rd., Kodiak, AK 99615 Bruce McNeil 487-4952 539-7072 Levelock: #101 Airport Way, Levelock, AK 99625 Kyler Hylton 246-3325 439-1129 Petersburg: 288 Mitkof Hwy., Petersburg, AK 99833 Mike Etcher 772-4624 518-9012 Port Heiden: #101 Airport Way, Port Heiden, AK 99549 Derek Schraffenberger 837-2410 444-9260 Sitka: 605 Airport -
ITB No. 2519H039 Grader, Wing & Plow Blades.Pdf
INVITATION TO BID ITB No.: 2519H039 RETURN THIS BID TO THE ISSUING OFFICE AT: Department of Transportation & Public Facilities Statewide Contracting & Procurement P.O. Box 112500 (3132 Channel Drive, Suite 350) Juneau, Alaska 99811-2500 THIS IS NOT AN ORDER DATE ITB ISSUED: March 1, 2019 ITB TITLE: Grader, Wing, and Plow Blades SEALED BIDS MUST BE SUBMITTED TO THE STATEWIDE CONTRACTING AND PROCUREMENT SECTION. BIDS MUST BE TIME AND DATE STAMPED BY THE PURCHASING SECTION PRIOR TO 2:00 PM ON MARCH 27, 2019, AT WHICH TIME THEY WILL BE PUBLICLY OPENED. DELIVERY LOCATION: See the “Bid Schedule” and “Attachment A”. DELIVERY DATE: Not before July 1, 2019 and no later than September 30, 2019, unless otherwise noted on the Bid Schedule. *See Northern Region lots for asterisk. F.O.B. POINT: FINAL DESTINATION IMPORTANT NOTICE: If you received this solicitation from the State’s “Online Public Notice” web site, you must register with the Procurement Officer listed on this document to receive notification of subsequent amendments. Failure to contact the Procurement Officer may result in the rejection of your offer. BIDDER'S NOTICE: By signature on this form, the Bidder certifies that: (1) the Bidder has a valid Alaska business license, or will obtain one prior to award of any contract resulting from this ITB. If the Bidder possesses a valid Alaska business license, the license number must be written below or one of the following forms of evidence must be submitted with the bid: • a canceled check for the business license fee; • a copy of the business -

Airport Diagram Airport Diagram
18200 KING SALMON (AKN)(PAKN) AIRPORT DIAGRAM AL-1237 (FAA) KING SALMON, ALASKA ATIS 128.8 KING SALMON TOWER 118.3 279.5 GND CON 121.9 E 3 D . 14 R VA USAF AREA BASE OPS JANUARY 2015 ANNUAL RATE OF CHANGE 0.3° W L N MILITARY M RAMP K 12 ELEV 60 18 58°41'N A 117 ° . 0 5 . ° ELEV B CIVIL 66 RAMP 182 AK, 19 JUL 2018 to 13 SEP 100 X 165 4017 TWR 125 8901 X 150 D C ° 0 . ELEV AK, 19 JUL 2018 to 13 SEP 60 36 002 E G 297 .6 ° EAST RAMP P FIELD ELEV 73 30 58°40'N RWY 12-30 PCN 67 F/B/X/T S-67, D-90, 2D-175, 2D/2D2-335 RWY 18-36 PCN 66 F/B/X/T S-30, D-50 CAUTION: BE ALERT TO RUNWAY CROSSING CLEARANCES. READBACK OF ALL RUNWAY HOLDING INSTRUCTIONS IS REQUIRED. 156°40'W 156°39'W 156°38'W KING SALMON, ALASKA AIRPORT DIAGRAM KING SALMON (AKN)(PAKN) 18200 AK, 19 JUL 2018 to 13 SEP 2018 SEP 13 to 2018 JUL 19 AK, AK, 19 JUL 2018 to 13 SEP 2018 KING SALMON, ALASKA AL-1237 (FAA) 18200 WAAS APP CRS Rwy Idg 8501 CH77908 TDZE 73 RNAV (GPS) RWY 30 296° W30A Apt Elev 73 KING SALMON (AKN)(PAKN) T For uncompensated Baro-VNAV systems, LNAV/VNAV MISSED APPROACH: Climb to 3000 direct A NA below -25°C (-13°F) or above 49°C (120°F). DME/DME HEXES and via 250° track to EXIPE and via -31°C RNP-0.3 NA. -

Planning Commission Meeting Minutes
Northwest Arctic Borough Planning Commission Regular Quarterly Meeting Minutes June 27, 2014 - 9:00 A.M. Northwest Arctic Borough Assembly Chambers, Kotzebue, AK CALL TO ORDER Madam Chair Barbara MacManus called the meeting to order at 9:07 A.M. INVOCATION/MOMENT OF SILENCE Millie Hawley gave invocation. ROLL CALL Commissioners Present During Roll Call: Barbara MacManus Calvin Moto Sr Ernie Norton Dale Stotts Carol Wesley Millie Hawley Absent Janet Mills Daniel Foster Sr. A quorum has been established to conduct business. INTRODUCTION OF STAFF AND GUESTS Noah Naylor Charlie Gregg Zach Stevenson Al Beck John Chase Damian Phillips Robert Gransberry Jennifer Smith Paul Karczmarczyk Phi Barnes Calvin Moto II Elia Gomez Vern Cleveland Sr. Natalia Ruppert (Telephonic) AGENDA APPROVAL The agenda of June 27, 2014 was presented for approval. Noah mentioned that National Park Service won’t be able to attend today; remove from communications and appearances on the agenda. Noah also requested to switch communications and appearances and conditional use permits on the agenda. 1 Planning Commission – June 27, 2014 Commissioner Dale Stotts moved, seconded by Commissioner Millie Hawley to approve the agenda as amended. The motion passed unanimously. MINUTES APPROVAL Minutes of previous meeting dated February 19, 2014 were presented for approval. Member Stotts requested information regarding the Shell presentation that Mayor Joule has given on purpose of the Science Department. Commissioner Ernie Norton moved, seconded by Commissioner Millie Hawley to approve the minutes. The motion passed unanimously. PUBLIC HEARING/COMMENTS FOR APPROVAL OF CONDITIONAL USE PERMITS a) Permit No. 113-03-14 Shungnak Trial Council submitted a title 9 permit to construct a 2.6 mile gravel road that will provide access to a new landfill site for the community.