Evaluation of Kangaroo Mother Care Services in Uganda
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Nakaseke Constituency: 109 Nakaseke South County
Printed on: Monday, January 18, 2021 16:36:23 PM PRESIDENTIAL ELECTIONS, (Presidential Elections Act, 2005, Section 48) RESULTS TALLY SHEET DISTRICT: 069 NAKASEKE CONSTITUENCY: 109 NAKASEKE SOUTH COUNTY Parish Station Reg. AMURIAT KABULETA KALEMBE KATUMBA KYAGULA MAO MAYAMBA MUGISHA MWESIGYE TUMUKUN YOWERI Valid Invalid Total Voters OBOI KIIZA NANCY JOHN NYI NORBERT LA WILLY MUNTU FRED DE HENRY MUSEVENI Votes Votes Votes PATRICK JOSEPH LINDA SSENTAMU GREGG KAKURUG TIBUHABU ROBERT U RWA KAGUTA Sub-county: 001 KAASANGOMBE 014 BUKUUKU 01 TIMUNA/KAFENE 716 1 0 1 0 278 2 0 1 0 1 140 424 43 467 0.24% 0.00% 0.24% 0.00% 65.57% 0.47% 0.00% 0.24% 0.00% 0.24% 33.02% 9.21% 65.22% 02 LUKYAMU PR. SCHOOL 778 2 2 0 1 348 2 2 0 1 0 110 468 24 492 0.43% 0.43% 0.00% 0.21% 74.36% 0.43% 0.43% 0.00% 0.21% 0.00% 23.50% 4.88% 63.24% 03 BUKUUKU PRI. SCHOOL 529 0 0 1 1 188 0 1 0 0 0 74 265 3 268 0.00% 0.00% 0.38% 0.38% 70.94% 0.00% 0.38% 0.00% 0.00% 0.00% 27.92% 1.12% 50.66% Parish Total 2023 3 2 2 2 814 4 3 1 1 1 324 1157 70 1227 0.26% 0.17% 0.17% 0.17% 70.35% 0.35% 0.26% 0.09% 0.09% 0.09% 28.00% 5.70% 60.65% 015 BULYAKE 01 NJAGALABWAMI COMM. -

Nakaseke Makes Model Town Plan
40 The New Vision, FrIday, June 4, 2010 NAKASEKE DISTRICT REVIEW SUPPLEMENT Farmers benefit from Caritas support JOHN KASOZI By John Kasozi education, in August 1993 increased, I got married truck. Next year, he plans he moved to Kampala to the following year.” to buy a plot in Kampala ILSON Nsobya find employment. He initial- Nsobya now has 15 and build a commercial could not ly wanted to work as a acres of land under structure in future. believe, when vehicle mechanic, but he pineapples. He pays school fees Wa lady she met ended up as a cleaner. He notes that on for his four children and six in the bank paid sh24,000 “I decided to go back average an acre of others. as school fees for her home after working for one pineapple brings in about Joyce Kizito, the kindergarten child. That and half years,” says sh5m per year. But with Kamukamu community was in 1993 when his Nsobya. intensive farming, a farmer resource person from monthly pay was One morning in 1994, can garner about sh10m, Kawula, Luweero who sh20,000. Nsobya decided to pack his he says. is also a CARITAS “From that day, I became four-inch mattress, The cost of one pineapple beneficiary says before restless. I wondered how Panasonic radio, a basin ranges between sh600 to they started getting I would pay fees for my and utensils. He used his sh1, 000, Nsobya says support from from the children, rent, feed the savings of sh3,000 for adding that his clientele is organisation in 2002, their family, settle medical transport. -

Typhoid Over Diagnosis in Nakaseke District, June 2016
Public Health Fellowship Program – Field Epidemiology Track Typhoid Over diagnosis in Nakaseke District, June 2016 Dr. Kusiima Joy, MBChB-MHSR Fellow,2016 Typhoid Alert May June 2016 2016 1 2 3 4 5 6 7 8 9 10 11 12 13 14 Notification Data Audit ,12 health Reviewed HMIS data facilities Nakaseke 84 cases/ 50,000 by FFETP(wk 15-21) Typhoid Outbreak verification exercise 323 Typhoid cases reported 2 Typhoid verification in Nakaseke District Objectives . Verify the existence of an outbreak . Verify reported diagnosis using standard case definition . Recommend public health action 3 Typhoid verification in Nakaseke District District location 4 Typhoid verification in Nakaseke District Facilities selected . Private hospital - Kiwoko . Government hospital - Nakaseke . Health center IV - Semuto . Health center III - Kapeeka 5 Typhoid verification in Nakaseke District Data collection . Extracted records from registers (1st/12/ 2015 to 14th/06/2016) . Discussed with clinicians & lab personnel . Took clinical history &examined typhoid suspects 6 Typhoid verification in Nakaseke District Standard case definition . Suspected case: Onset of fever ≥3days,negative malaria test, resident of Nakaseke district Plus any of following: chills, malaise, headache, sore throat, cough, abdominal pain, constipation, diarrhea . Probable case: Suspected case plus positive antigen test (Widal) . Confirmed case: Suspected case plus salmonella typhi (+) blood or stool by culture 7 Typhoid verification in Nakaseke District Data quality assessment . Reviewed laboratory -
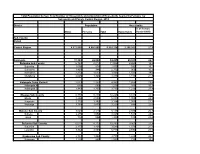
Population by Parish
Total Population by Sex, Total Number of Households and proportion of Households headed by Females by Subcounty and Parish, Central Region, 2014 District Population Households % of Female Males Females Total Households Headed HHS Sub-County Parish Central Region 4,672,658 4,856,580 9,529,238 2,298,942 27.5 Kalangala 31,349 22,944 54,293 20,041 22.7 Bujumba Sub County 6,743 4,813 11,556 4,453 19.3 Bujumba 1,096 874 1,970 592 19.1 Bunyama 1,428 944 2,372 962 16.2 Bwendero 2,214 1,627 3,841 1,586 19.0 Mulabana 2,005 1,368 3,373 1,313 21.9 Kalangala Town Council 2,623 2,357 4,980 1,604 29.4 Kalangala A 680 590 1,270 385 35.8 Kalangala B 1,943 1,767 3,710 1,219 27.4 Mugoye Sub County 6,777 5,447 12,224 3,811 23.9 Bbeta 3,246 2,585 5,831 1,909 24.9 Kagulube 1,772 1,392 3,164 1,003 23.3 Kayunga 1,759 1,470 3,229 899 22.6 Bubeke Sub County 3,023 2,110 5,133 2,036 26.7 Bubeke 2,275 1,554 3,829 1,518 28.0 Jaana 748 556 1,304 518 23.0 Bufumira Sub County 6,019 4,273 10,292 3,967 22.8 Bufumira 2,177 1,404 3,581 1,373 21.4 Lulamba 3,842 2,869 6,711 2,594 23.5 Kyamuswa Sub County 2,733 1,998 4,731 1,820 20.3 Buwanga 1,226 865 2,091 770 19.5 Buzingo 1,507 1,133 2,640 1,050 20.9 Maziga Sub County 3,431 1,946 5,377 2,350 20.8 Buggala 2,190 1,228 3,418 1,484 21.4 Butulume 1,241 718 1,959 866 19.9 Kampala District 712,762 794,318 1,507,080 414,406 30.3 Central Division 37,435 37,733 75,168 23,142 32.7 Bukesa 4,326 4,711 9,037 2,809 37.0 Civic Centre 224 151 375 161 14.9 Industrial Area 383 262 645 259 13.9 Kagugube 2,983 3,246 6,229 2,608 42.7 Kamwokya -
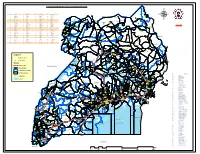
Legend " Wanseko " 159 !
CONSTITUENT MAP FOR UGANDA_ELECTORAL AREAS 2016 CONSTITUENT MAP FOR UGANDA GAZETTED ELECTORAL AREAS FOR 2016 GENERAL ELECTIONS CODE CONSTITUENCY CODE CONSTITUENCY CODE CONSTITUENCY CODE CONSTITUENCY 266 LAMWO CTY 51 TOROMA CTY 101 BULAMOGI CTY 154 ERUTR CTY NORTH 165 KOBOKO MC 52 KABERAMAIDO CTY 102 KIGULU CTY SOUTH 155 DOKOLO SOUTH CTY Pirre 1 BUSIRO CTY EST 53 SERERE CTY 103 KIGULU CTY NORTH 156 DOKOLO NORTH CTY !. Agoro 2 BUSIRO CTY NORTH 54 KASILO CTY 104 IGANGA MC 157 MOROTO CTY !. 58 3 BUSIRO CTY SOUTH 55 KACHUMBALU CTY 105 BUGWERI CTY 158 AJURI CTY SOUTH SUDAN Morungole 4 KYADDONDO CTY EST 56 BUKEDEA CTY 106 BUNYA CTY EST 159 KOLE SOUTH CTY Metuli Lotuturu !. !. Kimion 5 KYADDONDO CTY NORTH 57 DODOTH WEST CTY 107 BUNYA CTY SOUTH 160 KOLE NORTH CTY !. "57 !. 6 KIIRA MC 58 DODOTH EST CTY 108 BUNYA CTY WEST 161 OYAM CTY SOUTH Apok !. 7 EBB MC 59 TEPETH CTY 109 BUNGOKHO CTY SOUTH 162 OYAM CTY NORTH 8 MUKONO CTY SOUTH 60 MOROTO MC 110 BUNGOKHO CTY NORTH 163 KOBOKO MC 173 " 9 MUKONO CTY NORTH 61 MATHENUKO CTY 111 MBALE MC 164 VURA CTY 180 Madi Opei Loitanit Midigo Kaabong 10 NAKIFUMA CTY 62 PIAN CTY 112 KABALE MC 165 UPPER MADI CTY NIMULE Lokung Paloga !. !. µ !. "!. 11 BUIKWE CTY WEST 63 CHEKWIL CTY 113 MITYANA CTY SOUTH 166 TEREGO EST CTY Dufile "!. !. LAMWO !. KAABONG 177 YUMBE Nimule " Akilok 12 BUIKWE CTY SOUTH 64 BAMBA CTY 114 MITYANA CTY NORTH 168 ARUA MC Rumogi MOYO !. !. Oraba Ludara !. " Karenga 13 BUIKWE CTY NORTH 65 BUGHENDERA CTY 115 BUSUJJU 169 LOWER MADI CTY !. -

Client Satisfaction with Health Insurance in Uganda
Client Satisfaction with Health Insurance - Uganda CLIENT SATISFACTION WITH HEALTH INSURANCE IN UGANDA 1 Client Satisfaction with Health Insurance - Uganda TABLE OF CONTENTS I INTRODUCTION ..................................................................................................................................................... 6 II RESEARCH OVERVIEW ..................................................................................................................................... 6 RESEARCH OBJECTIVE ............................................................................................................................................... 6 RESEARCH METHODS ................................................................................................................................................ 6 RESEARCH SAMPLE ................................................................................................................................................... 7 REPORT OUTLINE ...................................................................................................................................................... 7 III SAVE FOR HEALTH UGANDA (SHU) ............................................................................................................. 8 BACKGROUND ON SAVE FOR HEALTH UGANDA (SHU) ............................................................................................. 8 THE KAMULI MUGANZI AWONGERWA ASSOCIATION – INSURANCE/CREDIT SCHEME .............................................. 8 -

NAKASEKE DLG Q4 REPORT.Pdf
Local Government Quarterly Performance Report Vote: 569 Nakaseke District 2016/17 Quarter 4 Structure of Quarterly Performance Report Summary Quarterly Department Workplan Performance Cumulative Department Workplan Performance Location of Transfers to Lower Local Services and Capital Investments Submission checklist I hereby submit _________________________________________________________________________. This is in accordance with Paragraph 8 of the letter appointing me as an Accounting Officer for Vote:569 Nakaseke District for FY 2016/17. I confirm that the information provided in this report represents the actual performance achieved by the Local Government for the period under review. Name and Signature: Chief Administrative Officer, Nakaseke District Date: 8/23/2017 cc. The LCV Chairperson (District)/ The Mayor (Municipality) Page 1 Local Government Quarterly Performance Report Vote: 569 Nakaseke District 2016/17 Quarter 4 Summary: Overview of Revenues and Expenditures Overall Revenue Performance Cumulative Receipts Performance Approved Budget Cumulative % UShs 000's Receipts Budget Received 1. Locally Raised Revenues 1,338,786 1,704,820 127% 2a. Discretionary Government Transfers 3,314,474 3,260,284 98% 2b. Conditional Government Transfers 16,270,489 15,459,486 95% 2c. Other Government Transfers 948,643 966,847 102% 4. Donor Funding 22,900 Total Revenues 21,872,393 21,414,338 98% Overall Expenditure Performance Cumulative Releases and Expenditure Perfromance Approved Budget Cumulative Cumulative % % % UShs 000's Releases Expenditure -

Emergency Health Fiscal and Growth Stabilization and Development
LIST OF COVID-19 QUARANTINE CENTRES IN WATER AND POWER UTILITIES OPERATION AREAS WATER S/N QUARANTINE CENTRE LOCATION POWER UTILITY UTILITY 1 MASAFU GENERAL HOSPITAL BUSIA UWS-E UMEME LTD 2 BUSWALE SECONDARY SCHOOL NAMAYINGO UWS-E UMEME LTD 3 KATAKWI ISOLATION CENTRE KATAKWI UWS-E UMEME LTD 4 BUKWO HC IV BUKWO UWS-E UMEME LTD 5 AMANANG SECONDARY SCHOOL BUKWO UWS-E UMEME LTD 6 BUKIGAI HC III BUDUDA UWS-E UMEME LTD 7 BULUCHEKE SECONDARY SCHOOL BUDUDA UWS-E UMEME LTD 8 KATIKIT P/S-AMUDAT DISTRICT KATIKIT UWS-K UEDCL 9 NAMALU P/S- NAKAPIRIPIRIT DISTRICT NAMALU UWS-K UEDCL 10 ARENGESIEP S.S-NABILATUK DISTRICT ARENGESIEP UWS-K UEDCL 11 ABIM S.S- ABIM DISTRICT ABIM UWS-K UEDCL 12 KARENGA GIRLS P/S-KARENGA DISTRICT KARENGA UWS-K UMEME LTD 13 NAKAPELIMORU P/S- KOTIDO DISTRICT NAKAPELIMORU UWS-K UEDCL KOBULIN VOCATIONAL TRAINING CENTER- 14 NAPAK UWS-K UEDCL NAPAK DISTRICT 15 NADUNGET HCIII -MOROTO DISTRICT NADUNGET UWS-K UEDCL 16 AMOLATAR SS AMOLATAR UWS-N UEDCL 17 OYAM OYAM UWS-N UMEME LTD 18 PADIBE IN LAMWO DISTRICT LAMWO UWS-N UMEME LTD 19 OPIT IN OMORO OMORO UWS-N UMEME LTD 20 PABBO SS IN AMURU AMURU UWS-N UEDCL 21 DOUGLAS VILLA HOSTELS MAKERERE NWSC UMEME LTD 22 OLIMPIA HOSTEL KIKONI NWSC UMEME LTD 23 LUTAYA GEOFREY NAJJANANKUMBI NWSC UMEME LTD 24 SEKYETE SHEM KIKONI NWSC UMEME LTD PLOT 27 BLKS A-F AKII 25 THE EMIN PASHA HOTEL NWSC UMEME LTD BUA RD 26 ARCH APARTMENTS LTD KIWATULE NWSC UMEME LTD 27 ARCH APARTMENTS LTD KIGOWA NTINDA NWSC UMEME LTD 28 MARIUM S SANTA KYEYUNE KIWATULE NWSC UMEME LTD JINJA SCHOOL OF NURSING AND CLIVE ROAD JINJA 29 MIDWIFERY A/C UNDER MIN.OF P.O.BOX 43, JINJA, NWSC UMEME LTD EDUCATION& SPORTS UGANDA BUGONGA ROAD FTI 30 MAAIF(FISHERIES TRAINING INSTITUTE) NWSC UMEME LTD SCHOOL PLOT 4 GOWERS 31 CENTRAL INN LIMITED NWSC UMEME LTD ROAD PLOT 2 GOWERS 32 CENTRAL INN LIMITED NWSC UMEME LTD ROAD PLOT 45/47 CHURCH 33 CENTRAL INN LIMITED NWSC UMEME LTD RD CENTRAL I INSTITUTE OF SURVEY & LAND PLOT B 2-5 STEVEN 34 NWSC 0 MANAGEMENT KABUYE CLOSE 35 SURVEY TRAINING SCHOOL GOWERS PARK NWSC 0 DIVISION B - 36 DR. -
![Uganda Health Facilities Survey 2002 [FR140]](https://docslib.b-cdn.net/cover/8904/uganda-health-facilities-survey-2002-fr140-1738904.webp)
Uganda Health Facilities Survey 2002 [FR140]
Uganda Health Facilities Survey 2002 Ministry of Health Kampala, Uganda ORC Macro MEASURE DHS+ Calverton, Maryland, USA John Snow, Inc./DELIVER Arlington, Virginia, USA JSI Research & Training Institute, Inc./ Uganda AIDS/HIV Integrated Model District Programme (AIM) Kampala, Uganda June 2003 Contributors: John Snow, Inc./DELIVER JSI Research and Training Institute, Inc./AIM Dana Aronovich Evas Kansiime Allison Farnum Cochran Maurice Adams Erika Ronnow Ministry of Health ORC Macro F. G. Omaswa Gregory Pappas H. Kyabaggu Eddie Mukooyo Martin O. Oteba This report presents findings from the 2002 Uganda Health Facilities Survey (UHFS 2002) carried out by the Uganda Ministry of Health. ORC Macro (MEASURE DHS+) and John Snow, Inc. (DELIVER) provided technical assistance. Other organizations contributing to the project were the U.S. Centers for Disease Control and Prevention (CDC/Uganda), the U.S. Agency for International Development (USAID/Uganda), and the JSI Research and Training Institute, Inc., AIDS/HIV Integrated Model District Programme (AIM). MEASURE DHS+, a USAID-funded project, assists countries worldwide in the collection and use of data to monitor and evaluate population, health, and nutrition programs. Information about the Uganda Health Facilities Survey or about the MEASURE DHS+ project can be obtained by contacting: MEASURE DHS+, ORC Macro, 11785 Beltsville Drive, Suite 300, Calverton, MD 20705 (Telephone 301-572-0200; Fax 301-572-0999; E-mail [email protected]; Internet: www.measuredhs.com). DELIVER, a worldwide technical assistance support project, is funded by the Commodities Security and Logistics Division (CSL) of the Office of Population and Reproductive Health of the Bureau for Global Health (GH) of the U.S. -
Usaid/Uganda Private Health Support Program (June 2013-June 2018)
USAID/UGANDA PRIVATE HEALTH SUPPORT PROGRAM (JUNE 2013-JUNE 2018) FINAL REPORT Contract No.: AID-617-C-13-00005 C Mothers and infants awaiting treatment at St Francis Health Care Services in Njeru (January 2018) September 2018 This report is made possible by the support of the American People through the United States Agency for International Development (USAID). The contents of this report are the sole responsibility of Cardno Emerging Markets USA, Ltd. and do not necessarily reflect the views of USAID or the United States Government. USAID/UGANDA PRIVATE HEALTH SUPPORT PROGRAM (JUNE 2013-JUNE 2018) FINAL REPORT Submitted by: Cardno Emerging Markets USA, Ltd. Submitted to: USAID/Uganda Contract No.: AID-617-C-13-00005 DISCLAIMER The author’s views expressed in this publication do not necessarily reflect the views of the United States Agency for International Development or the United States Government. USAID/Uganda Private Health Support Program Table of Contents ACRONYMS ............................................................................................................................................................. III EXECUTIVE SUMMARY ........................................................................................................................................... 1 CONTEXTUAL OVERVIEW ..................................................................................................................................... 4 PROGRAM OBJECTIVES ........................................................................................................................................... -

Comparison of Public and Pnfp Hospitals in Uganda
public administration and development Public Admin. Dev. 22, 415–428 (2002) Published online in Wiley InterScience (www.interscience.wiley.com) DOI: 10.1002/pad.244 WHAT COULD BE ACHIEVED WITH GREATER PUBLIC HOSPITAL AUTONOMY? COMPARISON OF PUBLIC AND PNFP HOSPITALS IN UGANDA FREDDIE SSENGOOBA1, LYNN ATUYAMBE1, BARBARA McPAKE2*, KARA HANSON3 AND SAM OKUONZI4 1Institute of Public Health, Makerere University, Uganda 2Health Systems Development Programme and Health Economics and Financing Programme, Health Policy Unit, London School of Hygiene and Tropical Medicine, London, UK 3Health Economics and Financing Programme, Health Policy Unit, London School of Hygiene and Tropical Medicine, London, UK 4Health Policy Unit, Ministry of Health, Uganda SUMMARY The policy of hospital autonomy has been discussed for some time in Uganda. There is little evidence from Uganda or elsewhere that increased autonomy will improve hospital performance. This article compares the performance of three private not-for- profit (PNFP) and public hospital pairs to address this question. PNFP and public hospitals have similar management structures but PNFP hospitals had better trained managers and a church affiliated chair in the hospital management committee. Both types have problems with personnel management but these appear more pronounced in public hospitals. Drug supply management appears better in PNFP hospitals. Overall, workloads are similar, but analysis of patterns of utilisation and prices across services suggest that patient choice of facilities is influenced by relative price levels, and that willingness to pay is higher for PNFP services. PNFP hospitals are more successful at generating revenue. There are no clear differences in efficiency between PNFP and public hospitals but there is some evidence of higher quality levels in PNFP hospitals. -

Prevalence of Intestinal Nematodes Among Children Below Ten Years Attending Kiwoko Hospital Pediatric Unit, Kasana, Nakaseke, District, Uganda
PrEVALENCE OF INTESTINAL Nematodes AMONG ChildrEN BELOW TEN YEARS ATTENDING KiwokO Hospital Pediatric Unit, Kasana, Nakaseke, District, Uganda. Henry Pecos NvuleA A Faculty OF Health Sciences , Uganda Martyrs University, Uganda AbstrACT Background:A INTESTINAL NEMATODES ARE AMONG THE MOST COMMON PARASITES INFECTING HUMANS IN DEVELOPING countries, PRECISE ESTIMATES OF THE POPULATIONS AT RISK OF INFECTION ARE DIffiCULT TO derive. TherEFORE TO UNDERSTAND THE DISEASE BURDEN THERE IS A NEED FOR RELIABLE DATA ON THE PREVALENCE OF INFECTION AS WELL AS INFORMATION ON THE RISK FACTORS OF infection. Methodology: 99 STOOL SAMPLES WERE COLLECTED FROM CHILDREN WHO PRESENTED WITH diarrhea, FEver, ITCHY ANUS OPENING ALL SYMPTOMS OF INTESTINAL NEMATODE infection. Stool SAMPLES WERE SCREENED USING THE DIRECT SALINE method. Samples NEGATIVE BY DIRECT SALINE WERE FURTHER EXAMINED USING THE FORMAL ETHER TECHNIQUE AND STAINED BY EOSIN FOR VISUALIZATION OF PARASITES eggs. A QUESTIONNAIRE WAS ADMINISTERED TO THEIR GUARdians/parENTS TO ASSESS THE RISK FACTORS OF infection. Results: The PREVALENCE OF INTESTINAL NEMATODE INFECTION WAS FOUND TO BE 62.6% (62/99). The INTESTINAL NEMATODE INFECTION RATE WAS FOUND TO BE HIGHER IN CHILDREN OVER fiVE YEARS AS COMPARED TO CHILDREN BELOW fiVE YEARS WITH A PREVALENCE OF 64.2% (43/67) AND 59.4% (19/32) RESPECTIVELY. The PREVALENCE OF INFECTION BY SEX WAS 66% (31/47) IN MALES AND 59.6% (31/52) IN females. Ascaris LUMBRICOIDES WERE THE MOST PREVALENT PARASITE IDENTIfiED IN 25 OF THE 62 PATIENTS INFECTED WITH INTESTINAL nematodes. This WAS FOLLOWED BY Hookworm (17/62), TRICHURIS TRICHIURA (12/62), AND StrONGYLOIDES STERCORALIS (8/62). Poor HYGIENE WAS THE MOST COMMON RISK FACTOR CITED FOLLOWED BY ILLITERACY AND POVERTY.