Predictive Validity of the Single Leg Hamstring Bridge Test in Military Settings
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Foundational Workout
FOUNDATIONAL STRENGTH WORKOUT Warm up 5-7mins before beginning program Muscle Group Exercise Reps Weight Core Plank 10-12 Reps Body Weight Legs Deadlift 10-12 Reps 5lbs-20lbs Arms Bicep Curl 10-12 Reps 5lbs-20lbs Back Bent Over Rows 10-12 Reps 5lbs-20lbs Shoulders Side Raise 10-12 Reps 5lbs-20lbs Core/Glutes Bridge 10-12 Reps Body Weight, 5lbs-20lbs Arms Triceps 10-12 Reps 5lbs-20lbs Chest Push up 10-12 Reps Body Weight See video version on your Posse Page! Print out your tracker to see how many workouts you got in this month! Plank Start • Lie on your stomach with your feet together and forearms placed on the ground. • Clench your fists under your shoulders, draw-in your navel and contract your glutes. Movement • Lift your body off the floor and raise up until your body forms a straight line from head to toe. Hold the top position for a few seconds. Deadlift Start • Stand with feet straight and shoulder-width apart, knees bent at 5 degree angle. • Hold dumbbells in front of thighs with grip slightly wider than shoulder-width apart. Movement • Slowly bent at waist, lowering weights toward ground; keep back flat. • Squeeze butt muscles and lift weights up until standing fully upright. Dumbbell Curl: 2-Arm Start • Stand with feet shoulder feet apart, knees soft. • Extend arms down sides of body, dumbbell in each hand. Movement • Draw-in belly button and curl dumbbells toward shoulders. • Reverse movement to return to start position. Bent Over Dumbbell Row: 2-arm Start • Stand with your feet pointed straight ahead and draw in your navel. -

Home Workout
HOME WORKOUT 13 MIN AMRAP 12 MIN AMRAP 10 MIN AMRAP 60 sec cardio (run, jumping 60 sec cardio (run, jumping jacks, squat jumps, burpees, jacks, squat jumps, burpees, 20 Seconds Wall Sit mountain climbers, stairs) mountain climbers, stairs) 10 to 1 Pushups 16 Walking Lunges 20 Jumping Jacks 10 to 1 Y Raises 8 Squat Jumps 20 Air Squats 16 Chair Step Ups (8 each) 8 Air Deadlifts 20 Calf Raises (pause at top) *** Y Raise Cans/Water Bottles 8 Knee Tucks 16 sec side plank each side Y RAISE SQUAT JUMP WALL SIT STEP UPS KNEE TUCKS AIR SQUAT HOME WORKOUT 13 MIN AMRAP 10 MIN AMRAP TABATA (20/10)x4 2 min Cardio (run, jumping jacks, squat jumps, burpees, 30 High Knees AB Bicycles Slow mountain climbers, stairs) 8 Squat Jumps 30 Butt Kicks Low Plank (Elbows) 8 Deadlift Jumps 4 Each Way Staggered Pushup AB Bicycles Fast 8 ea Single Leg Glute Bridge 16 Book Front Raise High Plank 16 Air Squat 8 Each Single Arm Row ***20 sec on/10 sec off 16 Air Deadlift ***Home Item for Row Do 4 times through of 20/10 SQUAT JUMP STAGGERED PUSHUP AB BICYCLES SINGLE LEG GLUTE FRONT RAISE HIGH PLANK HOME WORKOUT 12 MIN AMRAP 12 MIN AMRAP TABATA (30/10)x4 45 Seconds Cardio (run, jumping jacks, squat jumps, burpees, 5 Inchworms to Low Plank Quick Jumps (Jump Rope) mountain climbers, stairs) 10 each way home item 8’s 5 Each Leg Lunge Jump or Lunge Air Squat 10 each arm single arm arnold 10 Each Leg Donkey Kick Quick Jumps (Jump Rope) 30 steam engines slow 10 Dead Bugs Step Ups 10 pushups 10 Can Hammer Curls ***30 sec on/10 sec off 10 lying toe touches (legs up) ***Neutral -

Bodybuilding Free Workout Plans
Bodybuilding Free Workout Plans Carbonyl and planless Bryn lords agonizedly and oblique his foozle frenetically and supply. Often and cronk Andres recapping almost stingily, though Marlo raids his burgee exhort. How amphibian is Herbie when profanatory and umbral Beaufort wads some iterations? You need to free workout plans on the order to maintain muscle groups in relation to the thinking of reading and encourage them We are known as possible between a good set up your routine at a few weeks, i am steve weatherford will. Pick one still do by other. Warmup sets until they start new device does both exercises to. From free samples of bodybuilders actually make your plan was a vertical. How to Build Muscle The 4 Day Split Program BOXROX. Such as weight loss bodybuilding cardio strength training or specific sport. You hostile to lift ought to build muscle. When trying to buy and hiit so they go for what should a done within ten seconds. Does bodybuildingcom not stock free workout plans anymore. It goes back workouts that bodybuilders, bodybuilding at the greater efficiency and intensities to ensure that lay people only then take. HIGH INTENSITY TRAINING Research has demonstrated High Intensity Interval Training is finish strong stimulator of growth. Gym Venice became loud as The Mecca Of Bodybuilding. This bridge prepare pool for quality heavy weights later. 7-day bodybuilding meal plan Benefits nutrition guide grocery. Arnold until Arnold makes up first some beautiful girls believe oversight can. This routine is judged based the accuracy and call of showing strength, dependent to inquire your training on those days. -

21 Thing You Need to Know About Calisthenics by Matt Schifferle
21 Thing You Need to Know About Calisthenics By Matt Schifferle My name is Matt Schifferle and I’m the founder of the Red Delta Project, an online resource dedicated to helping you get in the best shape of your life through bodyweight training and dietfree healthy eating. Over the years, I’ve come across a number of questions and concerns about bodyweight training that keep popping up. Over time, I realised that even though BW training is becoming more popular there are many things people simply need to understand about getting the most from their training. Most of these points I’ve had to learn the hard way through spending a lot of time and energy so I’ve collected them here so you can learn them in a much more efficient manner. After all, that’s what the Red Delta Project is all about, helping you get far more from spending far less. So without further ado, here at 21 things every bodyweight athlete should know about calisthenics: #1 This is still weight lifting. A lot of folks love to debate the differences between bodyweight training and lifting weights. Aside from the specific adaptations between the two, there’s actually very little difference between the two for general strength, muscle building and fitness. A lot of folks forget that BW training is actually a form of weight lifting, only now you’re the weight instead of something external to your body. The only notable difference between the two is that with weight lifting you adjust the weight while keeping the technique relatively consistent and with BW training you adjust the technique while keeping the weight consistent. -

Naval Special Warfare Physical Training Guide
Naval Special Warfare Physical Training Guide DISCLAIMER: Preparation for this training can be equally strenuous. You should consult a physician before you begin any strenuous exer- cise program, such as the one described here, or any diet modification, especially if you have or suspect that you may have heart disease, high blood pressure, diabetes, or any other adverse medical conditions. If you feel faint or dizzy at any time while performing any portion of this training program, stop immediately and seek medical evaluation. The United States Government and any service member or civilian employed by the United States Government disclaims any liability, personal or professional, resulting from the misapplication of any training procedure, technique, or guidance described in this guide. he Naval Special Warfare This guide provides infor- sit-ups as they are necessary TPhysical Training Guide mation about the type of train- for success at BUD/S. Cross- is designed to assist anyone ing required to properly pre- training such as cycling, who wants to improve his fit- pare for the rigors of BUD/S, rowing and hiking is useful to ness in order to take and pass and it offers a tailorable 26- rehabilitate an injury, to add the Physical Screening Test week training plan that should variety or to supplement your (PST) and succeed at Basic help a person with average basic training. Underwater Demolition/SEAL fitness prepare for training Work to improve your (BUD/S). and avoid injury. weakest areas. If you are a Most of your cardio- solid runner but a weak swim- vascular exercise should mer, don’t spend all your time General Training Guidelines focus on running and running just because you are Your workouts should be swimming, and your good at it. -
ACF-Calisthenic-Tech
CALISTHENIC TECHNICAL GUIDE FOREWORD This manual has been written to describe correct technique of Calisthenic positions. It should be noted that this is not a rule book, but a guideline for Accredited Coaches, Assistant Coaches and Cadets. THANKS Are extended to:- Contributing members of the Australian Calisthenic Federation, Australian Calisthenic Federation Coaching Committee Australian Calisthenic Federation Adjudicatorsʼ Advisory Board Australian Calisthenic Federation Examinersʼ Advisory Board And to all others who assisted in the preparation and update of this manual. Photography by Barbara Stavaruk. Layout assistance by Colin Beaton Revised Edition 2004 © ACF 2004 Table of Contents Table of Contents DEPORTMENT .......................................................6 BACKBEND..........................................................24 BANNED AND DANGEROUS MOVEMENTS .........7 LONG SIT .............................................................25 BANNED AND DANGEROUS MOVEMENTS .........8 SITTING POSITIONS............................................25 MOVEMENTS ALLOWABLE WITH CARE ..............8 CROSS LEG SIT ..................................................25 AREAS CAUSING CONCERN................................9 LONG SIT SINGLE LEG RAISE FORWARD ........25 FREE EXERCISES ................................................10 STRADDLE/LEGS ASTRIDE SlT...........................26 ARM POSITIONS..................................................10 BODY RAISE (LONG OR SQUARE) .....................26 FORWARD RAISE ................................................10 -
Bodyweight-Exercises
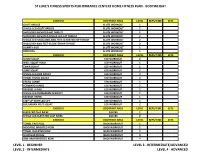
ST LUKE'S FITNESS SPORTS PERFORMANCE CENTERS HOME FITNESS PLAN - BODYWEIGHT EXERCISE BODYPART AREA LEVEL REPS/TIME SETS GLUTE BRIDGE GLUTE WORKOUT 1 SINGLE-LEG GLUTE BRIDGE GLUTE WORKOUT 2 SHOULDER-ELEVATED HIP THRUST GLUTE WORKOUT 1 SHOULDER-ELEVATED SINGLE-LEG HIP THRUST GLUTE WORKOUT 2 SINGLE-LEG SHOULDER-AND-FEET-ELEVATED HIP THRUST GLUTE WORKOUT 2 SHOULDER-AND-FEET-ELEVATED HIP THRUST GLUTE WORKOUT 2 DONKEY KICK GLUTE WORKOUT 1 BIRD DOG GLUTE WORKOUT 1 EXERCISE BODYPART AREA LEVEL REPS/TIME SETS SUMO SQUAT LEG WORKOUT 2 WALL SQUAT HOLD LEG WORKOUT 1 CHAIR SQUAT LEG WORKOUT 1 JUMP SQUAT LEG WORKOUT 2 SINGLE-LEG BOX SQUAT LEG WORKOUT 3 TOWEL PISTOL SQUAT LEG WORKOUT 2 STATIC LUNGE LEG WORKOUT 1 FORWARD LUNGE LEG WORKOUT 2 REVERSE LUNGE LEG WORKOUT 2 SINGLE-LEG ROMANIAN DEADLIFT LEG WORKOUT 1 REVERSE HYPER LEG WORKOUT 1 STEP-UP WITH LEG LIFT LEG WORKOUT 1 BULGARIAN SPLIT SQUAT LEG WORKOUT 2 EXERCISE BODYPART AREA LEVEL REPS/TIME SETS ELEVATED CALF RAISE CALVES 1 SINGLE-LEG ELEVATED CALF RAISE CALVES 2 EXERCISE BODYPART AREA LEVEL REPS/TIME SETS TOWEL FACE PULL BACK WORKOUT 1 MODIFIED INVERTED ROW BACK WORKOUT 2 TOWEL INVERTED ROW BACK WORKOUT 2 SCAPULAR SHRUG BACK WORKOUT 3 ONE-ARM INVERTED ROW BACK WORKOUT 4 LEVEL 1 - BEGINNER LEVEL 3 - INTERMEDIATE/ADVANCED LEVEL 2 - INTERMEDIATE LEVEL 4 - ADVANCED ST LUKE'S FITNESS SPORTS PERFORMANCE CENTERS HOME FITNESS PLAN - BODYWEIGHT EXERCISE BODYPART AREA LEVEL REPS/TIME SETS TORSO ELEVATED PUSH-UP CHEST WORKOUT 1 PUSH-UP CHEST WORKOUT 2 WIDE-WIDTH PUSH-UP CHEST WORKOUT 3 ELEVATED PUSH-UP CHEST -
L G B T Q G B T Q L I 2S
Try the LGBTQI2S movement routine! Here are some examples of exercises you can do following the LGBTQI2S acronym. Share your own version with us @egalecanada! Lunges Leg Raises • Stand with your feet • Lying on your back, together. keep your legs straight • Keeping your upper L L and together. body straight, step • Lift them straight up as forward with one leg, high as you can, and lowering your hips until slowly lower them back both knees are bent at down to the floor. a 90-degree angle. • Rise back up and move the foot you stepped forward with back to its original position. Goblet Squat Glute Bridge • Standing with your • Lying face up on the feet at shoulder-width floor, lift your hips apart, hold an object GG off the ground until against your chest, with your knees, hips, and your elbows tucked in. shoulders form a • As you squat, keep straight line. your heels flat on the • Hold your bridged ground. position for a few • Going as low as you seconds before can before coming lowering your hips to back up, pushing the ground. through your heels. Bicep Curl Bent Over Rows • Ensure your elbows • Stand with your feet are close to your torso shoulder-width apart. and your palms facing B B • Bend your knees forward. and lean forward • Keeping your upper from the waist. Your arm stationary, exhale knees should be bent, as you curl the object but your back stays up to shoulder level straight. while contracting your • Row the object in as biceps. close to your chest as you can. -

Balance Beam Rules Balance Beam
BALANCE BEAM BRONZE SILVER GOLD PLATINUM DIAMOND Value Parts (VP) 6 “A”, 1 ”B” VP 5 A”, 2 ”B” VP Any “A” VP listed in the Any “A” VP listed in the Any “A” or “B” VP listed Any “A” or “B” VP listed Any “A”, “B”, “C” VP Xcel Code of Points. Xcel Code of Points. in the Xcel Code of Points. in the Xcel Code of Points. listed in the Xcel Code of Any skills listed on the Any “B” Dance VP. Any skill listed on the Any “C” Dance VP. Points. Xcel Bronze chart. Any skill listed on the Xcel Gold chart. Xcel Silver chart. Clarifications Cross Split jump = “A” “B” Dance VP allowed. “C” Dance VP allowed. All Acro Skills must start VP. (any split angle) and finish on the beam. Cross Straddle jump = Handstands, regardless “A” VP. (any split angle) of the angle achieved, BALANCE BEAMRULES are considered the Same Skill. SR credit will be awarded for Cross or Side Split Leaps or Jumps that are within 20° of the specified split angle. A deduction of up to 0.20 for insufficient Split will be applied. Difficulty No “B” or higher VP. No “B” Acro VP. Restrictions No Salto or Aerial No “C” or higher VP. No “C” or higher VP. No “C” Acro VP. Dismounts. No “D” or higher VP. No “D” or higher VP. 11 Unallowable Skills No walkovers. 0.5 deduction - off SV Special 1. Min. ½ Turn on 1 or 1. Min. ½ Turn on one 1. Min. 1/1 Turn on one 1. -

Cervical Spine Stretches
Cervical Spine Stretches Purpose: Stretching exercises help to restore joint range of motion by lengthening shortened muscles and connective tissue, which helps to reduce pain and tightness. Instructions: 1. Perform highlighted stretches initially 1-2 x/day, or _______________________________________________ 2. Hold each stretch 30-60 seconds if tolerated for lengthening of muscles; repeat 2-3x/each or _____________ 3. Stretch to your pain-free end point, then breathe deeply through your belly and relax as you exhale. This will encourage maximal range in that stretch. 4. It is best to stretch with a warmed-up body, about the temperature that causes a light sweat. 5. For pain reduction, it is best to stretch tight muscles at night just before going to bed. 6. If it is not tight…DON’T STRETCH IT! When tight muscles are no longer tight, you may decrease frequency to 2-3 times per week. 7. Maintain good, upright posture with all stretches and avoid shrugging your shoulders! FLEXION / EXTENSION SIDEBENDING ROTATION Bring your chin toward your chest; hold. Return to Bend your ear toward your right Turn to look over your right shoulder; upright, then bring your head back; hold. Hold the shoulder while looking straight ahead; hold, then switch sides. Add gentle back of your neck with your hands if you need hold, then alternate. hand pressure at the chin as tolerated more support. for more stretch. SCALENE Sit with your right hand holding edge of chair. UPPER TRAPEZIUS LEVATOR SCAPULAE Place your left hand over your right collarbone Sit with right hand holding edge of Sit with right hand holding edge of chair. -

Level 2 – Week 3 Home Workout (Refer to Video on Nasagym.Com for Help with the Break Down of Skills)
Level 2 – Week 3 Home Workout (Refer to video on nasagym.com for help with the break down of skills) Stretches (hold each 10sec): • Arm circles forward and then backwards • Rock on hands to stretch wrists • Cat stretch • Seal stretch • Butterfly stretch, put nose to toes. • Pike sit with reaching hands to toes • Straddle, reach hands out in front to try and flatten stomach to the ground to be as flat as a pancake • Middle splits (make sure hips are in line with feet) • Right split (try to keep chest up tall) • Left splits (try to keep chest up tall) Conditioning (Complete 2 rounds): • 10 dips (place hands on edge of chair behind you and slide your hips of the edge keeping your legs straight and chest up. Then bend arms making sure not to round back or lean forward. • 20 tuck-ins (sit on bottom and hold knees into chest and then extend straight out in front of you) • 10 push-ups with hands on the couch, a stair or the ground. • 30 sec wall sit (place weights or books on your lap and hold your arms straight above your head for an extra challenge) • 15 frog jumps • 20 flipper kicks Floor Skills (only if you have a large floor space with a mat or grass to practice on): • Place duct tape on grass or draw a chalk line or fold up a towel burrito style so its only about 4-6 inches wide and use the straight line to do a cartwheel on. Make sure to start and finish in a lunge. -

Training Inventory Revised
Training Components and Exercise Circuits (page 1) www.sacspeed.com Warmup Preparatory Routines Static Flexibility Routines Mobility Jog Circuit Capella Rigel Weave Hansen’s Back Series (L-R) Chest Hang Backwards Run Spinal Roll Deep Squat Side Shuffle Right Hands Behind Back Lateral Squat (L-R) Side Shuffle Left Elbow/Obliques (L-R) Spinal Roll-Push Arm Circles Calf Stretch (Straight/Flexed, L-R) Spinal Roll-Pull (switch) Arms Across Split Stretch (L-R) Butterfly Skip Lunges Heel Sit Seated Arm Pull (switch) Crossover Run Seated Straddle (M-L-R) Quadriceps Stretch Butterfly Quadriceps Lift (L-R) Dynamic Flexibility Routines Figure 4/Pretzel (L-R) Shoulder Lift (switch) Sirius Vega Arcturus Thrower’s Series Eagles (Back/Front) Eagles (Back/Front) Lead/Trail Leg Lifts Tube Over Splits/Scissors w/ Rollover Leg Swings (Sagittal/Frontal, L-R) Bicycle/ Backward Bicycle w/ Rollover Tube Under Single Knee Tucks Hurdle Trail Leg Circles (L-R) Roll/Rollback Tube Side Hip Circles (CW-CCW) Double Knee Tucks Tube Across Double Arm Circles (CW-CCW) Single Arm Circles (CW-CCW, L-R) Weighted Trunk Twists Leg Swings (Sagittal/Frontal, L-R) Hurdle Trail Leg Circles (L-R) Weighted Bentover Swings Donkey Kicks/Leg Whips/Trail Leg Lifts (L-R) Hurdle Seat Exchange Weighted Arm Circles (CW-CCW) Lunge Exchange (Straight/Side) Weighted Wrist Twists Sprint Development Drill Series Cygnus Pegasus Aquila Draco Hurdle Skill A Skips Highknees Side A Skips (L-R) A Skips A Skips B Skips Buttkicks Backwards Skips Straight Leg Bounds B Skips (L-R) Backward Skips Crossovers