National Rabies Prevention and Control Program Manual of Operations (2012)
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Inspection Bukidnon
INSPECTION BUKIDNON Name of Establishment Address No. of Type of Industry Type of Condition Workers 1 AGLAYAN PETRON SERVICE CENTER POB. AGLAYAN, MALAYBALAY CITY 15 RETAIL HAZARDOUS 2 AGT MALAYBALAY PETRON (BRANCH) SAN VICENTE ST., MALAYBALAY CITY 10 RETAIL HAZARDOUS 3 AGT PETRON SERVICE CENTER SAN JOSE, MALAYBALAY CITY 15 RETAIL HAZARDOUS 4 AIDYL STORE POB. MALAYBALAY CITY 13 RETAIL HAZARDOUS 5 ALAMID MANPOWER SERVICES POB. AGLAYAN, MALAYBALAY CITY 99 NON-AGRI NON-HAZARDOUS 6 ANTONIO CHING FARM STA. CRUZ, MALAYBALAY CITY 53 AGRI HAZARDOUS 7 ASIAN HILLS BANK, INC. FORTICH ST., MALAYBALAY CITY 21 AGRI NON-HAZARDOUS 8 BAKERS DREAM (G. TABIOS BRANCH) T. TABIOS ST., MALAYBALAY CITY 10 RETAIL NON-HAZARDOUS 9 BAO SHENG ENTERPRISES MELENDES ST., MALAYBALAY CITY 10 RETAIL NON-HAZARDOUS 10 BELLY FARM KALASUNGAY, MALAYBALAY CITY 13 AGRI HAZARDOUS 11 BETHEL BAPTIST CHURCH SCHOOL FORTICH ST., MALAYBALAY CITY 19 PRIV. SCH NON-HAZARDOUS 12 BETHEL BAPTIST HOSPITAL SAYRE HIWAY, MALAYBALAY CITY 81 HOSPITAL NON-HAZARDOUS NON-HAZARDOUS 13 BUGEMCO LEARNING CENTER SAN VICTORES ST., MALAYBALAY CITY 10 PRIV. SCH GUILLERMO FORTICH ST., 14 BUKIDNON PHARMACY COOPERATIVE MALAYBALAY CITY 11 RETAIL NON-HAZARDOUS 15 CAFE CASANOVA (BRANCH) MAGSAYSAY ST., MALAYBALAY CITY 10 SERVICE NON-HAZARDOUS 16 CASCOM COMMERCIAL POB. AGLAYAN, MALAYBALAY CITY 30 RETAIL NON-HAZARDOUS CASISNG CHRISTIAN SCHOOL OF M NON-HAZARDOUS 17 MALAYBALAY CASISANG, MALAYBALAY CITY 34 PRIV. SCH A 18 CEBUANA LHUILLIER PAWNSHOP FORTICH ST., MALAYBALAY CITY 10 FINANCING NON-HAZARDOUS L 19 CELLUCOM DEVICES -
Nd Drrm C Upd Date
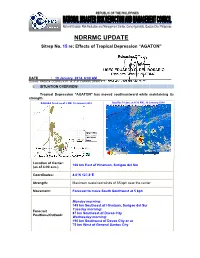
NDRRMC UPDATE Sitrep No. 15 re: Effects of Tropical Depression “AGATON” Releasing Officer: USEC EDUARDO D. DEL ROSARIO Executive Director, NDRRMC DATE : 19 January 2014, 6:00 AM Sources: PAGASA, OCDRCs V,VII, IX, X, XI, CARAGA, DPWH, PCG, MIAA, AFP, PRC, DOH and DSWD I. SITUATION OVERVIEW: Tropical Depression "AGATON" has moved southeastward while maintaining its strength. PAGASA Track as of 2 AM, 19 January 2014 Satellite Picture at 4:32 AM., 19 January 2014 Location of Center: 166 km East of Hinatuan, Surigao del Sur (as of 4:00 a.m.) Coordinates: 8.0°N 127.8°E Strength: Maximum sustained winds of 55 kph near the center Movement: Forecast to move South Southwest at 5 kph Monday morninng: 145 km Southeast of Hinatuan, Surigao del Sur Tuesday morninng: Forecast 87 km Southeast of Davao City Positions/Outlook: Wednesday morning: 190 km Southwest of Davao City or at 75 km West of General Santos City Areas Having Public Storm Warning Signal PSWS # Mindanao Signal No. 1 Surigao del Norte (30-60 kph winds may be expected in at Siargao Is. least 36 hours) Surigao del Sur Dinagat Province Agusan del Norte Agusan del Sur Davao Oriental Compostela Valley Estimated rainfall amount is from 5 - 15 mm per hour (moderate - heavy) within the 300 km diameter of the Tropical Depression Tropical Depression "AGATON" will bring moderate to occasionally heavy rains and thunderstorms over Visayas Sea travel is risky over the seaboards of Luzon and Visayas. The public and the disaster risk reduction and management councils concerned are advised to take appropriate actions II. -

Sustainable Agricultural Production Systems for Food Security in a Changing Climate in Batanes, Philippines
Journal of Developments in Sustainable Agriculture 9: 111-119 (2014) Sustainable Agricultural Production Systems for Food Security in a Changing Climate in Batanes, Philippines Lucille Elna P. de Guzman1, Oscar B. Zamora1, 2,JoanPaulineP.Talubo3* and Cesar Doroteo V. Hostallero4 1 Crop Science Cluster, College of Agriculture, University of the Philippines Los Baños 2 Office of the Vice-Chancellor for Academic Affairs, University of the Philippines Los Baños 3 Department of Community and Environmental Resource Planning, College of Human Ecology, University of the Philippines Los Baños 4 Office of the Provincial Agriculturist, Basco, Batanes, Philippines Climate change could have significant impacts in the Philippines on large sections of the population who are poor and vulnerable, especially those who live in areas prone to coastal storms, drought and sea level rise. The sectors mostly affected by climate change are agriculture and food security because of the risk of low productivity due to increasing temperature, drought, and increasing frequency and intensity of rainfall that brings about floods and land- slides. Located in the northernmost tip of the country, the Batanes group of islands lies on the country’s typhoon belt. Because of vulnerability and isolation from the rest of the archipelago, the Ivatans have developed self-sufficient, organic and climate-resilient crop production systems. This paper presents the indigenous crop production systems that have made the Ivatans food self-sufficient despite vulnerability of their agroecosystem. A typical Ivatan farmer owns 3-7 parcels of land. Each parcel has an average size of 300-500 m2.Farmers practice a rootcrop-based multiple cropping system with specific spatial arrangements of corn (Zea mays), gabi (Colocasia esculenta), yam (Dioscorea alata) and tugui (Dioscorea esculenta), using corn stover, hardwood trees or a local reed called viyawu (Miscanthus sp.) as trellis. -

Cost of Doing Business in the Province of Iloilo 2017 1
COST OF DOING BUSINESS IN THE PROVINCE OF ILOILO 2017 Cost of Doing Business in the Province of Iloilo 2017 1 2 Cost of Doing Business in the Province of Iloilo 2017 F O R E W O R D The COST OF DOING BUSINESS is Iloilo Provincial Government’s initiative that provides pertinent information to investors, researchers, and development planners on business opportunities and investment requirements of different trade and business sectors in the Province This material features rates of utilities, such as water, power and communication rates, minimum wage rates, government regulations and licenses, taxes on businesses, transportation and freight rates, directories of hotels or pension houses, and financial institutions. With this publication, we hope that investors and development planners as well as other interested individuals and groups will be able to come up with appropriate investment approaches and development strategies for their respective undertakings and as a whole for a sustainable economic growth of the Province of Iloilo. Cost of Doing Business in the Province of Iloilo 2017 3 4 Cost of Doing Business in the Province of Iloilo 2017 TABLE OF CONTENTS Foreword I. Business and Investment Opportunities 7 II. Requirements in Starting a Business 19 III. Business Taxes and Licenses 25 IV. Minimum Daily Wage Rates 45 V. Real Property 47 VI. Utilities 57 A. Power Rates 58 B. Water Rates 58 C. Communication 59 1. Communication Facilities 59 2. Land Line Rates 59 3. Cellular Phone Rates 60 4. Advertising Rates 61 5. Postal Rates 66 6. Letter/Cargo Forwarders Freight Rates 68 VII. -

Top 15 Lgus with Highest Poverty Incidence, Davao Region, 2012)
Table 1. City and Municipal-Level Small Area Poverty Estimates (Top 15 LGUs with Highest Poverty Incidence, Davao Region, 2012) Rank Province Municipality Poverty Incidence (%) 1 Davao Occidental Jose Abad Santos (Trinidad) 75.5 2 Davao Occidental Don Marcelino 73.8 3 Davao del Norte Talaingod 68.8 4 Davao Occidental Saragani 65.9 5 Davao Occidental Malita 60.8 6 Davao Oriental Manay 58.1 7 Davao Oriental Tarragona 56.9 8 Compostela Valley Laak (San Vicente) 53.8 9 Davao del Sur Kiblawan 52.9 10 Davao Oriental Caraga 51.6 11 Davao Occidental Santa Maria 50.7 12 Davao del Norte San Isidro 43.2 13 Davao del Norte New Corella 41.6 14 Compostela Valley Montevista 40.2 15 Davao del Norte Asuncion (Saug) 39.2 Source: Philippine Statistics Authority Note: The 2015 Small Area Poverty Estimates is not yet available. Table 2. Geographically-Isolated and Disadvantaged Areas (GIDAs) PROVINCE/HUC CITY/MUNICIPALITY BARANGAYS Baganga Binondo, Campawan, Mahan-ob Boston Caatihan, Simulao Caraga Pichon, Sobreacrey, San Pedro Cateel Malibago Davao Oriental Gov. Generoso Ngan Lupon Don Mariano, Maragatas, Calapagan Manay Taokanga, Old Macopa Mati City Langka, Luban, Cabuaya Tarragona Tubaon, Limot Asuncion Camansa, Binancian, Buan, Sonlon IGaCoS Pangubatan, Bandera, San Remegio, Libertad, San Isidro, Aundanao, Tagpopongan, Kanaan, Linosutan, Dadatan, Sta. Cruz, Cogon Davao del Norte Kapalong Florida, Sua-on, Gupitan San Isidro Monte Dujali, Datu Balong, Dacudao, Pinamuno Sto. Tomas Magwawa Talaingod Palma Gil, Sto. Niño, Dagohoy Laak Datu Ampunan, Datu Davao Mabini Anitapan, Golden Valley Maco Calabcab, Elizalde, Gubatan, Kinuban, Limbo, Mainit, Malamodao, Masara, New Barili, New Leyte, Panangan, Panibasan, Panoraon, Tagbaros, Teresa Maragusan Bahi, Langgawisan Compostela Valley Monkayo Awao, Casoon, Upper Ulip. -

Sanitary Landfills Region Province LGU Location 1 Ilocos Norte Bacarra Brgy
Sanitary Landfills Region Province LGU Location 1 Ilocos Norte Bacarra Brgy. Durepes Pungto 1 Ilocos Norte Banna (Espiritu) Brgy. Bangsar 1 Ilocos Norte Nueva Era Brgy. Poblacion 1 Ilocos Norte Piddig Brgy. Abucay 1 Ilocos Norte Vintar Brgy. Parparoroc (14 Ester) 1 Ilocos Sur Candon City Brgy. Balingaoan 1 Ilocos Sur Narvacan Brgy. Dasay 1 La Union Agoo Brgy. San Agustin Norte 1 La Union Bangar Brgy. Cadapli 1 La Union Balaoan Brgy. Calumbayan 1 La Union Naguilian Brgy. Cabaritan Norte 1 La Union Rosario Brgy. Inabaan Norte 1 La Union Santol Brgy. 1 La Union San Gabriel Brgy. 1 La Union San Fernando City Brgy. Mameltac 1 La Union Sudipen Brgy. Seng-ngat 1 La Union Luna Brgy. Suroc Norte 1 Pangasinan Bolinao Brgy. Balingasay 1 Pangasinan Urdaneta City Brgy Catablan 2 Cagayan Lal-lo Brgy. Cagoran 2 Isabela Quezon Sitio Namnama, Brgy. Santos 2 Nueva Vizcaya Aritao Brgy. Kirang 2 Nueva Vizcaya Bagabag Sitio Tapaya, Brgy. Baretbet 2 Nueva Vizcaya Bayombong Boundary of Brgy. Upper Magsaysay and Upper Busilac 2 Nueva Vizcaya Solano Brgy. Concepion 3 Aurora Dipaculao Brgy. Toytoyan 3 Aurora Maria Aurora Brgy. San Joanquin 3 Bulacan San Jose del Monte City Brgy. Minuyan (Alejandro Waste Mgt. Inc.) 3 Bulacan Norzagaray Sitio Coral, Brgy. Matictic 3 Bulacan Norzagaray Sitio Tiakad, Brgy. San Mateo (Wacuman Inc.) 3 Nueva Ecija Santa Rosa Brgy. Mapalad 3 Nueva Ecija Palayan City MetroBrgy. Atate Clark (EcoSci Waste Corp.)Mgt. Corp., Sub-zone Kalangitan, Clark Special 3 Tarlac Capas Economic Zone 4a Batangas Alitagtag Brgy. San Juan 4a Batangas Batangas City Waste Garde - Brgy. -

Press Release
PRESS RELEASE Highlights of the Region II (Cagayan Valley) Population 2020 Census of Population and Housing (2020 CPH) Date of Release: 20 August 2021 Reference No. 2021-317 • The population of Region II - Cagayan Valley as of 01 May 2020 is 3,685,744 based on the 2020 Census of Population and Housing (2020 CPH). This accounts for about 3.38 percent of the Philippine population in 2020. • The 2020 population of the region is higher by 234,334 from the population of 3.45 million in 2015, and 456,581 more than the population of 3.23 million in 2010. Moreover, it is higher by 872,585 compared with the population of 2.81 million in 2000. (Table 1) Table 1. Total Population Based on Various Censuses: Region II - Cagayan Valley Census Year Census Reference Date Total Population 2000 May 1, 2000 2,813,159 2010 May 1, 2010 3,229,163 2015 August 1, 2015 3,451,410 2020 May 1, 2020 3,685,744 Source: Philippine Statistics Authority • The population of Region II increased by 1.39 percent annually from 2015 to 2020. By comparison, the rate at which the population of the region grew from 2010 to 2015 was lower at 1.27 percent. (Table 2) Table 2. Annual Population Growth Rate: Region II - Cagayan Valley (Based on Various Censuses) Intercensal Period Annual Population Growth Rate (%) 2000 to 2010 1.39 2010 to 2015 1.27 2015 to 2020 1.39 Source: Philippine Statistics Authority PSA Complex, East Avenue, Diliman, Quezon City, Philippines 1101 Telephone: (632) 8938-5267 www.psa.gov.ph • Among the five provinces comprising Region II, Isabela had the biggest population in 2020 with 1,697,050 persons, followed by Cagayan with 1,268,603 persons, Nueva Vizcaya with 497,432 persons, and Quirino with 203,828 persons. -

Philippine Port Authority Contracts Awarded for CY 2018
Philippine Port Authority Contracts Awarded for CY 2018 Head Office Project Contractor Amount of Project Date of NOA Date of Contract Procurement of Security Services for PPA, Port Security Cluster - National Capital Region, Central and Northern Luzon Comprising PPA Head Office, Port Management Offices (PMOs) of NCR- Lockheed Global Security and Investigation Service, Inc. 90,258,364.20 27-Nov-19 23-Dec-19 North, NCR-South, Bataan/Aurora and Northern Luzon and Terminal Management Offices (TMO's) Ports Under their Respective Jurisdiction Proposed Construction and Offshore Installation of Aids to Marine Navigation at Ports of JARZOE Builders, Inc./ DALEBO Construction and General. 328,013,357.76 27-Nov-19 06-Dec-19 Estancia, Iloilo; Culasi, Roxas City; and Dumaguit, New Washington, Aklan Merchandise/JV Proposed Construction and Offshore Installation of Aids to Marine Navigation at Ports of Lipata, Goldridge Construction & Development Corporation / JARZOE 200,000,842.41 27-Nov-19 06-Dec-19 Culasi, Antique; San Jose de Buenavista, Antique and Sibunag, Guimaras Builders, Inc/JV Consultancy Services for the Conduct of Feasibility Studies and Formulation of Master Plans at Science & Vision for Technology, Inc./ Syconsult, INC./JV 26,046,800.00 12-Nov-19 16-Dec-19 Selected Ports Davila Port Development Project, Port of Davila, Davila, Pasuquin, Ilocos Norte RCE Global Construction, Inc. 103,511,759.47 24-Oct-19 09-Dec-19 Procurement of Security Services for PPA, Port Security Cluster - National Capital Region, Central and Northern Luzon Comprising PPA Head Office, Port Management Offices (PMOs) of NCR- Lockheed Global Security and Investigation Service, Inc. 90,258,364.20 23-Dec-19 North, NCR-South, Bataan/Aurora and Northern Luzon and Terminal Management Offices (TMO's) Ports Under their Respective Jurisdiction Rehabilitation of Existing RC Pier, Port of Baybay, Leyte A. -

CANDON CITY, ILOCOS SUR Geographic Profile the City of Candon Is a “C”-Shaped Landmass
Uses of CBMS on Local Planning and Revenue Allocation in CANDON CITY, ILOCOS SUR Geographic Profile THE City of Candon is a “C”-shaped landmass located along the shores of Ilocos Sur measuring of 10,328 hectares of land area 42 barangays – 4 urban and 38 rural Geographic Profile LAOAG It is situated south of CITY Laoag City (132 kms.) North of the City of San Fernando, La Union (72 kms.) CANDON CITY Baguio (100 kms.) SAN FERNANDO CITY BAGUIO CITY Geographic Profile CANDON CITY CANDON CITY TO MANILA (347 kms) MANILA Geographic Profile As a coastal city in the Ilocos Region (Region I), it has great potentials to become a sub-regional growth center in complement with the regional growth hub of San Fernando City, La Union. Geographic Profile It has become also the center for trade in Southern Ilocos as it serves about 15 nearby towns in the provinces of Ilocos Sur, La Union and Abra Geographic Profile due to the fact that a 12 kms. stretch of the National Highway traverses the city and it is the only entry point towards the eastern upland towns of the 2nd District of Ilocos Sur Geographic Profile Comprising of mountains and hills in the east a bountiful farmland plains in the center a 16-kilometers shoreline the City of Candon has diverse natural resources and a solid agriculture-based economy. Boundaries Mun. of Mun. of Santiago Banayoyo S Mun. of Mun. of O Lidlidda San Emilio U T H Mun. of C Galimuyod H I Mun. of Salcedo N A S E Mun. -
Cagayan Riverine Zone Development Framework Plan 2005—2030
Cagayan Riverine Zone Development Framework Plan 2005—2030 Regional Development Council 02 Tuguegarao City Message The adoption of the Cagayan Riverine Zone Development Framework Plan (CRZDFP) 2005-2030, is a step closer to our desire to harmonize and sustainably maximize the multiple uses of the Cagayan River as identified in the Regional Physical Framework Plan (RPFP) 2005-2030. A greater challenge is the implementation of the document which requires a deeper commitment in the preservation of the integrity of our environment while allowing the development of the River and its environs. The formulation of the document involved the wide participation of concerned agencies and with extensive consultation the local government units and the civil society, prior to its adoption and approval by the Regional Development Council. The inputs and proposals from the consultations have enriched this document as our convergence framework for the sustainable development of the Cagayan Riverine Zone. The document will provide the policy framework to synchronize efforts in addressing issues and problems to accelerate the sustainable development in the Riverine Zone and realize its full development potential. The Plan should also provide the overall direction for programs and projects in the Development Plans of the Provinces, Cities and Municipalities in the region. Let us therefore, purposively use this Plan to guide the utilization and management of water and land resources along the Cagayan River. I appreciate the importance of crafting a good plan and give higher degree of credence to ensuring its successful implementation. This is the greatest challenge for the Local Government Units and to other stakeholders of the Cagayan River’s development. -

Iloilo Provincial Profile 2012
PROVINCE OF ILOILO 2012 Annual Provincial Profile TIUY Research and Statistics Section i Provincial Planning and Development Office PROVINCE OF ILOILO 2012 Annual Provincial Profile P R E F A C E The Annual Iloilo Provincial Profile is one of the endeavors of the Provincial Planning and Development Office. This publication provides a description of the geography, the population, and economy of the province and is designed to principally provide basic reference material as a backdrop for assessing future developments and is specifically intended to guide and provide data/information to development planners, policy makers, researchers, private individuals as well as potential investors. This publication is a compendium of secondary socio-economic indicators yearly collected and gathered from various National Government Agencies, Iloilo Provincial Government Offices and other private institutions. Emphasis is also given on providing data from a standard set of indicators which has been publish on past profiles. This is to ensure compatibility in the comparison and analysis of information found therewith. The data references contained herewith are in the form of tables, charts, graphs and maps based on the latest data gathered from different agencies. For more information, please contact the Research and Statistics Section, Provincial Planning & Development Office of the Province of Iloilo at 3rd Floor, Iloilo Provincial Capitol, and Iloilo City with telephone nos. (033) 335-1884 to 85, (033) 509-5091, (Fax) 335-8008 or e-mail us at [email protected] or [email protected]. You can also visit our website at www.iloilo.gov.ph. Research and Statistics Section ii Provincial Planning and Development Office PROVINCE OF ILOILO 2012 Annual Provincial Profile Republic of the Philippines Province of Iloilo Message of the Governor am proud to say that reform and change has become a reality in the Iloilo Provincial Government. -

Actual Census Pop. 2015 2017 2018 2019 2020 2021 REGION V
Total Population by Province, City, Municipality and Barangay: Actual Census Pop. 2015 2017 2018 2019 2020 2021 REGION V - BICOL REGION 5,796,989 6,266,652 6,387,680 6,511,148 6,637,047 6,766,622 ALBAY 1,314,826 1,404,477 1,428,207 1,452,261 1,476,639 1,501,348 0.033530 0.027955 0.025166 0.023484 0.022356 BACACAY 68,906 73,604 74,848 76,109 77,386 78,681 Baclayon 2,703 2,887 2,936 2,986 3,036 3,086 Banao 1,491 1,593 1,620 1,647 1,674 1,703 Bariw 625 668 679 690 702 714 Basud 1,746 1,865 1,897 1,929 1,961 1,994 Bayandong 1,650 1,763 1,792 1,822 1,853 1,884 Bonga (Upper) 7,649 8,171 8,309 8,449 8,590 8,734 Buang 1,337 1,428 1,452 1,477 1,502 1,527 Cabasan 2,028 2,166 2,203 2,240 2,278 2,316 Cagbulacao 862 921 936 952 968 984 Cagraray 703 751 764 776 790 803 Cajogutan 1,130 1,207 1,227 1,248 1,269 1,290 Cawayan 1,247 1,332 1,355 1,377 1,400 1,424 Damacan 431 460 468 476 484 492 Gubat Ilawod 1,080 1,154 1,173 1,193 1,213 1,233 Gubat Iraya 1,159 1,238 1,259 1,280 1,302 1,323 Hindi 3,800 4,059 4,128 4,197 4,268 4,339 Igang 2,332 2,491 2,533 2,576 2,619 2,663 Langaton 765 817 831 845 859 874 Manaet 836 893 908 923 939 955 Mapulang Daga 453 484 492 500 509 517 Mataas 518 553 563 572 582 591 Misibis 1,007 1,076 1,094 1,112 1,131 1,150 Nahapunan 402 429 437 444 451 459 Namanday 1,482 1,583 1,610 1,637 1,664 1,692 Namantao 778 831 845 859 874 888 Napao 1,883 2,011 2,045 2,080 2,115 2,150 Panarayon 1,848 1,974 2,007 2,041 2,075 2,110 Pigcobohan 817 873 887 902 918 933 Pili Ilawod 1,522 1,626 1,653 1,681 1,709 1,738 Pili Iraya 997 1,065 1,083 1,101