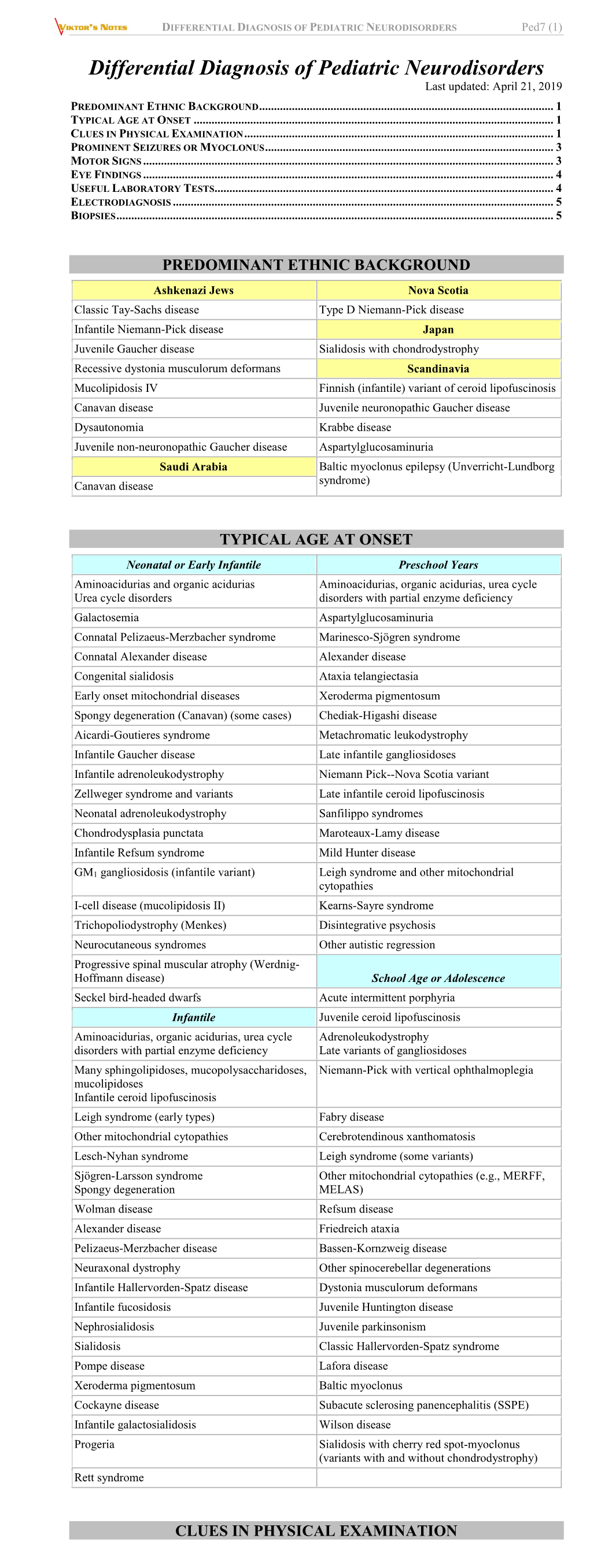
DIFFERENTIAL DIAGNOSIS of PEDIATRIC NEURODISORDERS Ped7 (1)
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Newborn Screening for X-Linked Adrenoleukodystrophy: Information for Parents
Newborn Screening for X-linked Adrenoleukodystrophy: Information for Parents Baby girl with ABCD1 gene mutation What is newborn screening? the symptoms of ALD during childhood. Rarely, some women who are carriers of ALD develop mild symptoms as adults. It Newborn screening involves laboratory testing on a small is important for your family to meet with a genetic counselor sample of blood collected from newborns’ heels. Every state to talk about the genetics of ALD and implications for other has a newborn screening program to identify infants with rare family members. disorders, which would not usually be detected at birth. Early diagnosis and treatment of these disorders often prevents Why do only boys have ALD? serious complications. Only boys have ALD because it is caused by a mutation in What is adrenoleukodystrophy (ALD)? a gene (ABCD1) on the X chromosome, called “X-linked inheritance.” Males only have one X chromosome so they have ALD is one of over 40 disorders included in newborn screening one ABCD1 gene. Males with a nonfunctioning ABCD1 gene in New York State. It is a rare genetic disorder. People with have ALD. Females have 2 X chromosomes, so they have two ALD are unable to breakdown a component of food called ABCD1 genes. Females with one ABCD1 gene mutation will very long chain fatty acids (VLCFA). If VLCFA are not broken be carriers. When a mother is a carrier of ALD, each son has a down, they build up in the body and cause symptoms. 50% chance of inheriting the disorder and each daughter has a 50% chance of being a carrier. -

Inheritance of Multiple Epiphyseal Dysplasia, Tarda
Inheritance of Multiple Epiphyseal Dysplasia, Tarda RICHARD C. JUBERG1 AND JOHN F. HOLT2 Multiple epiphyseal dysplasia, tarda, a modeling error of the epiphyses, is charac- terized by shortness of stature and micromelia, particularly stubby hands (Rubin, 1964). A patient with this trait generally shows satisfactory development, adequate muscle mass, and normal intelligence. As a rule, there are few complaints of joint discomfort during childhood. Eventually, however, problems arise from joint motion, which lead to difficulty in walking because of pain in the hips, knees, or ankles. De- formities may result. On the other hand, the defect may not be recognized until the patient presents manifestations of degenerative arthritis at an unusually early age. The classification of epiphyseal modeling errors by Rubin (1964) contains six different entities. Spondyloepiphyseal dysplasia, congenita (Morquio's disease) is characterized by irregularity of epiphyses and vertebrae. It is an abnormality of mucopolysaccharide metabolism, and it is transmitted as an autosomal recessive. Multiple epiphyseal dysplasia, congenita (stippled epiphyses) is characterized by stippled or punctate epiphyses, and it too is transmitted as an autosomal recessive. Epiphyseal retardation, which occurs in cretinism (hypothyroidism), may result from any of several different metabolic errors which appear to be transmitted as autosomal recessives (Stanbury, 1966). Diastrophic dwarfism results in delayed appearance of epiphyses and joint luxations, and this, too, apparently is transmitted as an autosomal recessive. Multiple epiphyseal dysplasia, tarda, which is also known in the literature as epi- physeal dysplasia multiplex, must be differentiated from spondyloepiphyseal dys- plasia, tarda. As the name implies, one difference is in the extent and severity of spinal involvement as well as in the changes in the epiphyses of the long tubular bones. -

Diseases of the Digestive System (KOO-K93)
CHAPTER XI Diseases of the digestive system (KOO-K93) Diseases of oral cavity, salivary glands and jaws (KOO-K14) lijell Diseases of pulp and periapical tissues 1m Dentofacial anomalies [including malocclusion] Excludes: hemifacial atrophy or hypertrophy (Q67.4) K07 .0 Major anomalies of jaw size Hyperplasia, hypoplasia: • mandibular • maxillary Macrognathism (mandibular)(maxillary) Micrognathism (mandibular)( maxillary) Excludes: acromegaly (E22.0) Robin's syndrome (087.07) K07 .1 Anomalies of jaw-cranial base relationship Asymmetry of jaw Prognathism (mandibular)( maxillary) Retrognathism (mandibular)(maxillary) K07.2 Anomalies of dental arch relationship Cross bite (anterior)(posterior) Dis to-occlusion Mesio-occlusion Midline deviation of dental arch Openbite (anterior )(posterior) Overbite (excessive): • deep • horizontal • vertical Overjet Posterior lingual occlusion of mandibular teeth 289 ICO-N A K07.3 Anomalies of tooth position Crowding Diastema Displacement of tooth or teeth Rotation Spacing, abnormal Transposition Impacted or embedded teeth with abnormal position of such teeth or adjacent teeth K07.4 Malocclusion, unspecified K07.5 Dentofacial functional abnormalities Abnormal jaw closure Malocclusion due to: • abnormal swallowing • mouth breathing • tongue, lip or finger habits K07.6 Temporomandibular joint disorders Costen's complex or syndrome Derangement of temporomandibular joint Snapping jaw Temporomandibular joint-pain-dysfunction syndrome Excludes: current temporomandibular joint: • dislocation (S03.0) • strain (S03.4) K07.8 Other dentofacial anomalies K07.9 Dentofacial anomaly, unspecified 1m Stomatitis and related lesions K12.0 Recurrent oral aphthae Aphthous stomatitis (major)(minor) Bednar's aphthae Periadenitis mucosa necrotica recurrens Recurrent aphthous ulcer Stomatitis herpetiformis 290 DISEASES OF THE DIGESTIVE SYSTEM Diseases of oesophagus, stomach and duodenum (K20-K31) Ill Oesophagitis Abscess of oesophagus Oesophagitis: • NOS • chemical • peptic Use additional external cause code (Chapter XX), if desired, to identify cause. -

Zellweger Syndrome: Biochemical and Morphological Studies on Two Patients Treated with Clofibrate
003 1-3998/85/19 12-1356$02.00/0 PEDIATRIC RESEARCH Vol. 19, No. 12, 1985 Copyright O 1985 International Pediatric Research Foundation, Inc. Printed in (I.S. A. Zellweger Syndrome: Biochemical and Morphological Studies on Two Patients Treated with Clofibrate PAUL B. LAZAROW, VIRGINIA BLACK, HELEN SHIO, YUKIO FUJIKI, AMIYA K. HAJRA, NABANITA S. DATTA, BABU S. BANGARU, AND JOSEPH DANCIS The Rockefiller University, 1230 York Avenue, New York, New York 10021 [P.B.L., H.S., Y.F.] Departments of Cell Biology [V.B.] and Pediatrics [B.S.B., J.D.], New York University School of Medicine, 550 First Avenue, New York, NY 10016; and Neuroscience Laboratory, The University of Michigan, Ann Arbor, Michigan 48109 [A.K.H., N.S.D.] ABSTRACT. Two infants with Zellweger syndrome (cer- genetic change, which is implied by the observed autosomal ebro-hepato-renal syndrome) have been studied bio- recessive mode of inheritance (2)? The functions of peroxisomes chemically and morphologically. Peroxisomal enzymes in- include respiration (forming HZ02)(12), fatty acid catabolism volved in respiration, fatty acid @-oxidation,and plasmal- (13, 14), and the initial steps in plasmalogen biosynthesis (15). ogen biosynthesis were assessed. In liver, catalase was The peroxisomal fatty acid P-oxidation system acts on saturated present in normal amounts but was located in the cell and unsaturated fatty acyl-CoAs with chainlengths from 6 to 26 cytosol. Dihydroxyacetone phosphate acyltransferase ac- (14, 16, 17), the sidechain of cholesterol (18), dicarboxylic fatty tivity was less than one-tenth of normal. The amount of acids (l9), and glutaryl-CoA (20). -

Peroxisomal Bifunctional Enzyme Deficiency
Peroxisomal bifunctional enzyme deficiency. P A Watkins, … , A B Moser, M E Beard J Clin Invest. 1989;83(3):771-777. https://doi.org/10.1172/JCI113956. Research Article Peroxisomal function was evaluated in a male infant with clinical features of neonatal adrenoleukodystrophy. Very long chain fatty acid levels were elevated in both plasma and fibroblasts, and beta-oxidation of very long chain fatty acids in cultured fibroblasts was significantly impaired. Although the level of the bile acid intermediate trihydroxycoprostanoic acid was slightly elevated in plasma, phytanic acid and L-pipecolic acid levels were normal, as was plasmalogen synthesis in cultured fibroblasts. The latter three parameters distinguish this case from classical neonatal adrenoleukodystrophy. In addition, electron microscopy and catalase subcellular distribution studies revealed that, in contrast to neonatal adrenoleukodystrophy, peroxisomes were present in the patient's tissues. Immunoblot studies of peroxisomal beta- oxidation enzymes revealed that the bifunctional enzyme (enoyl-CoA hydratase/3-hydroxyacyl-CoA dehydrogenase) was deficient in postmortem liver samples, whereas acyl-CoA oxidase and the mature form of beta-ketothiolase were present. Density gradient centrifugation of fibroblast homogenates confirmed that intact peroxisomes were present. Immunoblots of fibroblasts peroxisomal fractions showed that they contained acyl-CoA oxidase and beta-ketothiolase, but bifunctional enzyme was not detected. Northern analysis, however, revealed that mRNA coding for the bifunctional enzyme was present in the patient's fibroblasts. These results indicate that the primary biochemical defect in this patient is a deficiency of peroxisomal bifunctional enzyme. It is of interest that the phenotype of this patient resembled neonatal adrenoleukodystrophy and would not have been […] Find the latest version: https://jci.me/113956/pdf Peroxisomal Bifunctional Enzyme Deficiency Paul A. -

Zellweger Spectrum Disorder
ZELLWEGER SPECTRUM DISORDER What is it? Zellweger Spectrum Disorder (ZSD) was recently viewed as 3 separate diseases but today is categorized as set of disorders that form a spectrum, or continuum, of 1 disease. This spectrum can range from mild Infantile Refsum Disease (IRD), to moderate Neonatal Adrenoleukodystrophy (NALD), to severe Zellweger Syndrome (ZS) ZSD is also known as peroxisome biogenesis disorders (PBDs). These disorders are caused by a loss of function in important parts of your cells called “peroxisomes,” which are responsible for breaking down fats and chemicals and getting rid of waste so that your body can function properly. This disorder can affect many parts of the body from the eyes to the liver. The various body systems and functions as described below. Nutrition Malabsorption of nutrients can lead to poor growth, feeding problems, and deficiency in fat-soluble vitamins. Hearing Varying degree of hearing loss requires the child receive a yearly evaluation . Vision Vision loss is the most common problem. Neurological Improper development of the white matter in the brain (leukodystrophy) results in nerve damage and can potentially affect their development. Damage to the nerves that send information from the brain to the rest of the body (peripheral neuropathy) can often cause numbness or weakness in the hands and/or feet. Walking abnormality is the main neurological complication in adults with ZSDs. In people with mild forms of ZSDs, nerve damage to the muscles, skin, and internal organs usually begins during adolescence. Kidney Kidney issues occur in children 4 years and older and include kidney stones, kidney cyst, and kidney failure. -

Congenital Abnormalities Reported in Pelger-Huët Homozygosity As Compared to Greenberg/HEM Dysplasia
937 LETTER TO JMG J Med Genet: first published as 10.1136/jmg.40.12.937 on 18 December 2003. Downloaded from Congenital abnormalities reported in Pelger-Hue¨t homozygosity as compared to Greenberg/HEM dysplasia: highly variable expression of allelic phenotypes J C Oosterwijk, S Mansour, G van Noort, H R Waterham, C M Hall, R C M Hennekam ............................................................................................................................... J Med Genet 2003;40:937–941 n 1928 the Dutch physician Pelger described two patients Key points with a morphological abnormality of leukocytes that Iconsisted of hypolobulation of the nuclei: there were two lobes instead of the usual five or more and the chromatin N Pelger-Hue¨t anomaly (PHA) is a benign, autosomal structure was coarse and denser.1 This was subsequently dominant haematological trait characterised by hypo- shown to be a genetic trait by paediatrician Hue¨t.2 In the lobulation of granulocyte nuclei. PHA homozygosity, following years many families with Pelger-Hue¨t anomaly however, is associated with skeletal abnormalities and (PHA) from different countries were reported and autosomal early lethality on the basis of animal studies and case dominant inheritance was firmly established.3 Bilobulated reports. In 2002 PHA was found to be due to PHA nuclei (‘‘spectacle’’ or ‘‘pince-nez’’ cells) can also be a heterozygous mutations in the lamin B receptor gene transient symptom in the presence of underlying disease (— (LBR), and a homozygous LBR mutation was detected in for example, infection, myeloid leukaemia or medication) as a boy with mild congenital abnormalities. Homozygous part of a ‘‘shift to the left’’ (pseudo PHA), but constitutional mutations in Lbr cause the ic/ic phenotype in mice. -

Blueprint Genetics Comprehensive Growth Disorders / Skeletal
Comprehensive Growth Disorders / Skeletal Dysplasias and Disorders Panel Test code: MA4301 Is a 374 gene panel that includes assessment of non-coding variants. This panel covers the majority of the genes listed in the Nosology 2015 (PMID: 26394607) and all genes in our Malformation category that cause growth retardation, short stature or skeletal dysplasia and is therefore a powerful diagnostic tool. It is ideal for patients suspected to have a syndromic or an isolated growth disorder or a skeletal dysplasia. About Comprehensive Growth Disorders / Skeletal Dysplasias and Disorders This panel covers a broad spectrum of diseases associated with growth retardation, short stature or skeletal dysplasia. Many of these conditions have overlapping features which can make clinical diagnosis a challenge. Genetic diagnostics is therefore the most efficient way to subtype the diseases and enable individualized treatment and management decisions. Moreover, detection of causative mutations establishes the mode of inheritance in the family which is essential for informed genetic counseling. For additional information regarding the conditions tested on this panel, please refer to the National Organization for Rare Disorders and / or GeneReviews. Availability 4 weeks Gene Set Description Genes in the Comprehensive Growth Disorders / Skeletal Dysplasias and Disorders Panel and their clinical significance Gene Associated phenotypes Inheritance ClinVar HGMD ACAN# Spondyloepimetaphyseal dysplasia, aggrecan type, AD/AR 20 56 Spondyloepiphyseal dysplasia, Kimberley -

Physical Assessment of the Newborn: Part 3
Physical Assessment of the Newborn: Part 3 ® Evaluate facial symmetry and features Glabella Nasal bridge Inner canthus Outer canthus Nasal alae (or Nare) Columella Philtrum Vermillion border of lip © K. Karlsen 2013 © K. Karlsen 2013 Forceps Marks Assess for symmetry when crying . Asymmetry cranial nerve injury Extent of injury . Eye involvement ophthalmology evaluation © David A. ClarkMD © David A. ClarkMD © K. Karlsen 2013 © K. Karlsen 2013 The S.T.A.B.L.E® Program © 2013. Handout may be reproduced for educational purposes. 1 Physical Assessment of the Newborn: Part 3 Bruising Moebius Syndrome Congenital facial paralysis 7th cranial nerve (facial) commonly Face presentation involved delivery . Affects facial expression, sense of taste, salivary and lacrimal gland innervation Other cranial nerves may also be © David A. ClarkMD involved © David A. ClarkMD . 5th (trigeminal – muscles of mastication) . 6th (eye movement) . 8th (balance, movement, hearing) © K. Karlsen 2013 © K. Karlsen 2013 Position, Size, Distance Outer canthal distance Position, Size, Distance Outer canthal distance Normal eye spacing Normal eye spacing inner canthal distance = inner canthal distance = palpebral fissure length Inner canthal distance palpebral fissure length Inner canthal distance Interpupillary distance (midpoints of pupils) distance of eyes from each other Interpupillary distance Palpebral fissure length (size of eye) Palpebral fissure length (size of eye) © K. Karlsen 2013 © K. Karlsen 2013 Position, Size, Distance Outer canthal distance -

Tests Performed Through Our International Collaboration
Tests performed through our international collaboration Molecular Studies for Inborn Errors of Metabolism A Inborn Errors of Metabolism Defective Gene 1 Acyl - Co A oxidase deficiency ACOX 1 2 Argininosuccinate lyase deficiency ASL 3 Aromatic L – amino acid decarboxylase (AADC) DDC Deficiency 4 Carnitine – acylcarnitine translocase (CACT) CACT Deficiency 5 Primary (systemic) carnitine deficiency OCTN2 6 Carnitine palmitoyltransferase I (CPT1) CPT1A 7 Carnitine palmitoyltransferase 2 (CPT2) CPT2 8 CHILD Syndrome NSDHL 9 Conradi – Hunermann – Happle syndrome EBP (CDPX2) 10 D – Bifunctional protein (DBP) Deficiency DBP, MFE2 11 Desmosterolosis DHCR24 12 Dihydropyrimidinase (DHP) Deficiency DPYS 13 Dihydropyrimidine dehydrogenase (DPD) DPYD Deficiency 14 Ethylmalonaciduria ETHE1 (Ethylmalonic encephalopathy) 15 Fructose intolerance, hereditary ALDOB 16 Galactosemia, classic GALT 17 Galactokinase deficiency GALK1 18 Glutaric aciduria type I (Glutaryl – Co A GCDH dehydrogenase deficiency 19 Glycogen storage disease 0 GYS2 20 Greenberg skeletal dysplasia LBR (Sterol – delta 14 reductase deficiency) 21 GTP cyclohydrolase I deficiency GCH1 22 Hydroxyacyl – Co A dehydrogenase deficiency HADH2 (2 – Methyl – 3 – hydroxybutyryl – CoA dehydrogenase deficiency) 23 Hyper Ig D Syndrome MVK (Mevalonate Kinase deficiency) 24 Hyperoxaluria type I AGXT 25 Isovaleric acidemia IVD 26 Lathosterolosis SC5DL 27 3 – methylglutaconicaciduria type I (3 – AUH methylglutaconyl – CoA hydratase deficiency) 28 Medium – chain – acyl – Co A dehydrogenase ACADM (MCAD) Deficiency -

Inherited Peroxisomal Disorders Involving the Nervous System
Arch Dis Child: first published as 10.1136/adc.63.7.767 on 1 July 1988. Downloaded from Archives of Disease in Childhood, i988, 63, 767-770 Annotations Inherited peroxisomal disorders involving the nervous system For genetic reasons peroxisomes may be absent or defective. Because of the great importance of the lack one or more of their enzymes. The result may peroxisomal enzymes involved in the I oxidation of be subtle and long delayed, but is often catastrophic VLCFA and the use of measurements of VLCFA in and immediately recognisable as a serious disorder diagnosis, this group is itself subdivided. Group 3A at birth. The trouble for the clinician is that it is includes those conditions in which VLCFA oxidation often not possible to make a diagnosis unless the is impaired and thus VLCFA accumulates, and right tests are thought of: these tests are not part of group 3B those in which the single enzyme defect is routine 'metabolic screens.' It is first necessary to of another sort. frame the question 'could this be a peroxisomopathy?' The object of this annotation is to help with when GENERALISED PEROXISOMAL DISORDERS (GROUP 1) and how to answer this question. The now classical example is the cerebro-hepato- renal syndrome of Zellweger. l 2The typical neonate Peroxisomes is more dysmorphic than a baby with Down's syndrome with high forehead and huge fontanelle Peroxisomes are subcellular organelles with a single with metopic extension. Inactivity is even greater membrane which occur in every cell apart from the than in the Prader-Willi syndrome and hypotonia mature erythrocyte. -

The Osteopetrotic Mutation Toothless (Tl) Is a Loss-Of-Function Frameshift Mutation in the Rat Csf1 Gene: Evidence of a Crucial
The osteopetrotic mutation toothless (tl)isa loss-of-function frameshift mutation in the rat Csf1 gene: Evidence of a crucial role for CSF-1 in osteoclastogenesis and endochondral ossification Liesbeth Van Wesenbeeck*, Paul R. Odgren†, Carole A. MacKay†, Marina D’Angelo‡§, Fayez F. Safadi‡, Steven N. Popoff‡, Wim Van Hul*, and Sandy C. Marks, Jr.†¶ *Department of Medical Genetics, University of Antwerp, Universiteitsplein 1, Antwerp B-2610, Belgium; †Department of Cell Biology, University of Massachusetts Medical School, 55 Lake Avenue, North Worcester, MA 01655; and ‡Department of Anatomy and Cell Biology, Temple University School of Medicine, 3400 North Broad Street, Philadelphia, PA 19140 Edited by Elizabeth D. Hay, Harvard Medical School, Boston, MA, and approved July 30, 2002 (received for review June 3, 2002) The toothless (tl) mutation in the rat is a naturally occurring, dritic cells, and formation of osteoclasts (refs. 9–12; reviewed in autosomal recessive mutation resulting in a profound deficiency of ref. 13). The transcription factor PU.1 functions in osteoclast bone-resorbing osteoclasts and peritoneal macrophages. The fail- differentiation and activation and in myeloid cells and B lym- ure to resorb bone produces severe, unrelenting osteopetrosis, phocytes (14); and NF-B, originally described as regulating with a highly sclerotic skeleton, lack of marrow spaces, failure of transcription of Ig light chain genes, is likewise necessary for tooth eruption, and other pathologies. Injections of CSF-1 improve osteoclastogenesis (15). some, but not all, of these. In this report we have used polymor- Phenotypes of osteopetrotic mutations vary widely, depending phism mapping, sequencing, and expression studies to identify the on where bone resorption is intercepted.