Ethiopia Emergency Type: Complex Reporting Period: 1-31 March 2019
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Districts of Ethiopia
Region District or Woredas Zone Remarks Afar Region Argobba Special Woreda -- Independent district/woredas Afar Region Afambo Zone 1 (Awsi Rasu) Afar Region Asayita Zone 1 (Awsi Rasu) Afar Region Chifra Zone 1 (Awsi Rasu) Afar Region Dubti Zone 1 (Awsi Rasu) Afar Region Elidar Zone 1 (Awsi Rasu) Afar Region Kori Zone 1 (Awsi Rasu) Afar Region Mille Zone 1 (Awsi Rasu) Afar Region Abala Zone 2 (Kilbet Rasu) Afar Region Afdera Zone 2 (Kilbet Rasu) Afar Region Berhale Zone 2 (Kilbet Rasu) Afar Region Dallol Zone 2 (Kilbet Rasu) Afar Region Erebti Zone 2 (Kilbet Rasu) Afar Region Koneba Zone 2 (Kilbet Rasu) Afar Region Megale Zone 2 (Kilbet Rasu) Afar Region Amibara Zone 3 (Gabi Rasu) Afar Region Awash Fentale Zone 3 (Gabi Rasu) Afar Region Bure Mudaytu Zone 3 (Gabi Rasu) Afar Region Dulecha Zone 3 (Gabi Rasu) Afar Region Gewane Zone 3 (Gabi Rasu) Afar Region Aura Zone 4 (Fantena Rasu) Afar Region Ewa Zone 4 (Fantena Rasu) Afar Region Gulina Zone 4 (Fantena Rasu) Afar Region Teru Zone 4 (Fantena Rasu) Afar Region Yalo Zone 4 (Fantena Rasu) Afar Region Dalifage (formerly known as Artuma) Zone 5 (Hari Rasu) Afar Region Dewe Zone 5 (Hari Rasu) Afar Region Hadele Ele (formerly known as Fursi) Zone 5 (Hari Rasu) Afar Region Simurobi Gele'alo Zone 5 (Hari Rasu) Afar Region Telalak Zone 5 (Hari Rasu) Amhara Region Achefer -- Defunct district/woredas Amhara Region Angolalla Terana Asagirt -- Defunct district/woredas Amhara Region Artuma Fursina Jile -- Defunct district/woredas Amhara Region Banja -- Defunct district/woredas Amhara Region Belessa -- -

Humanitarian Bulletin
Humanitarian Bulletin Ethiopia Issue #3| 17– 23 Feb. 2020 In this issue Recovery programming to returnees P.1 US$51.5 required for DL response P.2 Ethiopia’s ratification of the Kampala HIGHLIGHTS Convention P.2 • A US$20 million The personal story of Damma Abbalosa, recovery project an IDP in Hara Kela, Guji Zone P.3 (2019-2022) to benefit 50,000 Funding update P.4 households heavily impacted by the Gedeo-West Guji Displacement. • The project seeks to complement 50,000 returnee HHs in Gedeo and West Guji humanitarian assistance by zones to benefit from recovery programming supporting IDPs and local communities as A four-year recovery project (2019-2022) is underway in Gedeo zone SNNP region and per UNDP’s global West Guji zone, Oromia region with a total required budget of US$20 million. The project 3x6 approach that targets 50,000 households heavily impacted by the Gedeo-West Guji displacement in builds resilience in Kercha and Hamela Wamena woredas of West Guji Zone and Gedeb and Yirgachefe post-crisis situations woredas of Gedeo Zone. The project comes in complement of humanitarian assistance by for vulnerable groups supporting IDPs and local communities in the next phase towards recovery as per UNDP’s through introducing global 3x6 approach that builds resilience in post-crisis situations for vulnerable groups sustainable through introducing sustainable livelihoods. livelihoods. FIGURES People People in need targeted Food/Non- 8.4 M 7 M food SAM 544K 444K MAM 3.9 M 3.1 M IDPs 1.01M 1.01M Returnees 1.78 M 1.78 M HUMANITARIAN FUNDING US$1.001 billion Requirement for 2020 Ethiopia Humanitarian Response Plan Figure 1 IDPs sheltering at Harmufo site, Gedeb town at the height of the crisis in July 2018. -

ETHIOPIA Humanitarian Access Situation Report June – July 2019
ETHIOPIA Humanitarian Access Situation Report June – July 2019 This report is produced by OCHA Ethiopia in collaboration with humanitarian partners. It covers the period June - July 2019. The next report will be issued around September - October 2019. OVERVIEW IUS • In June - July, Ethiopia experienced an at- TIGRAY 276 Access incidents reported tempted government overthrow in Amhara, Western socio-political unrest in Sidama (SNNPR), North Gondar Wag Hamra Central Gondar and a rise in security incidents in Southwest- Zone 4 (Fantana Rasu) AFAR ern Oromia and Gambella. The quality of ac- Zone 1 (Awsi Rasu) cess declined, limiting assistance to people AMHARA No. o incidents by one South Wello Metekel in need, against a backdrop of massive gov- Oromia East Gojam BENISHANGUL Zone 5 (Hari Rasu) 4 13 35 49 AsosaGUMUZ Siti ernment-led returns of IDP to areas of origin. Zone 3 (Gabi Rasu) North Shewa(O) North Shewa(A) Kemashi Dire Dawa urban West Wellega East Wellega DIRE DAWA West Shewa Fafan • Hostilities between Ethiopian Defense Forc- ADDIS ABABA Kelem Wellega East Hararge Finfine Special West Hararge es (EDF) and Unidentified Armed Groups Buno Bedele East Shewa Etang Special Ilu Aba Bora Jarar OROMIA Erer (UAGs) as well as inter-ethnic, remained the GAMBELA Jimma Agnewak main access obstacle, with 197 incidents Doolo Nogob West Arsi SOMALI (out of 276), mostly in Southwestern Oromia SNNP Sidama Bale Korahe (110). The Wellegas, West Guji (Oromia), and Gedeo Shabelle Gambella, were the most insecure areas for Segen Area P. West Guji Guji aid workers. Liban Borena • In June, conflict in the Wellegas scaled up, Daawa with explosive devices attacks causing ci- Source: Access Incidents database vilian casualties in urban centres. -

Ethiopia: West Guji – Gedeo Conflict Displacement Flash Update 2
Ethiopia: West Guji – Gedeo Conflict Displacement Flash Update 2 22 May 2018 Highlights • A rapid assessment conducted in Gedeo zone (SNNPR) found that at least 274,5481 people were displaced from West Guji (Oromia) to Gedeo zone following the violence that erupted along the regional boundary in mid-April. Some 84,000 people were also displaced in West Guji zone. More than 4,000 houses were reportedly burnt down or damaged in West Guji and livelihoods destroyed. • Official reports indicate that as of early May, 102,593 people of the 274,548 people displaced in Gedeo were returned to their villages in West Guji zone • The Government, the local community and civil society were the first and main responders to date, with sup- port from few partners. Significant gaps in food, shelter, NFI and WaSH are reported • Although there were no reported health outbreaks so far, AWD, scabies and measles are potential health risks due to the use of water from unsafe sources, open defecation, overcrowded shelter and sharing of clothes. The overcrowded shelter conditions within hosting households also present protection concerns. Dara Sidama Dila I. Displacement overview ! 12,176 452 Bore Chichu A rapid assessment conducted in Gedeo zone ! 3,772 (SNNPR) from 2 to 8 May found that at least Dila Zuria stite eturns 274,548 people (139,494 male; 135,104 female) Wenago einin ! were displaced from West Guji (Oromia) to Gedeo Bule isceent 4,844 ! Koti ! zone, following the inter-communal violence that 8,198 Ilalcha ! erupted in mid-April 2018 along the borders of the Wenago Bule Abaya two zones. -

Socio-Economic Assessment
SOCIO-ECONOMIC ASSESSMENT SNNP IAIP and RTC Report Produced by: WSP in collaboration with Engineer Tequam Water Resources Development and Environment Consultancy (ETWRDEC) DATE: JANUARY 2018 Socio-Economic Assessment – SNNP IAIP & RTCDraft January 2018 Table of Contents 1 INTRODUCTION .................................................................... 1 1.1 social areas of influence (AoI) – social study area ............................................................................................................ 1 1.2 administrative and demographic environment ......................................................................................... 1 1.3 migration patterns .............................................................................3 1.4 land use, livelihood and vulnerability .......................................3 1.5 ethnicity, religion and language ................................................. 4 1.6 education .............................................................................................. 4 1.7 household income and expenditure ........................................ 4 1.8 existing infrastructure .................................................................... 5 1.9 national holidays ............................................................................... 5 2 SOCIO-ECONOMIC PROFILE OF PEOPLE IN THE PROJECT AREA (BASED ON WSP SURVEY) ............................................. 7 2.1 methodology ....................................................................................... -
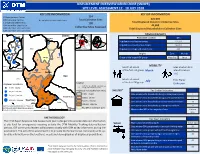
Displacement Overview Gedeo Zone (Snnpr)
DISPLACEMENT OVERVIEW GEDEO ZONE (SNNPR) SITE LEVEL ASSESSMENT 12 - 18 JULY 2018 KEY SITE INFORMATION KEY IDP INFORMATION 23 Spontaneous Camps 134 106 Collective Centres 4 Completely Inaccesible Sites Total Collective Sites 276,939 1 Dispersed Settlements 130 Total Displaced People In Collective Sites 19 Inaccesible Sites By Car 44,005 Collective Sites Assessed 123 Collective Sites with SMC Total Displaced Households In Collective Sites 127 Collective Sites with SMA Sidama Hadiya Arsi KTAlaba DEMOGRAPHICS Dila Town Sidama Hadiya ! Dila Town Wolayita West Arsi Population Location IDPs D!ila Zuria Sidama Abaya ÔÔ Bale Population in collective centres 217,971 Wenago Ô Gamo GofaGedio Bule Guji Population in spontaneous camps 58,518 ! Ô West Guji Abaya Yirgachefe Town Borena Liben Population in dispersed settlements 450 ! Dila Zuria ÔÔ Yirgachefe Ô Origins Zone Woreda Ô Ô ! Wenago Bule Ô Origin of the largest IDP group West Guji Kerca Ô Kochere ! Ô WGeestd eGbuji Ô Gelana MOBILITY Kercha Month of arrival Sites at which IDPs ÔÔ Yirgachefe Bule Hora Ô Ô Ô of the first IDP group March intend to return ÔÔ Yirgachefe Town Gedeo ÔÔ 116 Ô Ô Guji Ô Ô Gelana ÔÔ Ô Ô Month of arrival Time Frame Ô July ÔÔ Legend of the last IDP group Unknown Displaced individuals Ô Ô ÔKochere ÔÔ Collective sites (includes spontaneous ÔÔÔ Ô ÔÔ Ô ! 7,705 - 10,000 ÔÔÔ ÔÔ camps and collective centers) ÔÔ Ô Ô Displaced individuals (from Sites) SHELTER* Key Shelter Indicators ! 10,001 - 50,000 Ô Ô 7,705 - 10,000 Sites where >50% households living outside/open spaces 7 50,001 - 100,000 Ô Ô ! ÔÔÔÔ Ô ÔÔ ÔÔ ÔÔÔ Hambela Wamena ÔÔÔÔ Ô ÔÔÔ 10,001 - 50,000 Sites where >50% households living in permanent shelter 67 ! 100,001 - 129,629 West Guji Gedeb 50,001 - 100,000 Ô Kercha Sites where >50% households in below standard shelters 18 Ô This map is for illustration purposes only. -

World Bank Document
Sample Procurement Plan (Text in italic font is meant for instruction to staff and should be deleted in the final version of the PP) Public Disclosure Authorized (This is only a sample with the minimum content that is required to be included in the PAD. The detailed procurement plan is still mandatory for disclosure on the Bank’s website in accordance with the guidelines. The initial procurement plan will cover the first 18 months of the project and then updated annually or earlier as necessary). I. General 1. Bank’s approval Date of the procurement Plan: Updated Procurement Plan, M 2. Date of General Procurement Notice: Dec 24, 2006 Public Disclosure Authorized 3. Period covered by this procurement plan: The procurement period of project covered from year June 2010 to December 2012 II. Goods and Works and non-consulting services. 1. Prior Review Threshold: Procurement Decisions subject to Prior Review by the Bank as stated in Appendix 1 to the Guidelines for Procurement: [Thresholds for applicable procurement methods (not limited to the list below) will be determined by the Procurement Specialist /Procurement Accredited Staff based on the assessment of the implementing agency’s capacity.] Public Disclosure Authorized Procurement Method Prior Review Comments Threshold US$ 1. ICB and LIB (Goods) Above US$ 500,000 All 2. NCB (Goods) Above US$ 100,000 First contract 3. ICB (Works) Above US$ 15 million All 4. NCB (Works) Above US$ 5 million All 5. (Non-Consultant Services) Below US$ 100,000 First contract [Add other methods if necessary] 2. Prequalification. Bidders for _Not applicable_ shall be prequalified in accordance with the provisions of paragraphs 2.9 and 2.10 of the Public Disclosure Authorized Guidelines. -

Oromia Region Administrative Map(As of 27 March 2013)
ETHIOPIA: Oromia Region Administrative Map (as of 27 March 2013) Amhara Gundo Meskel ! Amuru Dera Kelo ! Agemsa BENISHANGUL ! Jangir Ibantu ! ! Filikilik Hidabu GUMUZ Kiremu ! ! Wara AMHARA Haro ! Obera Jarte Gosha Dire ! ! Abote ! Tsiyon Jars!o ! Ejere Limu Ayana ! Kiremu Alibo ! Jardega Hose Tulu Miki Haro ! ! Kokofe Ababo Mana Mendi ! Gebre ! Gida ! Guracha ! ! Degem AFAR ! Gelila SomHbo oro Abay ! ! Sibu Kiltu Kewo Kere ! Biriti Degem DIRE DAWA Ayana ! ! Fiche Benguwa Chomen Dobi Abuna Ali ! K! ara ! Kuyu Debre Tsige ! Toba Guduru Dedu ! Doro ! ! Achane G/Be!ret Minare Debre ! Mendida Shambu Daleti ! Libanos Weberi Abe Chulute! Jemo ! Abichuna Kombolcha West Limu Hor!o ! Meta Yaya Gota Dongoro Kombolcha Ginde Kachisi Lefo ! Muke Turi Melka Chinaksen ! Gne'a ! N!ejo Fincha!-a Kembolcha R!obi ! Adda Gulele Rafu Jarso ! ! ! Wuchale ! Nopa ! Beret Mekoda Muger ! ! Wellega Nejo ! Goro Kulubi ! ! Funyan Debeka Boji Shikute Berga Jida ! Kombolcha Kober Guto Guduru ! !Duber Water Kersa Haro Jarso ! ! Debra ! ! Bira Gudetu ! Bila Seyo Chobi Kembibit Gutu Che!lenko ! ! Welenkombi Gorfo ! ! Begi Jarso Dirmeji Gida Bila Jimma ! Ketket Mulo ! Kersa Maya Bila Gola ! ! ! Sheno ! Kobo Alem Kondole ! ! Bicho ! Deder Gursum Muklemi Hena Sibu ! Chancho Wenoda ! Mieso Doba Kurfa Maya Beg!i Deboko ! Rare Mida ! Goja Shino Inchini Sululta Aleltu Babile Jimma Mulo ! Meta Guliso Golo Sire Hunde! Deder Chele ! Tobi Lalo ! Mekenejo Bitile ! Kegn Aleltu ! Tulo ! Harawacha ! ! ! ! Rob G! obu Genete ! Ifata Jeldu Lafto Girawa ! Gawo Inango ! Sendafa Mieso Hirna -

Damage and Loss Assessment EXECUTIVE SUMMARY ©UNHCR/Adelina Gomez
©UNHCR/Anna Helge Damage and Loss Assessment EXECUTIVE SUMMARY ©UNHCR/Adelina Gomez TABLE OF CONTENT EXECUTIVE SUMMARY 3 DAMAGE AND LOSS IN AGRICULTURAL PRODUCTION SECTORS 4 DAMAGE ON LIVESTOCK PRODUCTION SYSTEM 5 DAMAGE AND LOSS ASSESMENT ON SOCIAL AND INFRAESTRUCTURAL 6 SECTORS • Private houses 6 • Public Infrastructure 7 • Recommendations 8 LEGAL ASSISTANCE NEEDS 10 • Access to justice 10 • Access to Land holding certificate 11 • Customary/Traditional justice system 12 • Recommendations 12 CONFLICT, PEACE BUILDING AND SOCIAL COHESION 13 POSSIBLE APPROACHES FOR CONFLICT TRANSFORMATION AND PEACE- 14 BUILDING IN THE CONTEXT OF GUJI AND GEDEO ETHNIC GROUPS • Building Trust 14 • Developing social cohesion 15 • Supporting local buy-in 15 • Recommendations 16 APPENDIX 1 18 - 2 - EXECUTIVE SUMMARY Damage and Loss Assessment in West Guji Bule Hora University initiated a Damage and Loss Assessment (DaLA) in West Guji zone in collaboration with the United Nations High Commissioner for Refugees (UNHCR) and the West Guji Zonal Disaster Risk Management Office to assess loss and damages incurred during the intercommunal conflict between the Gedeo and Guji people in 2018, which displaced hundreds of thousands. The assessment also analyzed legal assistance needs, as well as the potential for peace-building and social cohesion. A total of 78,257HHs (508,671 individuals) with an average family size of 6.5/HH were severely exposed to multiple socio-economic crises due to the conflict. Following the Government’s initiated return process based on the alleged improved safety and security situation (assessed by the Government) in May 2019, according to the Government, the majority of the IDPs were returned to their places of habitual residence 1. -

Ethiopia: Gedeo and West Guji Zones - Reference Map (July 2018)
Ethiopia: Gedeo and West Guji Zones - Reference map (July 2018) Dila Dilla Town Andida Arura Abaya Mochise Sisota Chichu Chebicha Gwangwa Halo Dila Zuria Tomata Chercha Guanguwa Wenago SokichaUolabo Hasi Bule Adis Kofe Wenago Ilacha Sokicha Dedero Ghelissa Resa Bekere Holjo Chitu Lekicha Halemo Bule Repe Dumerso Bukisa Chichela Tulise Dido Shara Adame Yirgachefe Gerse Yirga Chefe Foge Wachile Gerse Haru Melka LoteKusae Haru Adido Konga Widese Kedida Mora Kele Ononcho Resiti Fiseha Genet Arru Adis Ketema Biloya - 793,094 Giwe Gelana Kochere Abel Ciorso Sisota Chelelektu Sigiga Dimtu Dibandibe Barti Wachu Jareme Tore Hambela Wamena Gedeb Gedeb Baya Edera Gadabi Jeba Sire Bilida Bukisa Edera Haro Kara Gerba Town Kercha Era Inshi Ela Ferda Birbirsa Kojowa Danise Ela Dima Mati Ebela Gaesa Dibisa Bule Hora Bule Hora Suro Surro Berguda Ropi Giari Bule Melkasoda Melka Soda Baya Gundi Welena Bokosa Finchawa Dugda Dawa Chichilla Cheme Town Paved road Zonal Capital Gravel road Wereda Capital Dry Weather road Other town/village Other road Region boundary Zones Zone boundary Gedio Woreda boundary West Guji Road 10km The boundaries and names shown and the designations used on this map do not imply official endorsement or acceptance by the United Nations. Creation date: 9 July 2018 Map Name: 21_ADM__Gedeo_WestGuji_070918_A0 Sources: CSA Feedback: [email protected] www.humanitarianresponse.info/operations/ethiopia www.reliefweb.int. -

Ethiopia Humanitarian Situation Report
UNICEF ETHIOPIA HUMANITARIAN SITUATION REPORT ETHIOPIA Humanitarian Situation Report SitRep # 5 - Reporting Period May 2019 SITUATION IN NUMBERS Highlights 4.89 million # of children in need of humanitarian Failed spring rains this year in parts of Afar, Amhara, Oromia and Somali regions have renewed concerns about another drought affecting children, assistance (Ethiopia Humanitarian Needs Overview 2019) further compounding vulnerabilities in regions already suffering from chronic food insecurity, prolonged and complex population displacements, and increased risks to outbreaks of cholera and measles. These regions 8.86 million also have over-stretched health care systems, poor access to water, and # of people in need recurrent outbreaks of preventable diseases. (Ethiopia Humanitarian Needs Overview 2019) As of April 2019, UNICEF has supported the screening and admission of 110,826 children under the age of five for severe acute malnutrition (SAM) 3.19 million treatment and the numbers are expected to grow with the projected Internally displaced persons in Ethiopia drought in the country. (Ethiopia Humanitarian Needs Overview 2019) UNICEF Ethiopia urgently requires US$ 5.4 million to replenish its nutrition commodities pipeline for the expected surge in severe acute malnutrition 919,938 (SAM) in 2019. In addition, US$ 2.45 million is required to rehabilitate 35 Registered refugees and asylum seekers in water schemes and provide durable safe water and sanitation for the most Ethiopia vulnerable children, including displaced children, -

The Quest for Resolution of Guji-Gedeo Conflicts in Southern Ethiopia: a Review of Mechanisms Employed, Actors and Their Effectiveness
The Quest for Resolution of Guji-Gedeo Conflicts in Southern Ethiopia: A Review of Mechanisms Employed, Actors and Their Effectiveness Girum Kinfemichael1 Abstract This article assesses the quest for resolution of Guji-Gedeo conflicts, the federal device as a means of managing conflict employed and their effectiveness. Methodologically, the study is mainly based on qualitative approach with an opinion and descriptive surveys to reveal the existing problems. It emerges from the study that the different structures, processes and mechanisms, which are employed at various levels of administrative hierarchies of governments for managing the conflicts, remain ad-hoc, not well-coordinated and, above all, their actions are mainly reactive. The study draws an argumentative conclusion that the Federal Government and authorities of the Southern Nations, Nationalities and Peoples’ Region (SNNPR) and Oromiya Regional State need to boost their close cooperation, engagement in early warning and conflict management endeavors in addressing the conflict as the two communities are still at loggerheads over the issue of defining the contested boundary claims. It is also useful to extend the scope of such cooperation and engagement to the level of local governments in both Regional States. Along with these efforts, it would be better if authorities at various levels revitalize and empower traditional conflict resolution institutions to run parallel with ‘modern’ government structures to respond to the conflicts promptly. It is thus prudent to use the advantage of federalism as flexible and innovative system of governance to manage the conflict constructively. Keywords: Boundary conflicts, ethnicity, ethnic federation, federal restructuring, Guji-Gedeo conflicts, indigenous institutions. 1 Lecturer, Department of Federalism and Local Government Studies, Institute of Federalism and Legal Studies, Ethiopian Civil Service University.