2-Cultural Context and Impact of Alcohol Use.Pdf (62Kb)
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Signatory ID Name CIN Company Name 02700003 RAM TIKA
Signatory ID Name CIN Company Name 02700003 RAM TIKA U55101DL1998PTC094457 RVS HOTELS AND RESORTS 02700032 BANSAL SHYAM SUNDER U70102AP2005PTC047718 SHREEMUKH PROPERTIES PRIVATE 02700065 CHHIBA SAVITA U01100MH2004PTC150274 DEJA VU FARMS PRIVATE LIMITED 02700070 PARATE VIJAYKUMAR U45200MH1993PTC072352 PARATE DEVELOPERS P LTD 02700076 BHARATI GHOSH U85110WB2007PTC118976 ACCURATE MEDICARE & 02700087 JAIN MANISH RAJMAL U45202MH1950PTC008342 LEO ESTATES PRIVATE LIMITED 02700109 NATESAN RAMACHANDRAN U51505TN2002PTC049271 RESHMA ELECTRIC PRIVATE 02700110 JEGADEESAN MAHENDRAN U51505TN2002PTC049271 RESHMA ELECTRIC PRIVATE 02700126 GUPTA JAGDISH PRASAD U74210MP2003PTC015880 GOPAL SEVA PRIVATE LIMITED 02700155 KRISHNAKUMARAN NAIR U45201GJ1994PTC021976 SHARVIL HOUSING PVT LTD 02700157 DHIREN OZA VASANTLAL U45201GJ1994PTC021976 SHARVIL HOUSING PVT LTD 02700183 GUPTA KEDAR NATH U72200AP2004PTC044434 TRAVASH SOFTWARE SOLUTIONS 02700187 KUMARASWAMY KUNIGAL U93090KA2006PLC039899 EMERALD AIRLINES LIMITED 02700216 JAIN MANOJ U15400MP2007PTC020151 CHAMBAL VALLEY AGRO 02700222 BHAIYA SHARAD U45402TN1996PTC036292 NORTHERN TANCHEM PRIVATE 02700226 HENDIN URI ZIPORI U55101HP2008PTC030910 INNER WELLSPRING HOSPITALITY 02700266 KUMARI POLURU VIJAYA U60221PY2001PLC001594 REGENCY TRANSPORT CARRIERS 02700285 DEVADASON NALLATHAMPI U72200TN2006PTC059044 ZENTERE SOLUTIONS PRIVATE 02700322 GOPAL KAKA RAM U01400UP2007PTC033194 KESHRI AGRI GENETICS PRIVATE 02700342 ASHISH OBERAI U74120DL2008PTC184837 ASTHA LAND SCAPE PRIVATE 02700354 MADHUSUDHANA REDDY U70200KA2005PTC036400 -

Physiology and Biochemistry of Indigenous Tribal Liquor Haria: a State of Art
Mini Review Adv Biotech & Micro Volume 6 Issue 2 - september 2017 Copyright © All rights are reserved by Rintu Banerjee DOI: 10.19080/AIBM.2017.06.555683 Physiology and Biochemistry of Indigenous Tribal Liquor Haria: A State of Art Mohan Das, Debajyoti Kundu, Jagriti Singh, Akanksha Rastogi and Rintu Banerjee* Agricultural and Food Engineering Department, Indian Institute of Technology Kharagpur, India Submission: August 21, 2017; Published: September 20, 2017 *Corresponding author: Rintu Banerjee, Agricultural and Food Engineering Department, Indian Institute of Technology, Kharagpur-721302, India, Tel: + (O)/+ (R); Fax: + ; Email: Abstract Haria, also known as rice beer is an ethnic alcoholic drink that has gained huge approbation among the tribal’s of Bengal. The liquor is mostly prepared using the indigenous knowledge of the tribal community. The uniqueness of the liquor lies in the application of Bakhar, an amylolytic starter culture. Although, the preparation of Bakhar differs from community to community but ~42 species of ethno-botanically important plants are mostly used. The microbial consortia are naturally outsourced from rice and herbs used for the preparation of Bakhar. The amylolytic starter culture consistently generates maltooligosaccharides, which is a low calorie ingredient, less sweet and viscous, capable of retaining ample quantity of water within it. Besides, serving the purpose of a beverage, Haria can compensate the loss of water in the human system under extreme high temperature. Together with this, the drink also serves as a remedy for several acute and chronic diseases which may be due to the use of certain medicinal herbs as starter culture. Keywords: Fermentation; Beverage; Tribe; Haria; Bakhar Introduction Preservation of foods through natural fermentation is a purpose of beverage, brewed liquors sometimes acts as a widely accepted methodology, practised from the ancient times. -
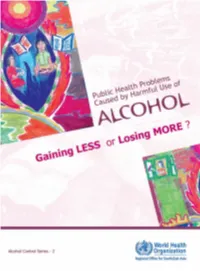
Public Health Problems Caused by Harmful Use of Alcohol — Gaining Less Or Losing More? (Alcohol Control Series No
“ALCOHOL CONTROL” SERIES, No. 2 Other titles in the “Alcohol Control” series are: No.1. Burden and Socio-Economic Impact of Alcohol — The Bangalore Study No.3. Alcohol Control Policies in the South-East Asia Region — Selected Issues No.4. Alcohol Use and Abuse — What You Should Know No.5. Reducing Harm from Use of Alcohol — Community Responses Cover adapted from painting by: Sahil Bakshi, Class-X, Lovely Public Senior School, New Delhi, India Contributors National Institute of Mental Health and Neurosciences, Bangalore, India Dr Gururaj G, Professor and Head of Epidemiology Dr Girish N, Assistant Professor of Epidemiology Dr Vivek Benegal, Associate Professor of Psychiatry Department of Non-communicable Diseases and Mental Health World Health Organization, Regional Office for South-East Asia, New Delhi, India Dr Vijay Chandra, Regional Adviser, Mental Health and Substance Abuse Unit Dr Rajesh Pandav, Short-term Professional, Mental Health and Substance Abuse Unit Public Health Problems Caused by Harmful Use of Gaining LESS or Losing MORE ? Acknowledgement The authors would like to thank Dr Thaksaphon Thamarangsi for his input into the section on “international evidence for intervention”. WHO Library Cataloguing-in-Publication Data World Health Organization, Regional Office for South-East Asia Public Health Problems Caused by Harmful Use of Alcohol — Gaining Less or Losing More? (Alcohol Control Series No. 2) Keywords 1. Alcoholism – Prevention and Control 2. Alcohol-related Disorders 3. Alcohol Drinking – Adverse Effects 4. Public Health – Statistics and Numerical Data 5. South-East Asia ISBN 92 9022 273 5 (NLM classification: WM 270) © World Health Organization 2006 Publications of the World Health Organization enjoy copyright protection in accordance with the provisions of Protocol 2 of the Universal Copyright Convention. -

ALCOHOLIC BEVERAGES in INDIA Dacca Division, Populated Mostly by Muslims by Sir R
Special Articles ALCOHOLIC BEVERAGES IN INDIA Dacca division, populated mostly by Muslims By Sir R. N. CHOPRA, c.i.e., m.a., m.d., sc.d., (67 per cent). This area is mainly agricultural, and of alcohol on f.r.c.p. (Lond.) therefore the consumption is, the much lower here than in the other colonel, i.m.s. (Retd.) whole, parts of the province. G. S. CHOPRA, m.b., b.s. Pachwai or handia or mama, i.e., fermented liquor and brewed from rice or millet, is drunk chiefly by the both I. C. CHOPRA, m.r.c.s. (Eng.), l.r.c.p. (Lond.), aboriginal tribes in several districts and is used as a stimulant and as a food. It is the favourite drink d.t.m. (Cal.) of the lower classes, particularly the aboriginals. {From the School of Tropical Medicine, Calcutta) Except in Darjeeling, where pachwai is chiefly made from millet, rice is mainly used for its production. Part II Free home-brewing of pachwai is permitted only f?r private to the tribes in a few in consumption aboriginal Consumption of country spirits and beers districts during the annual Bandhana and Pons different provinces Sankranti festivals. Wanchu, a variety of fermented liquor, prepared from is sometimes used by the In this section an is made to review rice, attempt Chinese in Calcutta on ceremonial occasions for which the present position of the use of different temporary permission is obtainable. alcoholic beverages in different provinces with special reference to the conditions which deter- Table VI mine their in these areas. -

Bangla Menu 2014 for Lal.Pdf
A warm welcome to: MoFo 2010 The Federation of British Curry Awards Specialist Restaurants. 2008 & 2010 Bangla Fusion known for its opulent style and unrivalled fine dining is inviting you to come and experience the most elegant and paramount dishes that will exceed your satisfaction. The divine combination of East and West promises a delectable meal whilst marrying the sublime ambience with comfortable sofas and rich artefacts; Bangla Fusion guarantees a night that you will never forget. Whether you fancy a drink from our vast wine bar, a classic curry or perhaps you have an acquired taste for something special, we have the menu to fulfil your choice.We are sure we can offer something that will satisfy your palate. Our welcoming staff will take care of your every need, starting with a drink of your choosing from the ample wine bar. You might want to order from our variety of wines, where we have a wide selection of red, white and rose to perfectly accompany your meal. Or naturally you can choose from our draft lagers, bottles, spirits or soft drinks. We use the highest quality ingredients because our aim is to provide our guests with a memorable wine & dining experience, and the food itself is integral to this. Whatever you choose our talented chefs will prepare your food with care and craft, taking every step to ensure your meal is the best it can be. It’s this approach that has earned Bangla Fusion some prestigious accolades. We’re also proud to be voted in the Top 100 restaurants in the UK with British Curry Awards from 2008 and are delighted to be nominated and shortlisted for the British Curry Awards this year. -
Excise the World of Intoxication
REVENUE EARNING DEPARTMENTS - EXCISE THE WORLD OF INTOXICATION Alcoholic Drinks: Previous Era Alcoholic Drinks: History Alcoholic drinks made from fermented food stuffs have been in used from ancient times. Fermented drinks antedate distilled spirits, though the process of distillation was known to the ancient Assyrians, Chinese, Greeks and Hindus. The manufacture, sale and consumption of intoxicating liquor have been subject to state control from very early times in India. Alcoholic Drinks - in India Drinks were known in India in Vedik and Post Vedik times. The celestial drink of Vedik period is known as Soma. • Sura is fermented beverage during Athavana Veda period. Alcoholic Drinks – Making in different periods • Pulasty’s • Kautilya’s Alcohol making : Pulasty’s Period • Panasa( Liquor from Jack fruit) • Madhvika (Mohowa Liquor) • Draksha (Liquor from Grape) • Saira (Long pepper Liquor) • Madhuka (Honey Liquor) • Arishta (Soap Berry Liquor) • Khajura (Date Liquor) • Maireya (Rum) • Tala (Palm Liquor) • Narikelaja (Coconut Liquor) • Sikhshava (Cane Liquor) • Sura / Arrack. Alcohol making : Kautilya’s Period • Medaka • Prasanna • Asava • Arisha • Maireya • Madhu Indian Alcoholic Beverages Indian Alcoholic Beverages : Types • Traditional Alcoholic Beverages • Non- Traditional Alcoholic Beverages Traditional Alcoholic Beverages • Feni • Hudamaba • Palm Wine • Handia • Hariya • Kaidum • Desidaru • Sonti • Kodo Kojaanr • Apo / Apung • Sulai • Laopani • Arrack • Sundakanji • Luqdi • Bangla • Sura • Mahua • Bitchi • Tati Kallu • Mahuli • Chhaang • Tharra • Mandia Pej • Cholai • Zawlaidi • Manri • Chuak • Zutho • Pendha • Sekmai Non - Traditional Alcoholic Beverages • Indian Beer • Indian Brandy • Indian made Foreign Liquor • Indian Rum • Indian Vodka • Indian Wine Alcoholic Beverages Alcohol Beverages : as a source of Revenue Alcoholic beverages received to distinctions with the advent of the British Rule in India. -

Alcoholic Beverages in Bangladesh-How Much We Know? Md
Medical S & c e ie in n c c i e d R e e M s Family Medicine & e y l a i r c m h Rasker JJ et al., Fam Med Med Sci Res 2014, 3:2 a F ISSN: 2327-4972 Medical Science Research DOI: 10.4172/2327-4972.1000123 Research Article Open Access Alcoholic Beverages in Bangladesh-How Much We Know? Md. Islam N1,2, Ferdous N2, Nesha K2, Rasker JJ3* 1Department of Rheumatology, Bangabandhu Sheikh Mujib Medical University, Dhaka, Bangladesh 2Modern One stop Arthritis Care and Research Center® (MOAC&RC®), Dhanmondi, Road 8, House 17, Dhaka, Bangladesh 3Faculty of Behavoural Sciences, Department of Psychology, Health & Technology, University of Twente, Enschede, The Netherlands *Corresponding author: Johannes J Rasker, Faculty of Behavoural Sciences, Department of Psychology, Health & Technology, University of Twente, Enschede, The Netherlands; Tel: 31623628967; E-mail: [email protected] Rec date: Mar 16, 2014, Acc date: June 02, 2014, Pub date: June 04, 2014 Copyright: © 2014 Md. Islam N, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Abstract Objectives: This study was aimed to determine the names and alcohol content or strength of different alcoholic beverages used in different parts of Bangladesh and also to determine contamination with heavy metals and bacteria in some samples. Methods: Eight different types of alcoholic beverages consumed in different parts of Bangladesh were collected and studied in the laboratory of Bangladesh Council of Scientific and Industrial Research (BCSIR). -

Types of Alcohol and Alcoholic Beverages
Y K here are different types of alcohol. Some are used in chemistry laboratories and industry, e.g. isopropyl and methyl alcohol. Isopropanol, or Tisopropyl alcohol is also used in industrial processes as well as in home cleaning products and skin lotions. It is TYPES OF ALCOHOL also commonly known as "rubbing alcohol". Methanol, AND ALCOHOLIC or methyl alcohol or wood alcohol has been used as an industrial solvent and is also commonly available as BEVERAGES methylated spirit. It is found in cleaning solvents, paint removers, photocopier developer and anti-freeze solutions. As such, it is often available in large quantities inexpensively. It is similar to ethanol but the end product after it is digested by the body is formaldehyde, which is poisonous. This is responsible for "alcohol poisoning". Methanol poisoning leading to blindness has been known to occur on consuming even small amounts. Another type of alcohol is ethyl alcohol, also known as ethanol. This has been consumed by human beings for its intoxicating and mind-altering effects. The term 'alcohol', unless specified otherwise, refers to ethanol or ethyl alcohol. It is a thin, clear liquid with harsh burning taste and high volatility. It is usually consumed in diluted concentrations M C M K of absolute (i.e. 100 per cent) ethyl alcohol. Ethyl alcohol is Y K also used as a reagent in some industrial applications. For such use, ethyl alcohol is combined with small quantities of methanol, with the mixture being called "denatured ethanol" to prevent theft for human consumption. Brief description of alcoholic beverages Wines are made from a variety of fruits, such as grapes, peaches, plums or apricots. -

Download (1073KB)
National Journal of Multidisciplinary Research and Development National Journal of Multidisciplinary Research and Development ISSN: 2455-9040 Impact Factor: RJIF 5.22 www.nationaljournals.com Volume 3; Issue 1; January 2018; Page No. 106-122 Alcohol and its induced aura that imposed adverse effects on socio-economic, neurobehavioural and biological health in Indians 1 Rajesh Kumar Kori, *2 Dr. Deepak Gupta 1 Research Fellow, M.Sc. (Forensic Science), Department of Criminology & Forensic Science, School of Applied Sciences, Dr. Harisingh Gour Central University, Madhya Pradesh, India 2 Assistant Professor, Ph.D. (Criminology), Department of Criminology & Forensic Science, School of Applied Sciences, Dr. Harisingh Gour Central University, Madhya Pradesh, India Abstract A chronic alcohol consumption (CAA) is a global problem for economic and health of an addicted person. The adverse effects of chronic and acute alcoholism have been started with short-term pleasant experience like a hangover, insanities extend with long- term addiction habits that lead to critical adverse health outcomes like cancer, a developmental disorder, neurobehavioural disorder (Depression, Anxiety, Impulsiveness, Aggression). Consequently, person entrapped with disorder riddle with imprudence, depressed, anxious, impaired decision slipped into the valley of detainment, loneliness state that trigger to think the permanent solution to pain or problem mostly that ends in different ways one might be initiated with suicidal ideation, suicidal attempts or suicide (inward -
Wine and Liquor Bottles to Carry Warnings from April 2019
Wine and Liquor Bottles to carry Warnings from April 2019 Aug 27: India’s apex food safety regulator, Food Safety and Standards Authority of India.(FSSAI) has given a directive that from April 2019, all wine, liquor bottles in every State will be required to affix a label saying “Be Safe-Don’t Drink and Drive” on the directives of High Court FSSAI has made it mandatory for all liquor bottles to have a message against drunken driving on their labels from April next year. A notification in this regard was published by the Ministry of Health and Family Welfare through FSSAI. The warning will read, “Be Safe-Don’t Drink and Drive”. Every liquor, wine or beer bottle, whether of country made liquor, Indian- Made Foreign Liquor, or imported alcohol, will carry the textual warnings in English, Hindi or a regional language. The Authority, however, decided not to enforce the suggestion to add a pictorial warning on the lines of that on cigarette packets, currently in force. The development follows an Order passed by the Delhi High Court, which had asked the FSSAI to look into the matter, on a petition filed by the NGO Community ‘Against Drunken Driving’ (CADD). “Countries across the world that have adopted such warnings include USA, Kenya, South Africa, Thailand, Zimbabwe, Taiwan, Mexico, and Turkey,” says Prince Singhal of CADD which filed the petition. He claims that these countries have been able to bring down the tragedies resulting from drunken driving. According to official data, the fatality rate in road crashes involving drink-driving is high. -

Alcoholic Beverages in Bangladesh-How Much We Know? Md
Family Medicine & Medical Rasker JJ et al., Fam Med Med Sci Res 2014, 3:2 Science Research http://dx.doi.org/10.4172/2327-4972.1000123 Research Article Open Access Alcoholic Beverages in Bangladesh-How Much We Know? Md. Islam N1,2, Ferdous N2, Nesha K2, Rasker JJ3* 1Department of Rheumatology, Bangabandhu Sheikh Mujib Medical University, Dhaka, Bangladesh 2Modern One stop Arthritis Care and Research Center® (MOAC&RC®), Dhanmondi, Road 8, House 17, Dhaka, Bangladesh 3Faculty of Behavoural Sciences, Department of Psychology, Health & Technology, University of Twente, Enschede, The Netherlands *Corresponding author: Johannes J Rasker, Faculty of Behavoural Sciences, Department of Psychology, Health & Technology, University of Twente, Enschede, The Netherlands; Tel: 31623628967; E-mail: [email protected] Rec date: Mar 16, 2014, Acc date: June 02, 2014, Pub date: June 04, 2014 Copyright: © 2014 Md. Islam N, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Abstract Objectives: This study was aimed to determine the names and alcohol content or strength of different alcoholic beverages used in different parts of Bangladesh and also to determine contamination with heavy metals and bacteria in some samples. Methods: Eight different types of alcoholic beverages consumed in different parts of Bangladesh were collected and studied in the laboratory of Bangladesh Council of Scientific and Industrial Research (BCSIR). Before sending to the laboratory, samples were stored in a refrigerator at temperature 4-8 degree Celsius. In all samples, strength of ethanol content was studied. -

List of Common Service Centres Established in Uttar Pradesh
LIST OF COMMON SERVICE CENTRES ESTABLISHED IN UTTAR PRADESH S.No. VLE Name Contact Number Village Block District SCA 1 Aram singh 9458468112 Fathehabad Fathehabad Agra Vayam Tech. 2 Shiv Shankar Sharma 9528570704 Pentikhera Fathehabad Agra Vayam Tech. 3 Rajesh Singh 9058541589 Bhikanpur (Sarangpur) Fatehabad Agra Vayam Tech. 4 Ravindra Kumar Sharma 9758227711 Jarari (Rasoolpur) Fatehabad Agra Vayam Tech. 5 Satendra 9759965038 Bijoli Bah Agra Vayam Tech. 6 Mahesh Kumar 9412414296 Bara Khurd Akrabad Aligarh Vayam Tech. 7 Mohit Kumar Sharma 9410692572 Pali Mukimpur Bijoli Aligarh Vayam Tech. 8 Rakesh Kumur 9917177296 Pilkhunu Bijoli Aligarh Vayam Tech. 9 Vijay Pal Singh 9410256553 Quarsi Lodha Aligarh Vayam Tech. 10 Prasann Kumar 9759979754 Jirauli Dhoomsingh Atruli Aligarh Vayam Tech. 11 Rajkumar 9758978036 Kaliyanpur Rani Atruli Aligarh Vayam Tech. 12 Ravisankar 8006529997 Nagar Atruli Aligarh Vayam Tech. 13 Ajitendra Vijay 9917273495 Mahamudpur Jamalpur Dhanipur Aligarh Vayam Tech. 14 Divya Sharma 7830346821 Bankner Khair Aligarh Vayam Tech. 15 Ajay Pal Singh 9012148987 Kandli Iglas Aligarh Vayam Tech. 16 Puneet Agrawal 8410104219 Chota Jawan Jawan Aligarh Vayam Tech. 17 Upendra Singh 9568154697 Nagla Lochan Bijoli Aligarh Vayam Tech. 18 VIKAS 9719632620 CHAK VEERUMPUR JEWAR G.B.Nagar Vayam Tech. 19 MUSARRAT ALI 9015072930 JARCHA DADRI G.B.Nagar Vayam Tech. 20 SATYA BHAN SINGH 9818498799 KHATANA DADRI G.B.Nagar Vayam Tech. 21 SATYVIR SINGH 8979997811 NAGLA NAINSUKH DADRI G.B.Nagar Vayam Tech. 22 VIKRAM SINGH 9015758386 AKILPUR JAGER DADRI G.B.Nagar Vayam Tech. 23 Pushpendra Kumar 9412845804 Mohmadpur Jadon Dankaur G.B.Nagar Vayam Tech. 24 Sandeep Tyagi 9810206799 Chhaprola Bisrakh G.B.Nagar Vayam Tech.