District Health Action Plan Kargil
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Distribution of Bufotes Latastii (Boulenger, 1882), Endemic to the Western Himalaya
Alytes, 2018, 36 (1–4): 314–327. Distribution of Bufotes latastii (Boulenger, 1882), endemic to the Western Himalaya 1* 1 2,3 4 Spartak N. LITVINCHUK , Dmitriy V. SKORINOV , Glib O. MAZEPA & LeO J. BORKIN 1Institute Of Cytology, Russian Academy Of Sciences, Tikhoretsky pr. 4, St. Petersburg 194064, Russia. 2Department of Ecology and EvolutiOn, University of LauSanne, BiOphOre Building, 1015 Lausanne, Switzerland. 3 Department Of EvOlutiOnary BiOlOgy, EvOlutiOnary BiOlOgy Centre (EBC), Uppsala University, Uppsala, Sweden. 4ZoOlOgical Institute, Russian Academy Of Sciences, Universitetskaya nab. 1, St. PeterSburg 199034, Russia. * CorreSpOnding author <[email protected]>. The distribution of Bufotes latastii, a diploid green toad species, is analyzed based on field observations and literature data. 74 localities are known, although 7 ones should be confirmed. The range of B. latastii is confined to northern Pakistan, Kashmir Valley and western Ladakh in India. All records of “green toads” (“Bufo viridis”) beyond this region belong to other species, both to green toads of the genus Bufotes or to toads of the genus Duttaphrynus. B. latastii is endemic to the Western Himalaya. Its allopatric range lies between those of bisexual triploid green toads in the west and in the east. B. latastii was found at altitudes from 780 to 3200 m above sea level. Environmental niche modelling was applied to predict the potential distribution range of the species. Altitude was the variable with the highest percent contribution for the explanation of the species distribution (36 %). urn:lSid:zOobank.Org:pub:0C76EE11-5D11-4FAB-9FA9-918959833BA5 INTRODUCTION Bufotes latastii (fig. 1) iS a relatively cOmmOn green toad species which spreads in KaShmir Valley, Ladakh and adjacent regiOnS Of nOrthern India and PakiStan. -

Current Affairs October 2020
Current Affairs 2020 Current Affairs October 2020 International Day of Rural Women 2020 International Day of Rural Women is celebrated on 15 October. From agriculture to food security, nutrition, land and natural resource management, domestic care and work, rural women are at the forefront and are taking charge by being in the driver's seat. The International Day of Rural Women was created in 1995 by Civil society organizations at the Fourth World Conference on Women in Beijing and was declared an official UN Day in 2007 by the UN General Assembly. From agriculture to food security, nutrition, land and natural resource management, domestic care and work, rural women are at the forefront. The theme for this International Day of Rural Women is “Building rural women’s resilience in the wake of COVID-19,” to create awareness of these women’s struggles, their needs, and their critical and key role in our society. Cabinet approved Special Package for UT of Jammu & Kashmir and Ladakh Union Cabinet has approved a Special Package worth Rs. 520 crore in the UTs of J&K and Ladakh for a period of five years till FY 2023-24 and ensure funding of DeendayalAntyodaya Yojana - National Rural Livelihoods Mission (DAY-NRLM) in the UTs of Jammu and Kashmir & Ladakh on a demand driven basis without linking allocation with poverty ratio during this extended period. This will ensure sufficient funds under the Mission, as per need to the UTs and is also in line with Government of India's aim to universalize all centrally sponsored beneficiary-oriented schemes in the UTs of J&K and Ladakh in a time bound manner. -
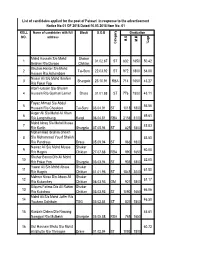
1 Mohd Hussain S/O Mohd Ibrahim R/O Dargoo Shakar Chiktan 01.02
List of candidates applied for the post of Patwari in response to the advertisement Notice No:01 OF 2018 Dated:10.03.2018 Item No: 01 ROLL Name of candidates with full Block D.O.B Graduation NO. address M.O M.M %age Category Category Mohd Hussain S/o Mohd Shakar 1 01.02.87 ST 832 1650 50.42 Ibrahim R/o Dargoo Chiktan Ghulam Haider S/o Mohd 2 Tai-Suru 22.03.92 ST 972 1800 54.00 Hassan R/o Achambore Nissar Ali S/o Mohd Ibrahim 3 Shargole 23.10.91 RBA 714 1650 43.27 R/o Fokar Foo Altaf Hussain S/o Ghulam 4 Hussain R/o Goshan Lamar Drass 01.01.88 ST 776 1800 43.11 Fayaz Ahmad S/o Abdul 5 56.56 Hussain R/o Choskore Tai-Suru 03.04.91 ST 1018 1800 Asger Ali S/o Mohd Ali Khan 6 69.61 R/o Longmithang Kargil 06.04.81 RBA 2158 3100 Mohd Ishaq S/o Mohd Mussa 7 45.83 R/o Karith Shargole 07.05.94 ST 825 1800 Mohammad Ibrahim Sheikh 8 S/o Mohammad Yousf Sheikh 53.50 R/o Pandrass Drass 05.09.94 ST 963 1800 Nawaz Ali S/o Mohd Mussa Shakar 9 60.00 R/o Hagnis Chiktan 27.07.88 RBA 990 1650 Shahar Banoo D/o Ali Mohd 10 52.00 R/o Fokar Foo Shargole 03.03.94 ST 936 1800 Yawar Ali S/o Mohd Abass Shakar 11 61.50 R/o Hagnis Chiktan 01.01.96 ST 1845 3000 Mehrun Nissa D/o Abass Ali Shakar 12 51.17 R/o Kukarchey Chiktan 06.03.93 OM 921 1800 Bilques Fatima D/o Ali Rahim Shakar 13 66.06 R/o Kukshow Chiktan 03.03.93 ST 1090 1650 Mohd Ali S/o Mohd Jaffer R/o 14 46.50 Youkma Saliskote TSG 03.02.84 ST 837 1800 15 Kunzais Dolma D/o Nawang 46.61 Namgyal R/o Mulbekh Shargole 05.05.88 RBA 769 1650 16 Gul Hasnain Bhuto S/o Mohd 60.72 Ali Bhutto R/o Throngos Drass 01.02.94 ST -

Sr. Form No. Name Parentage Address District Category MM MO %Age 1 1898155 MOHD BAQIR MOHAMMED ALI FAROONA P-O SALISKOTE
Selection List of candidates who have applied for admission to B. Ed Programme (Kargil Chapter) offered through Directorate of Admisssions, University of Kashmir session-2018 Sr. Form No. Name Parentage Address District Category MM MO %age OM 1 1898155 MOHD BAQIR MOHAMMED ALI FAROONA P-O SALISKOTE, KARGIL KARGIL ST 9 7.09 78.78 2 1898735 SHAHAR BANOO MOHAMMAD BAQIR BAROO KARGIL KARGIL ST 10 7.87 78.70 3 1895262 FARIDA BANOO MOHD HUSSAIN SHAKAR KARGIL ST 2400 1800 75.00 VILLAGE PASHKUM DISTRICT KARGIL, 4 1897102 HABIBULLAH MOHD BAQIR LADAKH. KARGIL ST 3000 2240 74.67 5 1894751 ANAYAT ALI MOHD SOLEH STICKCHEY CHOSKORE KARGIL ST 2400 1776 74.00 6 1898483 STANZIN SALTON TASHI SONAM R/O MULBEK TEHSIL SHARGOLE KARGIL ST 3000 2177 72.57 7 1892415 IZHAR HUSSAIN NIYAZ ALI TITICHUMIK BAROO POST OFFICE BAROO KARGIL ST 3600 2590 71.94 8 1897301 MOHD HASSAN HADIRE MOHD IBRAHIM HARDASS GRONJUK THANG KARGIL KARGIL ST 3100 2202 71.03 9 1896791 MOHD HUSSAIN GHULAM MOHD ACHAMBORE TAISURU KARGIL KARGIL ST 4000 2835 70.88 10 1898160 MOHD HUSSAIN MOHD TOHA KHANGRAL,CHIKTAN,KARGIL KARGIL ST 3400 2394 70.41 11 1898257 MARZIA BANOO MOHD ALI R/O SAMRAH CHIKTAN KARGIL KARGIL ST 10 7 70.00 12 1893813 ZAIBA BANOO KACHO TURAB SHAH YABGO GOMA KARGIL KARGIL ST 2100 1466 69.81 13 1894898 MEHMOOD MOHD ALI LANKERCHEY KARGIL ST 4000 2784 69.60 14 1894959 SAJAD HUSSAIN MOHD HASSAN ACHAMBORE TAISURU KARGIL ST 3000 2071 69.03 15 1897813 IMRAN KHAN AHMAD KHAN CHOWKIAL DRASS KARGIL RBA 4650 3202 68.86 16 1897210 ARCHO HAKIMA SYED ALI SALISKOTE TSG KARGIL ST 500 340 68.00 17 -

A Pilot Survey of the Avifauna of Rangdum Valley, Kargil, Ladakh (Indian Trans-Himalaya)
Journal of Threatened Taxa | www.threatenedtaxa.org | 26 May 2015 | 7(6): 7274–7281 A pilot survey of the avifauna of Rangdum Valley, Kargil, Ladakh (Indian Trans-Himalaya) ISSN 0974-7907 (Online) 1 2 3 Short Communication Short Tanveer Ahmed , Afifullah Khan & Pankaj Chandan ISSN 0974-7893 (Print) 1,2 Aligarh Muslim University, Department of Wildlife Sciences, Aligarh, Uttar Pradesh 202002, India OPEN ACCESS 3 WWF-India, 172-B, Lodhi Estate, New Delhi 110003, India 1 [email protected] (corresponding author), 2 [email protected],3 [email protected] Abstract: An avifaunal survey of Rangdum Valley in Kargil District, Pradesh) and Ladakh (Jammu & Kashmir) at an average Jammu & Kashmir, India was carried out between June and July 2011. altitude of over 4000m. In Ladakh, studies on avifauna McKinnon’s species richness and total count methods were used. A total of 69 species were recorded comprising six passage migrants, were initiated by A.L. Adam as early as 1859 (Adam 25 residents, 36 summer visitors and three vagrants. The recorded 1859). Some avifaunal surveys in this region were species represents seven orders and 24 families, accounting for 23% th of the species known from Ladakh. A majority of the bird species are carried out in early 20 century (Ludlow 1920; Wathen insectivores. 1923; Osmaston 1925, 1927). Later, more studies on avian species in different parts of Ladakh were Keywords: Avifauna, feeding guild, Ladakh, Rangdum Valley, status. carried out by Holmes (1986), Mallon (1987), Mishra & Humbert-Droz (1998), Singh & Jayapal (2000), Pfister The Himalaya constitute one of the richest and (2001), Namgail (2005), Sangha & Naoroji (2005a,b), most unique ecosystems on the earth. -

OU1901 092-099 Feature Cycling Ladakh
Cycling Ladakh Catching breath on the road to Rangdum monastery PICTURE CREDIT: Stanzin Jigmet/Pixel Challenger Breaking the There's much more to Kate Leeming's pre- Antarctic expeditions than preparation. Her journey in the Indian Himalaya was equally about changing peoples' lives. WORDS Kate Leeming 92 93 Cycling Ladakh A spectacular stream that eventually flows into the Suru River, on the 4,000m plains near Rangdum nergy was draining from my legs. My heart pounded hard and fast, trying to replenish my oxygen deficit. I gulped as much of the rarified air as I could, without great success; at 4,100m, the atmospheric oxygen is at just 11.5 per cent, compared to 20.9 per cent at sea level. As I continued to ascend towards the snow-capped peaks around Sirsir La pass, the temperature plummeted and my body, drenched in a lather of perspiration, Estarted to get cold, further sapping my energy stores. Sirsir La, at 4,828m, is a few metres higher than Europe’s Mont Blanc, and I was just over half way up the continuous 1,670m ascent to get there. This physiological response may have been a reality check, but it was no surprise. The ride to the remote village of Photoksar on the third day of my altitude cycling expedition in the Indian Himalaya had always loomed as an enormous challenge, and I was not yet fully acclimatised. I drew on experience to pace myself: keeping the pedals spinning in a low gear, trying to relax as much as possible and avoiding unnecessary exertion. -
Statistical Handbook District Kargil 2018-19
Statistical Handbook District Kargil 2018-19 “STATISTICAL HANDBOOK” DISTRICT KARGIL UNION TERRITORY OF LADAKH FOR THE YEAR 2018-19 RELEASED BY: DISTRICT STATISTICAL & EVALUATION OFFICE KARGIL D.C OFFICE COMPLEX BAROO KARGIL J&K. TELE/FAX: 01985-233973 E-MAIL: [email protected] Statistical Handbook District Kargil 2018-19 THE ADMINISTRATION OF UNION TERRITORY OF LADAKH, Chairman/ Chief Executive Councilor, LAHDC Kargil Phone No: 01985 233827, 233856 Message It gives me immense pleasure to know that District Statistics & Evaluation Agency Kargil is coming up with the latest issue of its ideal publication “Statistical Handbook 2018-19”. The publication is of paramount importance as it contains valuable statistical profile of different sectors of the district. I hope this Hand book will be useful to Administrators, Research Scholars, Statisticians and Socio-Economic planners who are in need of different statistics relating to Kargil District. I appreciate the efforts put in by the District Statistics & Evaluation Officer and the associated team of officers and officials in bringing out this excellent broad based publication which is getting a claim from different quarters and user agencies. Sd/= (Feroz Ahmed Khan ) Chairman/Chief Executive Councilor LAHDC, Kargil Statistical Handbook District Kargil 2018-19 THE ADMINISTRATION OF UNION TERRITORY OF LADAKH District Magistrate, (Deputy Commissioner/CEO) LAHDC Kargil Phone No: 01985-232216, Tele Fax: 232644 Message I am glad to know that the district Statistics and Evaluation Office Kargil is releasing its latest annual publication “Statistical Handbook” for the year 2018- 19. The present publication contains statistics related to infrastructure as well as Socio Economic development of Kargil District. -

Kargil Operation 1999
KARGIL OPERATION 1999 The Kargil War, also known as the Kargil conflict was an armed conflict between India and Pakistan that took place between May and July 1999 in the Kargil district of Kashmir and elsewhere along the Line of Control (LOC). In India, the conflict is also referred to as Operation Vijay which was the name of the Indian operation to clear the Kargil sector.The war is the most recent example of high-altitude warfare in mountainous terrain, and as such posed significant logistical problems for the combating sides.The cause of the war was the infiltration of Pakistani soldiers disguised as Kashmiri militants into positions on the Indian side of the LOC which serves as the border between the two states. During the initial stages of the war, Pakistan blamed the fighting entirely on independent Kashmiri insurgents, but documents left behind by casualties and later statements by Pakistan's Prime Minister and Chief of Army Staff showed involvement of Pakistani paramilitary forces led by General Ashraf Rashid. The Indian Army, later supported by the Indian Air Force, recaptured a majority of the positions on the Indian side of the LOC infiltrated by the Pakistani troops and militants. Facing international diplomatic opposition, the Pakistani forces withdrew from the remaining Indian positions along the LOC. There were three major phases to the Kargil War. First, Pakistan infiltrated forces into the Indian-controlled section of Kashmir and occupied strategic locations enabling it to bring NH1 within range of its artillery fire. The next stage consisted of India discovering the infiltration and mobilising forces to respond to it. -

Pakistan S Strategic Blunder at Kargil, by Brig Gurmeet
Pakistan’s Strategic Blunder at Kargil Gurmeet Kanwal Cause of Conflict: Failure of 10 Years of Proxy War India’s territorial integrity had not been threatened seriously since the 1971 War as it was threatened by Pakistan’s ill-conceived military adventure across the Line of Control (LoC) into the Kargil district of Jammu and Kashmir (J&K) in the summer months of 1999. By infiltrating its army soldiers in civilian clothes across the LoC, to physically occupy ground on the Indian side, Pakistan added a new dimension to its 10-year-old ‘proxy war’ against India. Pakistan’s provocative action compelled India to launch a firm but measured and restrained military operation to clear the intruders. Operation ‘Vijay’, finely calibrated to limit military action to the Indian side of the LoC, included air strikes from fighter-ground attack (FGA) aircraft and attack helicopters. Even as the Indian Army and the Indian Air Force (IAF) employed their synergised combat potential to eliminate the intruders and regain the territory occupied by them, the government kept all channels of communication open with Pakistan to ensure that the intrusions were vacated quickly and Pakistan’s military adventurism was not allowed to escalate into a larger conflict. On July 26, 1999, the last of the Pakistani intruders was successfully evicted. Why did Pakistan undertake a military operation that was foredoomed to failure? Clearly, the Pakistani military establishment was becoming increasingly frustrated with India’s success in containing the militancy in J&K to within manageable limits and saw in the Kashmiri people’s open expression of their preference for returning to normal life, the evaporation of all their hopes and desires to bleed India through a strategy of “a thousand cuts”. -

Contemporary Ladakh: Identifying the “Other” in Buddhist-Muslim
Issue Brief # 234 August 2013 Innovative Research | Independent Analysis | Informed Opinion Contemporary Ladakh Identifying the “Other” in Buddhist-Muslim Transformative Relations Sumera Shafi Jawaharlal Nehru University Changes in the relationship of major sub- identity being a fluid concept is often divisions of a society are reflected in the misappropriated by a certain section of development of active scholarly analysis the society for the furtherance of their of those changes. The ongoing interests. It is the age old congenial inter- transformations in the Ladakhi society communal networks that face the brunt of have also attracted certain amount of such maneuverings leading to irrevocable attention from scholars from within and transformations in the everyday relations. outside the area. Currently there is a select list of material for one to be able to This essay is mainly based on available evaluate the trajectory of social change literature and keen observations made as in Ladakh and also to identify the a native of Ladakh. The conclusions are causative factors for such change. In that preliminary in nature and aimed at the direction this paper seeks to specify the possibility of bringing out a theoretical process of identity formation amongst the standpoint through the use of empirical Ladakhis by emphasizing how the data. differential circumstances faced by the Who is the other? locals has led them to approximate religion as the prime identity marker. This essay does not aim at identifying the Through the illustration of Ladakh’s other but in contrast it is an attempt to experience, this essay seeks to argue that illustrate the complexity involved in doing just that! Identity is a fluid concept and there are This essay was initially presented in a multiple identities which an individual can conference organized by the IPCS in approximate based on various collaboration with the India circumstances. -

List of Candidates Applied for the Post of General Line Teacher In
List of candidates applied for the post of General Line Teacher in response to the advertisement Notice No:02 OF 2018 Dated:15.03.2018 Item No: 01 Graduation P.G B.Ed M.Ed Name of candidates with full ROLL NO. Block Stream JRF address P.hD M.Phill M.O M.O M.O M.O NET/SET M.M M.M M.M M.M Category %age %age %age %age Mohd Ibrahim S/0 Mirza Ali S/0 1 Saliskote TSG 02.04.91 ST 900 1800 50.00 6 10 60.00 0 0 #DIV/0! 0 0 #DIV/0! 0 0 0 0 Arts Tohera Banoo D/0 Haji Mohd 2 Hassan R/0 Andoo Shargol 02.04.93 ST 908 1800 50.44 0 0 #DIV/0! 0 0 #DIV/0! 0 0 #DIV/0! 0 0 0 0 Arts Kaniz Fatima D/0 Mohd Toha 3 R/0 Taisuru Taisuru 06.08.91 RBA 1012 1800 56.22 0 0 #DIV/0! 742 900 82.44 0 0 #DIV/0! 0 0 0 0 Arts Saleema Khanum D/0 Mohd 4 Ali Khan R/0 Balti Bazar Kargil 03.12.90 RBA 892 1800 49.56 6.3 10 63.00 709 900 78.78 0 0 #DIV/0! 0 0 0 0 Arts Farida Batool D/0 haji Hadi R/0 5 Staikchey Kargil Kargil 04.03.89 ST 769 1800 42.72 549 1000 54.90 0 0 #DIV/0! 0 0 #DIV/0! 0 0 0 0 Arts Sajida Batool D/0 Mohmmad 6 Sadiq R/0 Stikchey Kargil 15.01.93 ST 893 1650 54.12 1805 3200 56.41 0 0 #DIV/0! 0 0 #DIV/0! 0 0 0 0 Arts Mohd Jaffar S/0 Ali Mohd R/0 7 Saliskote TSG 10.11.89 ST 845 1800 46.94 656 1000 65.60 0 0 #DIV/0! 0 0 #DIV/0! 0 0 0 0 Arts 8 Imran Ali Khan S/0 Mohd Ali Kargil 05.12.87 RBA 1023 1800 56.83 1512 2500 60.48 0 0 #DIV/0! 0 0 #DIV/0! Net 0 0 0 Medical Khan R/0 Balti Bazar 9 Syeda Batool D/0 Haji Hadi Kargil 14.03.93 ST 849 1650 51.45 931 1800 51.72 0 0 #DIV/0! 0 0 #DIV/0! 0 0 0 0 Ats R/0 Staikchey 10 Gulshan Arah D/0 Abdul Aziz Drass 02.03.89 ALC 765 1800 -

China and Kashmir* Buildup Along the Indo-Pak Border in 2002 (Called Operation Parakram in India)
China and Kashmir* buildup along the Indo-Pak border in 2002 (called Operation Parakram in India). Even if the case may by JABIN T. Jacob be made that such support to Pakistan has strength- ened Pakistan’s hands on the Kashmir dispute, it is difficult to draw a direct link between the twists and turns in the Kashmir situation and Chinese arms supplies to Pakistan. Further, China has for over two Perceptions about the People’s Republic of China’s decades consistently called for a peaceful resolution position on Kashmir have long been associated with of the Kashmir dispute, terming it a dispute “left over its “all-weather” friendship with Pakistan. However, from history.” Both during Kargil and Operation the PRC’s positions on Kashmir have never been Parakram, China refused to endorse the Pakistani consistently pro-Pakistan, instead changing from positions or to raise the issue at the United Nations. disinterest in the 1950s to open support for the Paki- Coupled with rising trade and the continuing border stani position in the subsequent decades to greater dialogue between India and China, this has given rise neutrality in the 1980s and since. While China has to hopes in India that the Kashmir dispute will no China’s positions on continued military support to Pakistan even during longer be a card the Chinese will use against it. Kashmir have never been military conflicts and near-conflicts between India and Pakistan, its stance on Kashmir has shifted consistently pro-Pakistan, gradually in response to the prevailing domestic, China and Pakistan Occupied Kashmir instead changing from dis- regional, and international situations.