DREF Operation”- Final Report Page | 3 Based Activities
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

32 Mohamadou Tchinta
1 LASDEL Laboratoire d’études et recherches sur les dynamiques sociales et le développement local _________ BP 12901, Niamey, Niger – tél. (227) 72 37 80 BP 1383, Parakou, Bénin – tél. (229) 61 16 58 Observatoire de la décentralisation au Niger (enquête de référence 2004) Les pouvoirs locaux dans la commune de Tchintabaraden Abdoulaye Mohamadou Enquêteurs : Afélane Alfarouk et Ahmoudou Rhissa février 05 Etudes et Travaux n° 32 Financement FICOD (KfW) 2 Sommaire Introduction 3 Les Kel Dinnig : de la confédération aux communes 3 Objectifs de l’étude et méthodologie 4 1. Le pouvoir local et ses acteurs 6 1.1. Histoire administrative de l’arrondissement et naissance d’un centre urbain 6 1.2. Les acteurs de l’arène politique locale 7 2. Le découpage de l’arrondissement de Tchintabaraden 19 2.1. Logiques territoriale et logiques sociales 19 2.2. Le choix des bureaux de vote 22 2.3. Les stratégies des partis politiques pour le choix des conseillers 23 2.4. La décentralisation vue par les acteurs 23 3. L’organisation actuelle des finances locales 25 3.1. Les projets de développement 25 3. 2. Le budget de l’arrondissement 26 Conclusion 33 3 Introduction Les Kel Dinnig : de la confédération aux communes L’arrondisssement de Tchintabaraden correspondait avant la création de celui d’Abalak en 1992 à l’espace géographique et social des Touareg Iwillimenden ou Kel Dinnig. Après la révolte de Kaocen en 1916-1917 et son anéantissement par les troupes coloniales françaises, l’aménokalat des Iwilimenden fut disloqué et réparti en plusieurs groupements. Cette technique de diviser pour mieux régner, largement utilisée par l’administration coloniale, constitue le point de départ du découpage administratif pour les populations de cette région. -

Dynamique Des Conflits Et Médias Au Niger Et À Tahoua Revue De La Littérature
Dynamique des Conflits et Médias au Niger et à Tahoua Revue de la littérature Décembre 2013 Charline Burton Rebecca Justus Contacts: Charline Burton Moutari Aboubacar Spécialiste Conception, Suivi et Coordonnateur National des Evaluation – Afrique de l’Ouest Programmes - Niger Abidjan, Côte d’Ivoire [email protected] + 227 9649 00 39 [email protected] +225 44 47 24 57 +227 90 60 54 96 Dynamique des conflits et Médias au Niger et à Tahoua | PAGE 2 Table des matières 1. Résumé exécutif ...................................................................................................... 4 Contexte ................................................................................................. 4 Objectifs et méthodologie ........................................................................ 4 Résultats principaux ............................................................................... 4 2. Introduction ............................................................................................................. 7 2.1 Contexte de la revue de littérature ............................................................... 7 2.2 Méthodologie et questions de recherche ....................................................... 7 3. Contexte général du Niger .................................................................................. 10 3.1 Démographie ............................................................................................. 10 3.2 Situation géographique et géostratégique ............................................ -

NIGER: Carte Administrative NIGER - Carte Administrative
NIGER - Carte Administrative NIGER: Carte administrative Awbari (Ubari) Madrusah Légende DJANET Tajarhi /" Capital Illizi Murzuq L I B Y E !. Chef lieu de région ! Chef lieu de département Frontières Route Principale Adrar Route secondaire A L G É R I E Fleuve Niger Tamanghasset Lit du lac Tchad Régions Agadez Timbuktu Borkou-Ennedi-Tibesti Diffa BARDAI-ZOUGRA(MIL) Dosso Maradi Niamey ZOUAR TESSALIT Tahoua Assamaka Tillabery Zinder IN GUEZZAM Kidal IFEROUANE DIRKOU ARLIT ! BILMA ! Timbuktu KIDAL GOUGARAM FACHI DANNAT TIMIA M A L I 0 100 200 300 kms TABELOT TCHIROZERINE N I G E R ! Map Doc Name: AGADEZ OCHA_SitMap_Niger !. GLIDE Number: 16032013 TASSARA INGALL Creation Date: 31 Août 2013 Projection/Datum: GCS/WGS 84 Gao Web Resources: www.unocha..org/niger GAO Nominal Scale at A3 paper size: 1: 5 000 000 TILLIA TCHINTABARADEN MENAKA ! Map data source(s): Timbuktu TAMAYA RENACOM, ARC, OCHA Niger ADARBISNAT ABALAK Disclaimers: KAOU ! TENIHIYA The designations employed and the presentation of material AKOUBOUNOU N'GOURTI I T C H A D on this map do not imply the expression of any opinion BERMO INATES TAKANAMATAFFALABARMOU TASKER whatsoever on the part of the Secretariat of the United Nations BANIBANGOU AZEY GADABEDJI TANOUT concerning the legal status of any country, territory, city or area ABALA MAIDAGI TAHOUA Mopti ! or of its authorities, or concerning the delimitation of its YATAKALA SANAM TEBARAM !. Kanem WANZERBE AYOROU BAMBAYE KEITA MANGAIZE KALFO!U AZAGORGOULA TAMBAO DOLBEL BAGAROUA TABOTAKI TARKA BANKILARE DESSA DAKORO TAGRISS OLLELEWA -

(Between Warrior and Helplessness in the Valley of Azawaɤ ) Appendix 1: Northern Mali and Niger Tuareg Participation in Violenc
Appendix 1: Northern Mali and Niger Tuareg Participation in violence as perpetrators, victims, bystanders from November 2013 to August 2014 (Between Warrior and Helplessness in the Valley of Azawaɤ ) Northern Mali/Niger Tuareg participation in violence (perpetrators, victims, bystanders) November 2013 – August 2014. Summarized list of sample incidents from Northern Niger and Northern Mali from reporting tracking by US Military Advisory Team, Niger/Mali – Special Operations Command – Africa, USAFRICOM. Entries in Red indicate no Tuareg involvement; Entries in Blue indicate Tuareg involvement as victims and/or perpetrators. 28 November – Niger FAN arrests Beidari Moulid in Niamey for planning terror attacks in Niger. 28 November – MNLA organizes protest against Mali PMs Visit to Kidal; Mali army fires on protestors killing 1, injuring 5. 30 November – AQIM or related forces attack French forces in Menaka with Suicide bomber. 9 December – AQIM and French forces clash in Asler, with 19 casualties. 14 December – AQIM or related forces employ VBIED against UN and Mali forces in Kidal with 3 casualties. 14 December – MUJWA/AQIM assault a Tuareg encampment with 2 casualties in Tarandallet. 13 January – AQIM or related forces kidnap MNLA political leader in Tessalit. 16 January – AQIM kidnap/executes MNLA officer in Abeibera. 17 January – AQIM or related forces plant explosive device near Christian school and church in Gao; UN forces found/deactivated device. 20 January – AQIM or related forces attacks UN forces with IED in Kidal, 5 WIA. 22 January – AQIM clashes with French Army forces in Timbuktu with 11 Jihadist casualties. 24 January – AQIM or related forces fires two rockets at city of Kidal with no casualties. -
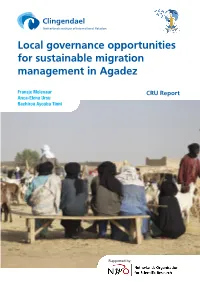
Local Governance Opportunities for Sustainable Migration Management in Agadez
Local governance opportunities for sustainable migration management in Agadez Fransje Molenaar CRU Report Anca-Elena Ursu Bachirou Ayouba Tinni Supported by: Local governance opportunities for sustainable migration management in Agadez Fransje Molenaar Anca-Elena Ursu Bachirou Ayouba Tinni CRU Report October 2017 October 2017 © Netherlands Institute of International Relations ‘Clingendael’. Cover photo: Men sitting on a bench at the Agadez Market. © Boris Kester / traveladventures.org Unauthorised use of any materials violates copyright, trademark and / or other laws. Should a user download material from the website or any other source related to the Netherlands Institute of International Relations ‘Clingendael’, or the Clingendael Institute, for personal or non-commercial use, the user must retain all copyright, trademark or other similar notices contained in the original material or on any copies of this material. Material on the website of the Clingendael Institute may be reproduced or publicly displayed, distributed or used for any public and non-commercial purposes, but only by mentioning the Clingendael Institute as its source. Permission is required to use the logo of the Clingendael Institute. This can be obtained by contacting the Communication desk of the Clingendael Institute ([email protected]). The following web link activities are prohibited by the Clingendael Institute and may present trademark and copyright infringement issues: links that involve unauthorized use of our logo, framing, inline links, or metatags, as well as hyperlinks or a form of link disguising the URL. About the authors Fransje Molenaar is a research fellow at the Clingendael Institute’s Conflict Research Unit Anca-Elena Ursu is a research assistant at the Clingendael Institute’s Conflict Research Unit Bachirou Ayouba Tinni is a PhD student at the University of Niamey The Clingendael Institute P.O. -
Assessment of Chronic Food Insecurity in Niger
Assessment of Chronic Food Insecurity in Niger Analysis Coordination March 2019 Assessment of Chronic Food Insecurity in Niger 2019 About FEWS NET Created in response to the 1984 famines in East and West Africa, the Famine Early Warning Systems Network (FEWS NET) provides early warning and integrated, forward-looking analysis of the many factors that contribute to food insecurity. FEWS NET aims to inform decision makers and contribute to their emergency response planning; support partners in conducting early warning analysis and forecasting; and provide technical assistance to partner-led initiatives. To learn more about the FEWS NET project, please visit www.fews.net. Acknowledgements This publication was prepared under the United States Agency for International Development Famine Early Warning Systems Network (FEWS NET) Indefinite Quantity Contract, AID-OAA-I-12-00006. The author’s views expressed in this publication do not necessarily reflect the views of the United States Agency for International Development or the United States Government. Recommended Citation FEWS NET. 2019. Assessment of Chronic Food Insecurity in Niger. Washington, DC: FEWS NET. Famine Early Warning Systems Network ii Assessment of Chronic Food Insecurity in Niger 2019 Table of Contents Executive Summary ..................................................................................................................................................................... 1 Background ............................................................................................................................................................................. -

Ref Agadeza1.Pdf
REGION D'AGADEZ: Carte référentielle Légende L i b y e ± Chef lieu de région Chef lieu de département localité Route principale Route secondaire ou tertiaire Frontière internationale Frontière régionale Cours d'eau MADAMA Région d'Agadez A l g é r i e ☶ Population Djado DJABA DJADO CHIRFA KANARIA I-N-AZAOUA SARA BILMA DAOTIMMI I-N-TADERA ☶ 17 459 TOUARET SEGUEDINE IFEROUANE TAGHAJIT TAMJIT TAZOUROUTETASSOS INTIKIKITENE OURARENE AGALANGAÏ ☶ 32 864 DOUMBA EZAZAW FARAZAKAT ANEY ASSAMAKKA ABARGOT TEZIRZEK LOTEY TCHOUGOY TIRAOUENE TAKARATEMAMANAT ZOURIKA EMI TCHOUMA AZATRAYA AGREROUM ET TCHWOUN ARLIT Gougaram ACHENOUMA IFEROUANE ISSAWANE ARRIGUI Dirkou ACHEGOUR TEMET DIRKOU ☶ 103 369 INIGNAOUEI TILALENE ARAKAW MAGHET TAKRIZA TARHMERT ARLIT AGAMGAM BILMA ANOU OUACHCHERENE TCHIGAYEN TAZOURAT TAGGAFADI Dannet GOUGARAM SIDAOUET ZOMO ASSODE IBOUL TCHILHOURENE ERISMALAN TIESTANE Bilma MAZALALE AJIWA INNALARENE TAZEWET AGHAROUS ESSELEL ZOBABA ANOUZAGHARAN DANNET FAYAYE Timia FACHI TIGUIR AJIR IMOURAREN TIMIA FACHI MARI Fachi TAKARACHE ZIKAT OFENE MALLETAS AKEREBREB ABELAJOUAD TCHINOUGOUWENEARITAOUA IN-ABANGHARIT TAMATEDERITTASSEDET ASSAK HARAU INTAMADE T c h a d EGHARGHAR TILIA OOUOUARI Dabaga ELMEKI BOURNI TIDEKAL SEKIRET ASSESA MERIG AKARI TELOUES EGANDAWEL AOUDERAS EOULEM SOGHO TAGAZA ATKAKI TCHIROZERINE TABELOT EGHOUAK M a l i AZELIK DABLA ABARDOKH TALAT INGAL IMMASSATANE AMAN NTEDENT ELDJIMMA ☶ 241 007 GUERAGUERA TEGUIDDA IN TESSOUM ABAZAGOR Tabelot FAGOSCHIA DABAGA TEGUIDDA IN TAGAIT I-N-OUTESSANE ☶ EKIZENGUI AGALGOU 51 818 TCHIROZERINE INGOUCHIL -

Agadez, Niger
Mayors Dialogue on Growth and Solidarity City profile: Agadez, Niger Population: 137,354 (2017 ) GDP per capita: $555 (2019, national) Major industries: trade and logistics, livestock, agriculture Percentage of migrants: 1% (2017, national) Mayor’s name: Dr Boukari Mamane | Next election date: 2021 Socioeconomic profile Migration profile Agadez is the fifth largest city in Niger, capital Agadez is home to a large number of internal rural of both the Agadez Region and Aïr, a traditional migrants who moved to the city in the 1970s and Tuareg–Berber federation (Institut National de la 1980s to escape severe droughts. Changes in rainfall Statistique, 2014). The city is geographically dispersed causing both drought and flash floods continue and is home to 137,354 individuals over an area to displace people across Niger (121,000 in 2019) of 213 km2 (Institut National de la Statistique du (Internal Displacement Monitoring Centre, n.d.). In Niger, 2020a). Since 2000, the population has been terms of international migration, Niger is home to growing by 3.17% annually (Institut National de la 295,600 foreign-born residents, mostly from nearby Statistique du Niger, 2019). A substantial proportion countries (Nigeria, Mali and Burkina Faso) (EU of Agadez residents are nomadic or semi-nomadic Commission, 2019). Out of Niger’s population of people (Molenaar et al., 2017). The city’s population around 21.5 million, this implies a national migrant is younger than the Nigerien average, with 40% population of around 1% (EU Commission, 2019). between the ages of 15 and 39 (Institut National de la In 2017, there were also 165,700 refugees and 300 Statistique du Niger, 2020b). -

Rethinking the Response to Jihadist Groups Across the Sahel
Research Rethinking the response Paper to jihadist groups across Africa Programme the Sahel March 2021 Marc-Antoine Pérouse de Montclos Chatham House, the Royal Institute of International Affairs, is a world-leading policy institute based in London. Our mission is to help governments and societies build a sustainably secure, prosperous and just world. Contents Summary 2 01 Introduction 3 02 Governments and armies in the Sahel: structural failures 6 03 The case of northern Mali 10 04 Niger: a counterexample 14 05 The role of local militia groups 18 06 The limitations of proxy warfare 20 07 Conclusion: the end of military cooperation? 24 About the author 27 Acknowledgments 27 1 Chatham House Summary — Rather than the ideology of global jihad, the driving force behind the emergence and resilience of non-state armed groups in the Sahel is a combination of weak states, corruption and the brutal repression of dissent, embodied in dysfunctional military forces. — The dominant narrative of a global jihadi threat has overshadowed the reality of the key role played by military nepotism, prevarication and indiscipline in generating and continuing conflict in the Sahel – problems that long predated the ‘war on terror’. Moreover, it has pushed the international community to intervene to regulate local conflicts that have little to do with global terrorism or religious indoctrination. — Mali offers a clear example of this. The widespread use of poorly controlled militias, the collapse of its army, two coups – in 2012 and 2020 – and a weak state presence in rural areas, on top of a history of repression and abuse suffered by its northern population, has done much more to drive the growth of insurgent groups than did the fall of the Gaddafi regime in Libya in 2011, Salafist indoctrination, or alleged support from Arab countries. -

Risk and Resilience Assessment Niger
Risk and Resilience Assessment Niger 2016 Annex 2: Niger Risk and Resilience Assessment 1) Background Niger at a glance The republic of Niger is a landlocked country located where northern and sub-Saharan Africa meet. It is a vast territory of 1,3 million km2, with a low population density given its 19.1 million inhabitants (2014 census). Niger has the highest demographic growth rate in the world, at 3,9 percent per year, and a very young population, 50 percent of which is under the age of fifteen. It is home to several ethnic groups, including the Hausa (which compose around half the population, present in the South East), Djerma (South West), Tuareg (North), Fulani (South-West), Arab (South), and Kanuri (South East). Niger’s economy largely depends on the agriculture and livestock sectors. Extractive industries are also a major contributor to the economy, amounting to 10 percent of the GDP and 50 percent of exportation revenues. Niger is the fourth-largest uranium producer in the world and could become second if the Imouraren site is finally put in production.1 Gold mining has remained largely informal to date, but recently authorities have adopted measures to begin formalizing the sector. Niger is faced with a high incidence of poverty and low human development. In 2014, 44.5 percent of the population was poor,2 and Niger ranked second to last out of 188 countries on the 2016 Human Development Index. Although poverty dropped between 2005 and 2014, it was unable to outpace the rate of demographic growth, which was four times higher during the same period,3 and as a result the absolute number of poor continues to rise. -
Livelihoods Zoning “Plus” Activity in Niger
LIVELIHOODS ZONING “PLUS” ACTIVITY IN NIGER A SPECIAL REPORT BY THE FAMINE EARLY WARNING SYSTEMS NETWORK (FEWS NET) August 2011 Table of Contents Introduction .................................................................................................................................................. 3 Methodology ................................................................................................................................................. 4 National Livelihoods Zones Map ................................................................................................................... 6 Livelihoods Highlights ................................................................................................................................... 7 National Seasonal Calendar .......................................................................................................................... 9 Rural Livelihood Zones Descriptions ........................................................................................................... 11 Zone 1: Northeast Oases: Dates, Salt and Trade ................................................................................... 11 Zone 2: Aïr Massif Irrigated Gardening ................................................................................................ 14 Zone 3 : Transhumant and Nomad Pastoralism .................................................................................... 17 Zone 4: Agropastoral Belt ..................................................................................................................... -

Niger Staple Food and Livestock Market Fundamentals. September 2017
NIGER STAPLE FOOD AND LIVESTOCK MARKET FUNDAMENTALS SEPTEMBER 2017 This publication was produced for review by the United States Agency for International Development. It was prepared by Chemonics International Inc. for the Famine Early Warning Systems Network (FEWS NET), contract number AID-OAA-I-12-00006. The authors’ views expressed in this publication do not necessarily reflect the views of the United States Agency for International Development or the United States government. FEWS NET NIGER Staple Food and Livestock Market Fundamentals 2017 About FEWS NET Created in response to the 1984 famines in East and West Africa, the Famine Early Warning Systems Network (FEWS NET) provides early warning and integrated, forward-looking analysis of the many factors that contribute to food insecurity. FEWS NET aims to inform decision makers and contribute to their emergency response planning; support partners in conducting early warning analysis and forecasting; and provide technical assistance to partner-led initiatives. To learn more about the FEWS NET project, please visit www.fews.net. Disclaimer This publication was prepared under the United States Agency for International Development Famine Early Warning Systems Network (FEWS NET) Indefinite Quantity Contract, AID-OAA-I-12-00006. The authors’ views expressed in this publication do not necessarily reflect the views of the United States Agency for International Development or the United States government. Acknowledgements FEWS NET gratefully acknowledges the network of partners in Niger who contributed their time, analysis, and data to make this report possible. Cover photos @ FEWS NET and Flickr Creative Commons. Famine Early Warning Systems Network ii FEWS NET NIGER Staple Food and Livestock Market Fundamentals 2017 Table of Contents Executive Summary ....................................................................................................................................................................