18Th International Myeloma Workshop 2021 September 8-11, 2021
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
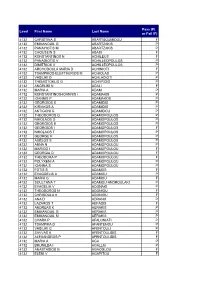
Results Level 3
Pass (P) Level First Name Last Name or Fail (F) 4132 CHRISTINA S ABARTSOUMIDOU F 4132 EMMANOUIL G ABARTZAKIS P 4132 PANAYIOTIS M ABARTZAKIS P 4132 CHOUSEIN S ABASI F 4132 KONSTANTINOS N ACHILEUS F 4132 PANAGIOTIS V ACHILLEOPOULOS P 4132 DIMITRIOS V ACHILLEOPOULOS P 4132 ARCHODOULA MARIA D ACHINIOTI F 4132 TSAMPIKOS-ELEFTHERIOS M ACHIOLAS P 4132 VASILIKI D ACHLADIOTI P 4132 THEMISTOKLIS G ACHYRIDIS P 4132 ANGELIKI N ADALI F 4132 MARIA A ADAM P 4132 KONSTANTINOS-IOANNIS I ADAMAKIS P 4132 IOANNIS P ADAMAKOS P 4132 GEORGIOS S ADAMIDIS P 4132 KIRIAKOS A ADAMIDIS P 4132 ANTIGONI G ADAMIDOU P 4132 THEODOROS G ADAMOPOULOS P 4132 NIKOLAOS G ADAMOPOULOS P 4132 GEORGIOS E ADAMOPOULOS P 4132 GEORGIOS I ADAMOPOULOS F 4132 NIKOLAOS T ADAMOPOULOS P 4132 GEORGE K ADAMOPOULOS P 4132 AGELOS S ADAMOPOULOS P 4132 ANNA N ADAMOPOULOU P 4132 MARIGO I ADAMOPOULOU F 4132 GEORGIA D ADAMOPOULOU F 4132 THEODORA P ADAMOPOULOU F 4132 POLYXENI A ADAMOPOULOU P 4132 IOANNA S ADAMOPOULOU P 4132 FOTIS S ADAMOS F 4132 EVAGGELIA A ADAMOU P 4132 MARIA G ADAMOU F 4132 SOULTANA T ADAMOU-ANDROULAKI P 4132 EVAGELIA V ADONAKI P 4132 THEODOROS N ADONIOU F 4132 CHRISOULA K ADONIOU F 4132 ANA D ADRANJI P 4132 LAZAROS T AEFADIS F 4132 ANDREAS K AERAKIS P 4132 EMMANOUIL G AERAKIS P 4132 EMMANOUIL M AERAKIS P 4132 CHARA P AFALONIATI P 4132 TSAMPIKA D AFANTENOU P 4132 VASILIKI G AFENTOULI P 4132 SAVVAS A AFENTOULIDIS F 4132 ALEXANDROS P AFENTOULIDIS F 4132 MARIA A AGA P 4132 BRUNILDA I AGALLIU P 4132 ANASTASIOS G AGAOGLOU F 4132 ELENI V AGAPITOU F 4132 JOHN K AGATHAGGELOS P 4132 PANAGIOTA -
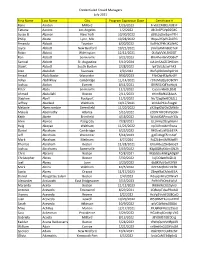
Credentialed Crowd Managers July 2021 First Name Last
Credentialed Crowd Managers July 2021 First Name Last Name City Program Expiration Date Certificate # Rano Aarden Milford 1/26/2023 FrvbECM3ELNUErF Tatiana Aarons Los Angeles 1/2/2022 J8r2x6PSVpDZGKC Susan B. Abanor New York 10/30/2022 s8lELzyDw2qmPTH Philip Abate Lynn, MA 10/28/2022 WqaslYQvPLZk07G Amanda Abbott Taunton 6/20/2022 Ka9Hs2Pkh1KUNAC Joyce Abbott New Bedford 10/21/2021 zVHllaFMm8dCTeK Robin Abbott Wilmington 12/12/2021 0fz5pVVXLSI60OT Ron Abbott Somerville 9/22/2023 8hk4henBxVDbBv7 Samuel Abbott St. Augustine 5/10/2024 xiA1mSAdZE0HG4m Stuart Abbott South Boston 2/28/2022 lpY1blLJbzwFhK3 Alan Abdallah Swansea 2/9/2022 WxFq0DJ9mPqGHof Amaal Abdelkader Worcester 9/30/2023 FYtrOqHF3pfkzOY Adiya Abdilkhay Cambridge 11/14/2021 r97oMqQly3OBcNY Joshua Abdon Everett 8/11/2021 8VW51lQEYwhliyk Peter Abdu Somerville 11/2/2022 Cuaserkl6OLDbIZ Ahmed Abdullahi Boston 2/11/2023 tHImRAfKLS8JsxA Stephen Abell Rockport 11/5/2023 NoT2agXeKIOBZL1 Jeffrey Abellard Waltham 10/17/2021 eCG3eP61sFxog9l Melanie Abercrombie Greenfield 11/20/2022 aY2bpJ0WOsCMN0v Makyla Abernathy Atlanta 5/15/2022 cODN7RFDYaYpDcH Keith Abete Brimfield 4/18/2022 Wxh4f0APmovh33s Alvin Abinas Pasig City 7/28/2021 ULzHHuZOsydr6mI Haig Aboyan Waltham 11/26/2022 np3UfnoLfzH5wca Daniel Abraham Cambridge 6/25/2022 9HDvxEuWGiLiE7A Jeff Abraham Worcester 5/14/2023 gj0TzUxgE5rmA9F Mark Abraham Methuen 4/7/2024 FxZZL4mXMf6JwRY Thomas Abraham Reston 11/28/2021 EVLm0eLZSHSmsq9 Joshua Abrahams Somerville 5/19/2022 Kdp8QRqKtAmGN2h Chris Abrams Boston 10/8/2021 MSbGbeMkEgADg9P Christopher -

En 380 023 AUTHOR TITLE INSTITUTION SPONS AGENCY
DOCUMENT RESUME En 380 023 HE 028 138 AUTHOR Haro, Roberto P.; And Others TITLE Latino Persistence in Higher Education: A 1994 Survey of University of California and California State University Chicano/Latino Students. INSTITUTION Latino Issues Forum, San Francisco, CA. SPONS AGENCY Ford Foundation, New York, N.Y. PUB DATE Sep 94 NOTE 51p. AVAILABLE FROM Latino Issues Forum, 785 Market St., Third Floor, San Francisco, CA 94103 ($5). PUS TYPE Reports Research/Technical (143) EDRS PRICE MF01/PC03 Plus Postage. DESCRIPTORS *Academic Persistence; College Programs; *College Students; Decision Making; Dropout Prevention; Dropout Rate; Family Role; Financial Support; Higher Education; Hispanic American Culture; *Hispanic Americans; Interviews; Mentors; Peer Influence; School Holding Power; State Universities; *Student Characteristics; Student Personnel Services IDENTIFIERS *California State University; ChiOanas; Chicanos; Hispanic American Students; Latinas; Latinos; *University of California ABSTRACT This study sought to identify and analyze critical factors in a Hispanic student's decision to persist or drcy out at California state four-year institutions. In-depth telephone interviews with 151 Hispanic American students at five University of California campuses and seven California State University campuses were conducted. The interviews focused on the role of the Latino family, influence of peers, mentors, gender, finances, retention programs at target institutions, and campus climate. Findings included the following:(1) most of the students -

Appendix B GREEK GIVEN NAMES THEIR VARIATIONS, ENGLISH EQUIVALENTS and NAME DAYS
Appendix B GREEK GIVEN NAMES THEIR VARIATIONS, ENGLISH EQUIVALENTS AND NAME DAYS The names are in Greek alphabetical order. The letters M and F which precede each name indicate the gender, M for male and F for female. NOTE: An English equivalent may be used for more than one Greek name Given Name Variations English Celebrated Equivalent Name-day A F Αγγελική ................ Άγγελα, Κική, Κoύλα .............................................. ................................. 25 Mar Aggeliki .................. Aggela, Kiki, Koula ............................................... Angela M Άγγελoς .................. ................................................................................. ................................. 25 Mar Aggelos .................. ................................................................................. Angel F Αθαvασία ............... Αθαvασoύλα, Σoύλα, Θανάσω ................................ ................................. 18 Jan Athanasia ................ Athanasoula, Soula, Thanaso M Αθαvάσιoς .............. Θάvoς, Θαvάσης, Σάκης, Νάσoς ............................ ................................. 18 Jan Athanasios .............. Thanos, Thanasis, Sakis, Nasos ............................. Arthur F Αθηvά ..................... Ναvά, Νoύλα Athina ..................... Nana, Noula ............................................................ Athena F Αικατερίvη ............. Καίτη, Κατίvα, Κατερίvα, Κατίλω, Κατιvιώ ........... ................................. 25 Nov Aikaterini ............... Kaiti, -

The Ubiquitin Proteasome System Is Required for Cell Proliferation of The
RESEARCH ARTICLE 3257 Development 137, 3257-3268 (2010) doi:10.1242/dev.053124 © 2010. Published by The Company of Biologists Ltd The ubiquitin proteasome system is required for cell proliferation of the lens epithelium and for differentiation of lens fiber cells in zebrafish Fumiyasu Imai1, Asuka Yoshizawa1, Noriko Fujimori-Tonou2, Koichi Kawakami3 and Ichiro Masai1,* SUMMARY In the developing vertebrate lens, epithelial cells differentiate into fiber cells, which are elongated and flat in shape and form a multilayered lens fiber core. In this study, we identified the zebrafish volvox (vov) mutant, which shows defects in lens fiber differentiation. In the vov mutant, lens epithelial cells fail to proliferate properly. Furthermore, differentiating lens fiber cells do not fully elongate, and the shape and position of lens fiber nuclei are affected. We found that the vov mutant gene encodes Psmd6, the subunit of the 26S proteasome. The proteasome regulates diverse cellular functions by degrading polyubiquitylated proteins. Polyubiquitylated proteins accumulate in the vov mutant. Furthermore, polyubiquitylation is active in nuclei of differentiating lens fiber cells, suggesting roles of the proteasome in lens fiber differentiation. We found that an E3 ubiquitin ligase anaphase-promoting complex/cyclosome (APC/C) is involved in lens defects in the vov mutant. These data suggest that the ubiquitin proteasome system is required for cell proliferation of lens epithelium and for the differentiation of lens fiber cells in zebrafish. KEY WORDS: Ubiquitin, Proteasome, Lens, Zebrafish, Psmd6, APC/C INTRODUCTION acid DNase (DLAD; Dnase2b). However, it is unclear how lens During development, the lens placode delaminates from the morphogenesis and organelle loss are related to these transcription epidermal ectoderm and forms the lens vesicle. -

Full-Time and Part-Time Faculty List: November 2020
THE UNIVERSITY OF VERMONT FULL-TIME AND PART-TIME FACULTY LIST: NOVEMBER 2020 FULL-TIME AND PART-TIME FACULTY Adrianzen Herrera, Diego Assistant Professor (COM); Department LIST: NOVEMBER 2020 of Med-Hematology Oncology; MD; Cayetano Heredia University Agnarsson, Ingi Associate Professor; Department of Biology; PHD; Abaied, Jamie L.; Associate Professor; Department of Psychological George Washington Univ Science; PHD; Univ of IL Urbana-Champaign Agrawal, Varun Associate Professor (COM); Department of Med- Abajian, Michael John; Lecturer; Department of Nursing; MD; St. Nephrology; George's Univ Ahern, Thomas Patrick; Assistant Professor; Department of Surgery; Abbott, John D.; Lecturer I; Rubenstein Sch Env Nat Res; BA; PHD; Boston Univ Abdul-Karim, Yasmeen Assistant Professor (COM); Department of Ahmadi, Afshin Lecturer I; Grossman School of Business; JD; Boston Psychiatry; MD; New Jersey Medical Sch Rutgers Univ Abernathy, Karen E; Assistant Professor (COM); Department of Ahmed, Shahid Sattar; Assistant Professor (COM); Department of Med-Gen Internal Med; MD; Univ of Mississippi Med-Hematology Oncology; Abernathy, Mac Wilson; Assistant Professor (COM); Department of Aitken, Margaret S.; Clinical Assistant Prof.; Department of Nursing; Psychiatry; MD; Univ of Mississippi DNP; University of Vermont Abnet, Kevin R; Associate Professor (COM); Department of Aitken, Phil A.; Professor (COM); Department of Surg- Anesthesiology; MD; Harvard Medical School Ophthalmology; MD; Baylor Coll of Med Abu Alfa, Amer K; Assistant Professor (COM); Department -

Baby Girl Names | Registered in 2019
Vital Statistics Baby2019 BabyGirl GirlsNames Names | Registered in 2019 From:Jan 01, 2019 To: Dec 31, 2019 First Name Frequency First Name Frequency First Name Frequency Aadhini 1 Aarnavi 1 Aadhirai 1 Aaro 1 Aadhya 2 Aarohi 2 Aadila 1 Aarora 1 Aadison 1 Aarushi 1 Aadroop 1 Aarya 3 Aadya 3 Aarza 2 Aafiya 1 Aashvee 1 Aaghnya 1 Aasiya 1 Aahana 2 Aasiyah 2 Aaila 1 Aasmi 1 Aaira 3 Aasmine 1 Aaleena 1 Aatmja 1 Aalia 1 Aatri 1 Aaliah 1 Aayah 2 Aalis 1 Aayara 1 Aaliya 1 Aayat 1 Aaliyah 17 Aayla 1 Aaliyah-Lynn 1 Aayna 1 Aalya 1 Aayra 2 Aamina 1 Aazeen 1 Aamna 1 Abagail 1 Aanaya 1 Abbey 4 Aaniya 1 Abbi 1 Aaniyah 1 Abbie 1 Aanya 3 Abbiejean 1 Aara 1 Abbigail 3 Aaradhya 1 Abbiteal 1 Aaradya 1 Abby 10 Aaraya 1 Abbygail 1 Aaria 2 Abdirashid 1 Aariya 1 Abeeha 1 Aariyah 1 Aberlene 1 Aarna 3 Abhideep 1 Abi 1 Abiah 1 10 Jun 2020 1 Abiegail 02:22:21 PM1 Abigael 1 Abigail 141 Abigale 1 1 10 Jun 2020 2 02:22:21 PM Baby Girl Names | Registered in 2019 First Name Frequency First Name Frequency Abigayle 1 Addalyn 4 Abihail 1 Addalynn 1 Abilene 2 Addasyn 1 Abina 1 Addelyn 1 Abisha 2 Addi 1 Ablakat 1 Addie 2 Aboni 1 Addilyn 3 Abrahana 1 Addilynn 2 Abreen 1 Addison 61 Abrielle 2 Addisyn 2 Absalat 1 Addley 1 Abuk 2 Addy 1 Abyan 1 Addyson 2 Abygale 1 Adedoyin 1 Acadia 1 Adeeva 1 Acelynn 1 Adeifeoluwa 1 Achai 1 Adela 1 Achan 1 Adélaïde 1 Achol 1 Adelaide 20 Ackley 1 Adelaine 1 Ada 23 Adelayne 1 Adabpreet 1 Adele 4 Adaeze 1 Adèle 2 Adah 1 Adeleigha 1 Adair 1 Adeleine 1 Adalee 1 Adelheid 1 Adalena 1 Adelia 3 Adaley 1 Adelina 2 Adalina 2 Adeline 40 Adalind 1 Adella -

MOLECULAR ECOLOGY of MARINE ALGAL VIRUSES by JOAQUIN
University of Plymouth PEARL https://pearl.plymouth.ac.uk 04 University of Plymouth Research Theses 01 Research Theses Main Collection 2006 MOLECULAR ECOLOGY OF MARINE ALGAL VIRUSES MARTINEZ, JOAQUIN MARTINEZ http://hdl.handle.net/10026.1/2459 University of Plymouth All content in PEARL is protected by copyright law. Author manuscripts are made available in accordance with publisher policies. Please cite only the published version using the details provided on the item record or document. In the absence of an open licence (e.g. Creative Commons), permissions for further reuse of content should be sought from the publisher or author. MOLECULAR ECOLOGY OF MARINE ALGAL VIRUSES By JOAQUIN MARTINEZ MARTINEZ A thesis submitted to the University of Plymouth for the degree of DOCTOR OF PHILOSOPHY Department of Biological Sciences University of Plymouth In collaboration with The Marine Biological Association (UK) Plymouth Marine Laboratory (UK) University of Bergen (Norway) September 2006 ~~ University ofiPiymol!th · 1 ~ ll.ibrary; I . -- ~ · ~ltem,No 'C?!oO:I),'lC,SI Of+ _ ~.,l. Shelfmark . .. i T~E.'OIS SliJ' .. ~(Q£\.~. b$-. tl~ . - . • , I This copy of,therthesis hlis. been !;llpplied of\:cohditicmthat anyone who:consults it is :understood I to recognise thahts;.copyright rests with its author 1111<1 ,tllM r\6 quotation' from the thesi.sian<i i1o ifl[orniation,denvedl from. it may'oe publishedi without .the'author's prior consent. b " Joaquin Martinez Martinez Molecular Ecology of Marine Algal Viruses IAbstract In this study phytoplankton viruses were investigated from a point of view of their genotypic richness, ecology and role in controlling two microalgae species: Emiliania huxleyi and Phaeocystis pouchetii. -

The American Indian in the American Film
THE AMERICAN INDIAN IN THE AMERICAN FILM Thesis presented in partial fulfilment of the requirements for the degree of Master of Arts in American Studies in the University of Canterbury by Michael J. Brathwaite 1981 ABSTRACT This thesis is a chronological examination of the ways in which American Indians have been portrayed in American 1 f.ilms and the factors influencing these portrayals. B eginning with the literary precedents, the effects of three wars and other social upheavals and changes are considered. In addition t-0 being the first objective detailed examination of the subj�ct in English, it is the first work to cover the last decade. It concludes that because of psychological factors it is unlikely that film-makers are - capable of advancing far beyond the basic stereotypes, and that the failure of Indians to appreciate this has repeatedly caused ill-feeling between themselves and the film-makers, making the latter abandon their attempts at a fair treatment of the Indians. ii TABLE OF CONTENTS Preface iii Chapter I: The Background of the Problem c.1630 to c.1900. 1 Chapter II: The Birth of the Cinema and Its Aftermath: 1889 to 1939. 21 Chapter III: World War II and Its Effects: 1940 to 1955. 42 Chapter IV: Assimilation of Separatism?: 1953 to 1965. 65 Chapter V: The Accuracy Question. 80 Chapter VI: Catch-22: 1965 to 1972. 105 Chapter VII: Back to the Beginning: 1973 to 1981. 136 Chapter VIII: Conclusion. 153 Bibliography 156 iii PREFACE The aim of this the.sis is to examine the ways in which the American Indians have been portrayed in American films, the influences on their portrayals, and whether or not they have changed. -
The University of Vermont List of Base Pay November 2019
THE UNIVERSITY OF VERMONT BURLINGTON, VERMONT The University of Vermont List of Base Pay November 2019 Release Date: November 2019 University of Vermont List of Base Pay, November 2019 Name Primary Job Title Base Pay Abaied,Jamie L. Associate Professor $67,200 Abair,Shirley Sam Office/Prgm Support Generalist $28,219 Abajian,Michael John Lecturer $53,612 Abbott,Lori M. Office/Prgm Support Generalist $45,766 Abdallah,Rany Talal Assistant Professor (COM) $30,000 Abdul-Karim,Yasmeen Assistant Professor (COM) $30,000 Abernathy,Karen E Assistant Professor (COM) $30,000 Abernathy,Mac Wilson Assistant Professor (COM) $30,000 Abiti,Pearl D. Early Childhood Teaching Ast $29,981 Abnet,Kevin R Associate Professor (COM) $19,800 Aboushousha,Reem M Lab Research Technician $40,641 Abu Alfa,Amer K Assistant Professor (COM) $40,500 AbuJaish,Wasef Associate Professor (COM) $35,000 Achenbach,Thomas Max Professor $63,050 Ackil,Daniel J. Assistant Professor (COM) $35,000 Acostamadiedo,Jose Maria Clinical Prac Phys-CVPH (COM) $30,000 Acquisto,Joseph T. Professor $118,256 Adair,Elizabeth Carol Associate Professor $83,786 Adam,Michael Anthony Facilities Repairperson $39,229 Adam,Wilfred Carl Maintenance Unit Supervisor $47,840 Adamczak,Christina L Office/Prgm Support Generalist $37,541 Adams,Alec L Business Oprtns Administrator $104,699 Adams,Clifford D. Custodial Maintenance Spec Sr $37,128 Adams,Elizabeth Jean Clinical Professor $96,794 Adams,Jane Lydia Researcher/Analyst $67,426 Adams,Zoe S Research Specialist $47,198 Adamson,Christine S.C. Lab Research Technician $49,140 Aden,Lule O Student Srvcs Professional $33,000 Aden,Mumina Hassan Custodial Maintenance Worker $29,390 Adeniyi,Aderonke Oluponle Assistant Professor (COM) $51,610 Ades,Philip A. -

Gene Name Forward Primer Reverse Primer ACTB
Gene Name Forward Primer Reverse Primer ACTB CTGGAACGGTGAAGGTGACA AAGGGACTTCCTGTAACAATGCA ACVRL1 ACATGAAGAAGGTGGTGTGTGTGG CGGGCAGAGGGGTTTGGGTA ADAMDEC1 GGGGCCAGACTACACTGAAACATT ACCCGTCACAAGTACTGATGCTG AHI1 GTCCAAAACTACCCCATCAAGGCT GCAGCACAGGAACGTATCACCT ANGPT2 TGGCAGCGTTGATTTTCAGAGG GCGAAACAAACTCATTTCCCAGCC ANPEP TGAAGAAGCAGGTCACACCCCT AACTCCGTTGGAGCAGGCGG APOA1 GCCGTGCTCTTCCTGACGG TGGGACACATAGTCTCTGCCGC ATXN7 CACCGCCCACTCTGGAAAAGAA GGGTGCAGGGCTTCTTGGTG B2M TGCTGTCTCCATGTTTGATGTATCT TCTCTGCTCCCCACCTCTAAGT BAG4 AGGTTCCAGGATATCCGCCTT TCGGTCCTGATTGTGGAACACT BCL2 ACAACATCGCCCTGTGGATGA CCGTACAGTTCCACAAAGGCAT BCL2L14 GCTCAGGGTCAAAGGACGTTGG TCAGCTACTCGGTTGGCAATGG BCL7A GAACCATGTCGGGCAGGTCG CCCATTTGTAGATTCGTAGGGATGTGT BIN1 TGCTGTCGTGGTGGAGACCTTC GCCGTGTAGTCGTGCTGGG BIRC3 TGCTATCCACATCAGACAGCCC TCTGAATGGTCTTCTCCAGGTTCA BIRC5 TTCTCAAGGACCACCGCATCT AGTGGATGAAGCCAGCCTCG BLK TCGGGGTCTTCACCATCAAAGC GCGCTCCAGGTTGCGGATGA BTRC CCAAATGTGTCATTACCAACATGGGC GCAGCACATAGTGATTTGGCATCC BUB3 CGGAACATGGGTTACGTGCAGC CCAAATACTCAACTGCCACTCGGC CAGE1 TCCAAAATGCACAGTCTTCTGGCT GGAGGCTCTTCAGTTTTTGCAGC CASP1 CCTGTTCCTGTGATGTGGAGGAAA GCTCTACCATCTGGCTGCTCAA CASP3 AGCGAATCAATGGACTCTGGAATATCC GTTTGCTGCATCGACATCTGTACCA CCL5 TCATTGCTACTGCCCTCTGCG ACTGCTGGGTTGGAGCACTTG CCL18 CCCTCCTTGTCCTCGTCTGCA GCACTGGGGGCTGGTTTCAG CCL26 TTCCAATACAGCCACAAGCCCC GGATGGGTACAGACTTTCTTGCCTC CCND2 TCAAGTGCGTGCAGAAGGACAT CTTCGCACTTCTGTTCCTCACA CCND3 TGGCTGCTGTGATTGCACATGA GATGGCGGGTACATGGCAAAGG CCR3 ACGCTGCTCTGCTTCCTGG TCCTCAGTTCCCCACCATCGC CCR4 AGCATCGTGCTTCCTGAGCAA GGTGTCTGCTATATCCGTGGGGT CCR7 AGACAGGGGTAGTGCGAGGC -
![Myelogenous Leukemia 8;21 Translocation: Evidence That C-Mos Is Not Translocated [Somatic Cell Hybrids/C-Myc/Gene Mapping/Superoxide Dismutase (Soluble)] HARRY A](https://docslib.b-cdn.net/cover/6910/myelogenous-leukemia-8-21-translocation-evidence-that-c-mos-is-not-translocated-somatic-cell-hybrids-c-myc-gene-mapping-superoxide-dismutase-soluble-harry-a-2176910.webp)
Myelogenous Leukemia 8;21 Translocation: Evidence That C-Mos Is Not Translocated [Somatic Cell Hybrids/C-Myc/Gene Mapping/Superoxide Dismutase (Soluble)] HARRY A
Proc. Natl. Acad. Sci. USA Vol. 82, pp. 464-468, January 1985 Genetics Isolation and analysis of the 21q+ chromosome in the acute myelogenous leukemia 8;21 translocation: Evidence that c-mos is not translocated [somatic cell hybrids/c-myc/gene mapping/superoxide dismutase (soluble)] HARRY A. DRABKIN*t, MANUEL DIAZt, CYNTHIA M. BRADLEY*, MICHELLE M. LE BEAUS, JANET D. ROWLEYt, AND DAVID PATTERSON*§¶ *The Eleanor Roosevelt Institute for Cancer Research, 4200 East Ninth Avenue, B-129, and tThe Division of Medical Oncology and Departments of Medicine and ¶Biochemistry, Biophysics and Genetics, University of Colorado Health Sciences Center, 4200 East Ninth Avenue, Denver, CO 80262; and tSection of Hematology-Oncology, Department of Medicine, Pritzker School of Medicine, The University of Chicago, Chicago, IL 60637 Contributed by Janet D. Rowley, September 4, 1984 ABSTRACT Acute myelogenous leukemia (AML), sub- light chain genes are translocated to the 3' region of c-myc group M2, is associated with a nonrandom chromosomal (4-7). translocation, t(8;21)(q22,q22). The oncogene c-mos also has Somatic cell genetic approaches have been used also to been localized to the q22 band on chromosome 8. There is also show that, in Philadelphia (Ph')-positive chronic myeloge- evidence that genes on chromosome 21 may be important in nous leukemia, c-abl oncogene sequences are translocated the development of leukemia. To determine whether the c-mos from chromosome 9 to the Ph' (22q-) chromosome (8). oncogene has been translocated in AML-M2 with this translo- Analysis of cells from two Ph'-positive patients has revealed cation and to isolate DNA sequences and genes from these two that the breakpoint in chromosome 9 is near c-abl (9).