Research Monograph Series
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Opioids): SOR/2018-77 Canada Gazette, Part II, Volume 152, Number 9
Canada Gazette, Part 2, Volume 152, Number 9: Regulations Amendin... http://gazette.gc.ca/rp-pr/p2/2018/2018-05-02/html/sor-dors77-eng.html Home (http://www.canada.ca/en/index.html) How government works (http://www.canada.ca/en/government/system/index.html) Treaties, laws and regulations (https://www.canada.ca/en/government/system/laws.html) Canada Gazette (/accueil-home-eng.html) Publications (/rp-pr/publications-eng.html) Part II: Vol. 152 (2018) (/rp-pr/p2/2018/index-eng.html) May 2, 2018 (/rp-pr/p2/2018/2018-05-02/html/index-eng.html) Regulations Amending the Food and Drug Regulations (Opioids): SOR/2018-77 Canada Gazette, Part II, Volume 152, Number 9 Registration April 23, 2018 FOOD AND DRUGS ACT P.C. 2018-429 April 20, 2018 Her Excellency the Governor General in Council, on the recommendation of the Minister of Health, pursuant to section 30a of the Food and Drugs Act b, makes the annexed Regulations Amending the Food and Drug Regulations (Opioids). Regulations Amending the Food and Drug Regulations (Opioids) Amendments 1 Subsections C.01.005(2) and (3) of the Food and Drug Regulations 1 are replaced by the following: (2) Subsection (1) does not apply to (a) a drug in dosage form that is compounded by a pharmacist under a prescription or by a practitioner; or (b) a drug in dosage form that is sold under a prescription if the following information appears on the drug’s label: (i) the drug’s proper name, common name or brand name, (ii) the drug’s potency, and (iii) the name of the drug’s manufacturer. -

Drug Threshold Enactments (2009-2015) 2015
NCSL: Drug Threshold Enactments 2009-2015 Page | 1 Drug Threshold Enactments (2009-2015) 2015 Alabama SB 67 Lowers from a class C to class D felony first degree possession of marijuana if the person possesses marijuana for personal use after previously being convicted of certain marijuana possession offenses. Connecticut HB 7104 Reduces from a felony to a class A misdemeanor possession of any amount of illegal drug. Reduces from a felony to a class A misdemeanor possession of a half-ounce or more of marijuana. Kentucky SB 192 Creates a new class C felony of importing heroin and a new class B felony of aggravated trafficking in a controlled substance in the first degree if the substance trafficked was 100 grams or more of heroin. Increases the penalty from a class A misdemeanor to a class D felony for drug trafficking that involves more than 120 dosage units. Louisiana HB 149 Creates graduated penalties for first time possession of marijuana offenses by weight, reduces penalties for second and third convictions for possession of marijuana offenses, and creates a penalty for fourth conviction of possession of marijuana. • First offense possession of less than 14 grams of marijuana is punishable by not more than 15 days in jail and not more than $300. • First offense possession of more than 14 grams but less than two and a half pounds of marijuana is punishable by not more than six months jail and not more than $500. • Reduces second offense possession of marijuana from not more than 5 years and not less than $250 but not more than $2,000, to not more than 6 months in jail and nor more than $1,000. -

Palliative Care Case of the Month
PALLIATIVE CARE CASE OF THE MONTH “Treating Non-Infectious Diarrhea” by Robert Arnold, MD Volume 19, No. 98 August, 2019 Case 1: Mr. Jones is a 58-year-old man with short gut Three drugs are used because of their ability to slow down the syndrome. Palliative Care was consulted for goals of care, gut, allowing for more time for absorption of intestinal fluids a however quickly it became clear uncontrolled diarrhea was a decrease of diarrhea. The most well-know is loperamide, a larger priority. He said having to change the bag every few hours synthetic opiate which has minimal absorption. The dosing is 4 completely interfered with his living a normal life. He said, “I’d mg after one’s first bowel movement and then 2 mg after every rather die than have all of this diarrhea.” unformed stool, up to 16 mg (in palliative care patients there is some data for use up to 54 mg).9, 10 Loperamide should be Case 2: A 62-year-old woman with non-small cell lung cancer continued for 12 hours after diarrhea is stopped. Adverse effects is receiving immunotherapy. She has done quite well but is include mostly constipation, abdominal cramps, nausea and distressed by her diarrhea. She tried Lomotil and Imodium but rarely CNS effects like fatigue or dizziness. Cases of torsades de neither worked. When seeing her palliative care doctor, she said, pointes and death have been reported with higher than “It isn’t worth treating my cancer if I can’t live a normal life.” 9 recommended doses. -
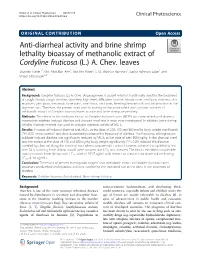
Anti-Diarrheal Activity and Brine Shrimp Lethality Bioassay of Methanolic Extract of Cordyline Fruticosa (L.) A
Naher et al. Clinical Phytoscience (2019) 5:15 https://doi.org/10.1186/s40816-019-0109-z ORIGINAL CONTRIBUTION Open Access Anti-diarrheal activity and brine shrimp lethality bioassay of methanolic extract of Cordyline fruticosa (L.) A. Chev. leaves Sharmin Naher1*, Md. Abdullah Aziz1, Mst. Irin Akter2, S. M. Mushiur Rahman1, Sadiur Rahman Sajon1 and Kishor Mazumder1,3 Abstract Background: Cordyline fruticosa (L.) A. Chev. (Asparagaceae) is a plant which is traditionally used for the treatment of cough, bloody cough, diarrhea, dysentery, high fever, difficulties in urine, bloody urine, small pox, madness, skin eruptions, joint pains, rheumatic bone pains, sore throat, neck pain, bleeding hemorrhoids and inflammation in the digestive tract. Therefore, the present work aims to investigate the antidiarrheal and cytotoxic activities of methanolic extract of Cordyline fruticosa leaves in mice and brine shrimp, respectively. Methods: The effects of the methanol extract of Cordyline fruticosa leaves (MCFL) on castor oil-induced diarrhea, magnesium sulphate induced diarrhea and charcoal meal test in mice were investigated. In addition, brine shrimp lethality bioassay method was used to evaluate cytotoxic activity of MCFL. Results: In castor oil induced diarrheal test, MCFL at the dose of 200, 400 and 800 mg/kg body weight significantly (∗P< 0.05, versus control) and dose-dependently reduced the frequency of diarrhea. The frequency of magnesium sulphate-induced diarrhea was significantly reduced by MCFL at the dose of with 800 mg/kg. In the charcoal meal test, the extract at the dose of 400 and 800 mg/kg body weight significantly (∗P< 0.05) reduced the distance travelled by charcoal along the intestinal tract when compare with control. -

Oklahoma Drug Threat Assessment
2018 Oklahoma Drug Threat Assessment Oklahoma Bureau of Narcotics and Dangerous Drugs i John Scully, Director MARY FALLIN JOHN SCULLY Governor Director September 12, 2018 The Oklahoma Bureau of Narcotics has served the citizens of Oklahoma in the quest for a drug- free state since 1975. Our agency remains committed to working with lawmakers, law enforcement, public health officials, and the citizens of Oklahoma to develop comprehensive strategies to address drug abuse in communities across the state. While we know many factors contribute to drug abuse, OBN is committed to reducing the availability of illegal drugs in Oklahoma. Our agency works to eradicate illegal drugs in Oklahoma by enforcing drug laws, administering statewide programs, and providing continual outreach to our stakeholders – lawmakers, law enforcement, public health officials, and the citizens of Oklahoma. OBN agents enforce drug laws by utilizing aggressive investigative methods and administering statewide drug diversion programs. The Prescription Drug Monitoring Program is a valuable tool for practitioners, pharmacists, and law enforcement in the prevention and detection of the diversion and abuse of pharmaceutical controlled substances. As a service to our communities, OBN also administers the Safe Trips for Scripts Drug Prevention Program. This program provides citizens a safe way to discard unwanted medications by disposing of them in one of our 177 take back boxes located around the state. This drug threat assessment was created to help provide officials and citizens with helpful information about drug threats across our state. We will continue to collaborate with other agencies and the citizens to work toward a safer and healthier Oklahoma. -

Information to Users
The direct and modulatory antinociceptive actions of endogenous and exogenous opioid delta agonists Item Type text; Dissertation-Reproduction (electronic) Authors Vanderah, Todd William. Publisher The University of Arizona. Rights Copyright © is held by the author. Digital access to this material is made possible by the University Libraries, University of Arizona. Further transmission, reproduction or presentation (such as public display or performance) of protected items is prohibited except with permission of the author. Download date 04/10/2021 00:14:57 Link to Item http://hdl.handle.net/10150/187190 INFORMATION TO USERS This ~uscript }las been reproduced from the microfilm master. UMI films the text directly from the original or copy submitted. Thus, some thesis and dissertation copies are in typewriter face, while others may be from any type of computer printer. The quality of this reproduction is dependent upon the quality of the copy submitted. Broken or indistinct print, colored or poor quality illustrations and photographs, print bleedthrough, substandard margins, and improper alignment can adversely affect reproduction. In the unlikely. event that the author did not send UMI a complete mannscript and there are missing pages, these will be noted Also, if unauthorized copyright material had to be removed, a note will indicate the deletion. Oversize materials (e.g., maps, drawings, charts) are reproduced by sectioning the original, beginnjng at the upper left-hand comer and contimJing from left to right in equal sections with small overlaps. Each original is also photographed in one exposure and is included in reduced form at the back of the book. Photographs included in the original manuscript have been reproduced xerographically in this copy. -

Pharmacy and Poisons (Third and Fourth Schedule Amendment) Order 2017
Q UO N T FA R U T A F E BERMUDA PHARMACY AND POISONS (THIRD AND FOURTH SCHEDULE AMENDMENT) ORDER 2017 BR 111 / 2017 The Minister responsible for health, in exercise of the power conferred by section 48A(1) of the Pharmacy and Poisons Act 1979, makes the following Order: Citation 1 This Order may be cited as the Pharmacy and Poisons (Third and Fourth Schedule Amendment) Order 2017. Repeals and replaces the Third and Fourth Schedule of the Pharmacy and Poisons Act 1979 2 The Third and Fourth Schedules to the Pharmacy and Poisons Act 1979 are repealed and replaced with— “THIRD SCHEDULE (Sections 25(6); 27(1))) DRUGS OBTAINABLE ONLY ON PRESCRIPTION EXCEPT WHERE SPECIFIED IN THE FOURTH SCHEDULE (PART I AND PART II) Note: The following annotations used in this Schedule have the following meanings: md (maximum dose) i.e. the maximum quantity of the substance contained in the amount of a medicinal product which is recommended to be taken or administered at any one time. 1 PHARMACY AND POISONS (THIRD AND FOURTH SCHEDULE AMENDMENT) ORDER 2017 mdd (maximum daily dose) i.e. the maximum quantity of the substance that is contained in the amount of a medicinal product which is recommended to be taken or administered in any period of 24 hours. mg milligram ms (maximum strength) i.e. either or, if so specified, both of the following: (a) the maximum quantity of the substance by weight or volume that is contained in the dosage unit of a medicinal product; or (b) the maximum percentage of the substance contained in a medicinal product calculated in terms of w/w, w/v, v/w, or v/v, as appropriate. -

Opioid Receptorsreceptors
OPIOIDOPIOID RECEPTORSRECEPTORS defined or “classical” types of opioid receptor µ,dk and . Alistair Corbett, Sandy McKnight and Graeme Genes encoding for these receptors have been cloned.5, Henderson 6,7,8 More recently, cDNA encoding an “orphan” receptor Dr Alistair Corbett is Lecturer in the School of was identified which has a high degree of homology to Biological and Biomedical Sciences, Glasgow the “classical” opioid receptors; on structural grounds Caledonian University, Cowcaddens Road, this receptor is an opioid receptor and has been named Glasgow G4 0BA, UK. ORL (opioid receptor-like).9 As would be predicted from 1 Dr Sandy McKnight is Associate Director, Parke- their known abilities to couple through pertussis toxin- Davis Neuroscience Research Centre, sensitive G-proteins, all of the cloned opioid receptors Cambridge University Forvie Site, Robinson possess the same general structure of an extracellular Way, Cambridge CB2 2QB, UK. N-terminal region, seven transmembrane domains and Professor Graeme Henderson is Professor of intracellular C-terminal tail structure. There is Pharmacology and Head of Department, pharmacological evidence for subtypes of each Department of Pharmacology, School of Medical receptor and other types of novel, less well- Sciences, University of Bristol, University Walk, characterised opioid receptors,eliz , , , , have also been Bristol BS8 1TD, UK. postulated. Thes -receptor, however, is no longer regarded as an opioid receptor. Introduction Receptor Subtypes Preparations of the opium poppy papaver somniferum m-Receptor subtypes have been used for many hundreds of years to relieve The MOR-1 gene, encoding for one form of them - pain. In 1803, Sertürner isolated a crystalline sample of receptor, shows approximately 50-70% homology to the main constituent alkaloid, morphine, which was later shown to be almost entirely responsible for the the genes encoding for thedk -(DOR-1), -(KOR-1) and orphan (ORL ) receptors. -

Overland Park, Kansas Municipal Code Table of Contents Title 1 - General Provisions 1.01 Code Adoption
Overland Park, Kansas Municipal Code Table Of Contents Title 1 - General Provisions 1.01 Code Adoption. 1.01.010 Generally. 1.01.020 Publication-Effect. 1.01.030 Short Title-Citation-Reference. 1.01.040 Reference Applies to Amendments. 1.01.050 Title, Chapter and Section Headings. 1.01.060 Reference to Specific Ordinances. 1.01.070 Supplements Authorized. 1.01.080 Effect of Code on Past Actions and Obligations. 1.01.090 Effective Date of Code. 1.01.100 Ordinance Book Designated. 1.01.110 Constitutionality. 1.04 General Provisions 1.04.010 Definitions. 1.04.020 Grammatical Interpretation. 1.04.030 Prohibited Acts Include Causing, Permitting, and Related Acts. 1.04.040 Construction. 1.04.050 Repeal Not To Revive Any Ordinances. 1.08 Right of Entry for Inspection 1.08.010 Regulations Generally. 1.12 General Penalty 1.12.010 Designated. 1.16 Ward Boundaries (Repealed) 1.16.010 Division - Boundaries - Renumbering - Boundary Adjustment. 1.20 Official Newspaper (Repealed) 1.20.010 Exemption from K.S.A. 13-1420. 1.20.020 Governing Body to Designate Official Newspaper. 1.20.030 Official Designation. 1.20.040 Official Newspaper To Have Been Published for a Year. 1.20.050 More Than One Official Newspaper. 1.24 Citations for Violations 1.24.010 Definitions. 1.24.020 Notice To Appear. 1.24.030 Time Specified. 1.24.040 Municipal Court. 1.24.050 Distribution of Notice. 1.24.060 Complaint To Be Filed. 1.24.070 Chapter Inapplicable To Certain Violations. Legal Basis for Overland Park, Kansas Title 2 - Administration and Personnel Page 1 2.09 City Manager/Governing Body Article I. -

3.2.2 Opioids and Abuse, Misuse and Dependence
Opioids and abuse, misuse and dependence CONFIDENTIAL Medicines Adverse Reactions Committee Meeting date 3/12/2020 Agenda item 3.2.2 Title Opioids and abuse, misuse and dependence Submitted by Medsafe Pharmacovigilance Paper type For advice Team Active ingredient Product name Sponsor Buprenorphine Codeine Dihydrocodeine Fentanyl See Annex 1 for the full list of opioids approved in New Zealand Methadone Morphine Oxycodone Pethidine Tramadol PHARMAC funding All opioids in Annex 1 have at least one product funded on the Hospital and Community Schedules. Previous MARC 169th meeting – held 9 March 2017: Concomitant use of opioids, benzodiazepines meetings and other CNS depressants and the risk of serious side effects International action • FDA - Risk Evaluation and Mitigation Strategy (REMS) required for all opioids; prescribing information updates • MHRA – warnings on package labelling, updates to prescribing information, safety leaflets for patients • TGA – smaller pack sizes, boxed warnings and class statements in prescribing information and consumer medicine information, indication review • Health Canada – Mandatory risk management plans for prescription opioids, Warning sticker and patient information handout Prescriber Update The following is a list of recent articles only. • Spotlight on tramadol including updated advice for use in children June 2020 • Spotlight on Codeine June 2018 • Medicines Interacting with Methadone June 2018 • Transdermal Opioid Patches - Stick to the Correct Application March 2020 Classification See Annex 1. Medicines -

Needle Sharing Among Intravenous Drug Abusers: National and International Perspectives
Needle Sharing Among Intravenous Drug Abusers: National and International Perspectives U. S. DEPARTMENT OF HEALTH AND HUMAN SERVICES • Public Health Service • Alcohol, Drug Abuse, and Mental Health Administration Needle Sharing Among Intravenous Drug Abusers: National and International Perspectives Editors: Robert J. Battjes, D.S.W. Roy W. Pickens, Ph.D. Division of Clinical Research National Institute on Drug Abuse NIDA Research Monograph 80 1988 U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Public Health Service Alcohol, Drug Abuse, and Mental Health Administration National Institute on Drug Abuse 5600 Fishers Lane Rockville, MD 20857 For sale by the Superintendent of Documents, U.S. Government Printing Office Washington, DC 20402 NIDA Research Monographs are prepared by the research divisions of the National Institute on Drug Abuse and published by its Office of Science. The primary objective of the series is to provide critical reviews of research problem areas and techniques, the content of state-of-the-art conferences, and integrative research reviews. Its dual publication emphasis is rapid and targeted dissemination to the scientific and professional community. Editorial Advisors MARTIN W. ADLER, Ph.D. MARY L. JACOBSON Temple University School of Medrcrne National Federation of Parents for Philadelphia. Pennsylvania Drug-Free Youth Omaha, Nebraska SYDNEY ARCHER, Ph.D. Rensselaer Polytechnic Institute Troy, New York REESE T. JONES, M.D. Langley Porter Neuropsychiatric lnstitute RICHARD E. BELLEVILLE. Ph.D. San Francisco, California NB Associates, Health Sciences RockviIle, Maryland DENISE KANDEL, Ph.D. KARST J. BESTEMAN College of Physicians and Surgeons of Alcohol and Drug Problems Association Columbia University of North America New York, New York Washington, D. -
Texas Controlled Substances Act
HEALTH AND SAFETY CODE TITLE 6. FOOD, DRUGS, ALCOHOL, AND HAZARDOUS SUBSTANCES SUBTITLE C. SUBSTANCE ABUSE REGULATION AND CRIMES CHAPTER 481. TEXAS CONTROLLED SUBSTANCES ACT SUBCHAPTER A. GENERAL PROVISIONS Sec.A481.001.AASHORT TITLE. This chapter may be cited as the Texas Controlled Substances Act. Acts 1989, 71st Leg., ch. 678, Sec. 1, eff. Sept. 1, 1989. Sec.A481.002.AADEFINITIONS. In this chapter: (1)AA"Administer" means to directly apply a controlled substance by injection, inhalation, ingestion, or other means to the body of a patient or research subject by: (A)AAa practitioner or an agent of the practitioner in the presence of the practitioner; or (B)AAthe patient or research subject at the direction and in the presence of a practitioner. (2)AA"Agent" means an authorized person who acts on behalf of or at the direction of a manufacturer, distributor, or dispenser. The term does not include a common or contract carrier, public warehouseman, or employee of a carrier or warehouseman acting in the usual and lawful course of employment. (3)AA"Commissioner" means the commissioner of state health services or the commissioner 's designee. (4)AA"Controlled premises" means: (A)AAa place where original or other records or documents required under this chapter are kept or are required to be kept; or (B)AAa place, including a factory, warehouse, other establishment, or conveyance, where a person registered under this chapter may lawfully hold, manufacture, distribute, dispense, administer, possess, or otherwise dispose of a controlled substance or other item governed by the federal Controlled Substances Act (21 U.S.C.