(M) of SARS-Cov-2
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Clinical Utility Gene Card For: 3-M Syndrome – Update 2013
European Journal of Human Genetics (2014) 22, doi:10.1038/ejhg.2013.156 & 2014 Macmillan Publishers Limited All rights reserved 1018-4813/14 www.nature.com/ejhg CLINICAL UTILITY GENE CARD UPDATE Clinical utility gene card for: 3-M syndrome – Update 2013 Muriel Holder-Espinasse*,1, Melita Irving1 and Vale´rie Cormier-Daire2 European Journal of Human Genetics (2014) 22, doi:10.1038/ejhg.2013.156; published online 31 July 2013 Update to: European Journal of Human Genetics (2011) 19, doi:10.1038/ejhg.2011.32; published online 2 March 2011 1. DISEASE CHARACTERISTICS nonsense and missense mutations c.4333C4T (p.Arg1445*) and 1.1 Name of the disease (synonyms) c.4391A4C (p.His1464Pro), respectively, render CUL7 deficient 3-M syndrome (gloomy face syndrome, dolichospondylic dysplasia). in recruiting ROC1, leading to impaired ubiquitination. OBSL1: microsatellites analysis of the locus (2q35-36.1) in con- 1.2 OMIM# of the disease sanguineous families. OBSL1: microsatellites analysis of the locus 273750. (2q35-36.1) in consanguineous families. Mutations induce non- sense mediated decay. Knockdown of OBSL1 in HEK293 cells 1.3 Name of the analysed genes or DNA/chromosome segments shows the role of this gene in the maintenance of normal levels of CUL7, OBSL1 and CCDC8.1–5 CUL7. Abnormal IGFBP2 andIGFBP5 mRNA levels in two patients with OBSL1 mutations, suggesting that OBSL1 modulates the 1.4 OMIM# of the gene(s) expression of IGFBP proteins. CCDC8: microsatellites analysis 609577 (CUL7), 610991 (OBSL1) and 614145 (CCDC8). at the locus (19q13.2-q13.32). CCDC8, 1-BP DUP, 612G and CCDC8, 1-BP. -

Whole-Genome Microarray Detects Deletions and Loss of Heterozygosity of Chromosome 3 Occurring Exclusively in Metastasizing Uveal Melanoma
Anatomy and Pathology Whole-Genome Microarray Detects Deletions and Loss of Heterozygosity of Chromosome 3 Occurring Exclusively in Metastasizing Uveal Melanoma Sarah L. Lake,1 Sarah E. Coupland,1 Azzam F. G. Taktak,2 and Bertil E. Damato3 PURPOSE. To detect deletions and loss of heterozygosity of disease is fatal in 92% of patients within 2 years of diagnosis. chromosome 3 in a rare subset of fatal, disomy 3 uveal mela- Clinical and histopathologic risk factors for UM metastasis noma (UM), undetectable by fluorescence in situ hybridization include large basal tumor diameter (LBD), ciliary body involve- (FISH). ment, epithelioid cytomorphology, extracellular matrix peri- ϩ ETHODS odic acid-Schiff-positive (PAS ) loops, and high mitotic M . Multiplex ligation-dependent probe amplification 3,4 5 (MLPA) with the P027 UM assay was performed on formalin- count. Prescher et al. showed that a nonrandom genetic fixed, paraffin-embedded (FFPE) whole tumor sections from 19 change, monosomy 3, correlates strongly with metastatic death, and the correlation has since been confirmed by several disomy 3 metastasizing UMs. Whole-genome microarray analy- 3,6–10 ses using a single-nucleotide polymorphism microarray (aSNP) groups. Consequently, fluorescence in situ hybridization were performed on frozen tissue samples from four fatal dis- (FISH) detection of chromosome 3 using a centromeric probe omy 3 metastasizing UMs and three disomy 3 tumors with Ͼ5 became routine practice for UM prognostication; however, 5% years’ metastasis-free survival. to 20% of disomy 3 UM patients unexpectedly develop metas- tases.11 Attempts have therefore been made to identify the RESULTS. Two metastasizing UMs that had been classified as minimal region(s) of deletion on chromosome 3.12–15 Despite disomy 3 by FISH analysis of a small tumor sample were found these studies, little progress has been made in defining the key on MLPA analysis to show monosomy 3. -
(HPG) Axis Published: 18 April 2017 Matthew D
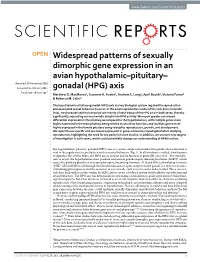
www.nature.com/scientificreports OPEN Widespread patterns of sexually dimorphic gene expression in an avian hypothalamic–pituitary– Received: 30 November 2016 Accepted: 16 February 2017 gonadal (HPG) axis Published: 18 April 2017 Matthew D. MacManes1, Suzanne H. Austin2, Andrew S. Lang1, April Booth2, Victoria Farrar2 & Rebecca M. Calisi2 The hypothalamic-pituitary-gonadal (HPG) axis is a key biological system required for reproduction and associated sexual behaviors to occur. In the avian reproductive model of the rock dove (Columba livia), we characterized the transcript community of each tissue of the HPG axis in both sexes, thereby significantly expanding our mechanistic insight into HPG activity. We report greater sex-biased differential expression in the pituitary as compared to the hypothalamus, with multiple genes more highly expressed in the male pituitary being related to secretory function, and multiple genes more highly expressed in the female pituitary being related to reproduction, growth, and development. We report tissue-specific and sex-biased expression in genes commonly investigated when studying reproduction, highlighting the need for sex parity in future studies. In addition, we uncover new targets of investigation in both sexes, which could potentially change our understanding of HPG function. The hypothalamic-pituitary-gonadal (HPG) axis is a system comprised of endocrine glands whose function is vital to the regulation of reproduction and associated behaviors (Fig. 1). In all vertebrates studied, from humans to Agnatha, the jawless fishes, the HPG axis is present and its function is generally conserved1. For reproduc- tion to occur, the hypothalamus must produce and secrete gonadotropin-releasing hormone (GnRH), which causes the pituitary gland to secrete gonadotropins, luteinizing hormone (LH) and follicle stimulating hormone (FSH)2. -

Identification and Validation of Methylation-Driven Genes Prognostic Signature for Recurrence of Laryngeal Squamous Cell Carcino
Cui et al. Cancer Cell Int (2020) 20:472 https://doi.org/10.1186/s12935-020-01567-3 Cancer Cell International PRIMARY RESEARCH Open Access Identifcation and validation of methylation-driven genes prognostic signature for recurrence of laryngeal squamous cell carcinoma by integrated bioinformatics analysis Jie Cui3†, Liping Wang2†, Waisheng Zhong4†, Zhen Chen5, Jie Chen4*, Hong Yang3* and Genglong Liu1* Abstract Background: Recurrence remains a major obstacle to long-term survival of laryngeal squamous cell carcinoma (LSCC). We conducted a genome-wide integrated analysis of methylation and the transcriptome to establish methyla- tion-driven genes prognostic signature (MDGPS) to precisely predict recurrence probability and optimize therapeutic strategies for LSCC. Methods: LSCC DNA methylation datasets and RNA sequencing (RNA-seq) dataset were acquired from the Cancer Genome Atlas (TCGA). MethylMix was applied to detect DNA methylation-driven genes (MDGs). By univariate and multivariate Cox regression analyses, fve genes of DNA MDGs was developed a recurrence-free survival (RFS)-related MDGPS. The predictive accuracy and clinical value of the MDGPS were evaluated by receiver operating characteristic (ROC) and decision curve analysis (DCA), and compared with TNM stage system. Additionally, prognostic value of MDGPS was validated by external Gene Expression Omnibus (GEO) database. According to 5 MDGs, the candidate small molecules for LSCC were screen out by the CMap database. To strengthen the bioinformatics analysis results, 30 pairs of clinical samples were evaluated by digoxigenin-labeled chromogenic in situ hybridization (CISH). Results: A total of 88 DNA MDGs were identifed, and fve RFS-related MDGs (LINC01354, CCDC8, PHYHD1, MAGEB2 and ZNF732) were chosen to construct a MDGPS. -

A Computational Approach for Defining a Signature of Β-Cell Golgi Stress in Diabetes Mellitus
Page 1 of 781 Diabetes A Computational Approach for Defining a Signature of β-Cell Golgi Stress in Diabetes Mellitus Robert N. Bone1,6,7, Olufunmilola Oyebamiji2, Sayali Talware2, Sharmila Selvaraj2, Preethi Krishnan3,6, Farooq Syed1,6,7, Huanmei Wu2, Carmella Evans-Molina 1,3,4,5,6,7,8* Departments of 1Pediatrics, 3Medicine, 4Anatomy, Cell Biology & Physiology, 5Biochemistry & Molecular Biology, the 6Center for Diabetes & Metabolic Diseases, and the 7Herman B. Wells Center for Pediatric Research, Indiana University School of Medicine, Indianapolis, IN 46202; 2Department of BioHealth Informatics, Indiana University-Purdue University Indianapolis, Indianapolis, IN, 46202; 8Roudebush VA Medical Center, Indianapolis, IN 46202. *Corresponding Author(s): Carmella Evans-Molina, MD, PhD ([email protected]) Indiana University School of Medicine, 635 Barnhill Drive, MS 2031A, Indianapolis, IN 46202, Telephone: (317) 274-4145, Fax (317) 274-4107 Running Title: Golgi Stress Response in Diabetes Word Count: 4358 Number of Figures: 6 Keywords: Golgi apparatus stress, Islets, β cell, Type 1 diabetes, Type 2 diabetes 1 Diabetes Publish Ahead of Print, published online August 20, 2020 Diabetes Page 2 of 781 ABSTRACT The Golgi apparatus (GA) is an important site of insulin processing and granule maturation, but whether GA organelle dysfunction and GA stress are present in the diabetic β-cell has not been tested. We utilized an informatics-based approach to develop a transcriptional signature of β-cell GA stress using existing RNA sequencing and microarray datasets generated using human islets from donors with diabetes and islets where type 1(T1D) and type 2 diabetes (T2D) had been modeled ex vivo. To narrow our results to GA-specific genes, we applied a filter set of 1,030 genes accepted as GA associated. -

I4X-JE-JFCM an Open-Label, Multicenter, Phase 1B/2 Study To
Protocol (e) I4X-JE-JFCM An Open-label, Multicenter, Phase 1b/2 Study to Evaluate Necitumumab in Combination with Gemcitabine and Cisplatin in the First-Line Treatment of Patients with Advanced (Stage IV) Squamous Non-Small Cell Lung Cancer (NSCLC) NCT01763788 Approval Date: 12-Jun-2016 I4X-JE-JFCM(e) Clinical Protocol Page 1 1. Protocol I4X-JE-JFCM(e) An Open-label, Multicenter, Phase 1b/2 Study to Evaluate Necitumumab in Combination with Gemcitabine and Cisplatin in the First-Line Treatment of Patients with Advanced (Stage IV) Squamous Non-Small Cell Lung Cancer (NSCLC) Confidential Information The information contained in this protocol is confidential and is intended for the use of clinical investigators. It is the property of Eli Lilly and Company or its subsidiaries and should not be copied by or distributed to persons not involved in the clinical investigation of Necitumumab (IMC-11F8; LY3012211), unless such persons are bound by a confidentiality agreement with Eli Lilly and Company or its subsidiaries. Note to Regulatory Authorities: This document may contain protected personal data and/or commercially confidential information exempt from public disclosure. Eli Lilly and Company requests consultation regarding release/redaction prior to any public release. In the United States, this document is subject to Freedom of Information Act (FOIA) Exemption 4 and may not be reproduced or otherwise disseminated without the written approval of Eli Lilly and Company or its subsidiaries. Necitumumab (IMC-11F8; LY3012211) Gemcitabine (LY188011) This is a Phase 1b/2 study in the first-line treatment of patients with advanced (Stage IV) Squamous Non-Small Cell Lung Cancer (NSCLC). -

List of Patented Medicines 2018
Patented Medicine Annual Report List 02 Apr 2019 Prices Review Board Protected A DIN Brand Chemical Name ATC Dosage Comments Status ABBVIE 02436027 HOLKIRA PAK 12.5/75/50/250 ombitasvir/paritaprevir/ritonavir/dasabuvir J05AX Oral Solid /Tablet Within Guidelines 02258595 HUMIRA - 40 MG/SYRINGE adalimumab L04AA Parenteral /Solution Within Guidelines 02312301 KALETRA 100/25 MG/TABLET lopinavir/ritonavir J05AE Oral Solid /Tablet Within Guidelines 02285533 KALETRA 200/50 MG/TABLET lopinavir/ritonavir J05AE Oral Solid /Tablet Within Guidelines 02243644 KALETRA 80/20 MG/MILLILITER lopinavir/ritonavir J05AE Oral Liquid /Solution Does Not Trigger 00884502 LUPRON DEPOT - 3.75 MG/VIAL leuprolide acetate L02AE Parenteral /Modified release injections Within Guidelines 00836273 LUPRON DEPOT - 7.5 MG/VIAL leuprolide acetate L02AE Parenteral /Modified release injections Within Guidelines 02239834 LUPRON DEPOT - 11.25 MG/VIAL leuprolide acetate L02AE Parenteral /Modified release injections Within Guidelines 02230248 LUPRON DEPOT - 22.5 MG/VIAL leuprolide acetate L02AE Parenteral /Modified release injections Within Guidelines 02239833 LUPRON DEPOT - 30 MG/VIAL leuprolide acetate L02AE Parenteral /Modified release injections Within Guidelines 02467550 MAVIRET 100/40 MG/TABLET glecaprevir/pibrentasvir J05AP Oral Solid /Tablet Subj. Investigation 02229145 NORVIR - 80 MG/MILLILITER ritonavir J05AE Oral Liquid /Solution Within Guidelines 02357593 NORVIR - 100 MG/TABLET ritonavir J05AE Oral Solid /Tablet Within Guidelines 02481332 ORILISSA - 150 MG/TABLET elagolix -

1 UST College of Science Department of Biological Sciences
UST College of Science Department of Biological Sciences 1 Pharmacogenomics of Myofascial Pain Syndrome An Undergraduate Thesis Submitted to the Department of Biological Sciences College of Science University of Santo Tomas In Partial Fulfillment of the Requirements for the Degree of Bachelor of Science in Biology Jose Marie V. Lazaga Marc Llandro C. Fernandez May 2021 UST College of Science Department of Biological Sciences 2 PANEL APPROVAL SHEET This undergraduate research manuscript entitled: Pharmacogenomics of Myofascial Pain Syndrome prepared and submitted by Jose Marie V. Lazaga and Marc Llandro C. Fernandez, was checked and has complied with the revisions and suggestions requested by panel members after thorough evaluation. This final version of the manuscript is hereby approved and accepted for submission in partial fulfillment of the requirements for the degree of Bachelor of Science in Biology. Noted by: Asst. Prof. Marilyn G. Rimando, PhD Research adviser, Bio/MicroSem 602-603 Approved by: Bio/MicroSem 603 panel member Bio/MicroSem 603 panel member Date: Date: UST College of Science Department of Biological Sciences 3 DECLARATION OF ORIGINALITY We hereby affirm that this submission is our own work and that, to the best of our knowledge and belief, it contains no material previously published or written by another person nor material to which a substantial extent has been accepted for award of any other degree or diploma of a university or other institute of higher learning, except where due acknowledgement is made in the text. We also declare that the intellectual content of this undergraduate research is the product of our work, even though we may have received assistance from others on style, presentation, and language expression. -

1 Supporting Information for a Microrna Network Regulates
Supporting Information for A microRNA Network Regulates Expression and Biosynthesis of CFTR and CFTR-ΔF508 Shyam Ramachandrana,b, Philip H. Karpc, Peng Jiangc, Lynda S. Ostedgaardc, Amy E. Walza, John T. Fishere, Shaf Keshavjeeh, Kim A. Lennoxi, Ashley M. Jacobii, Scott D. Rosei, Mark A. Behlkei, Michael J. Welshb,c,d,g, Yi Xingb,c,f, Paul B. McCray Jr.a,b,c Author Affiliations: Department of Pediatricsa, Interdisciplinary Program in Geneticsb, Departments of Internal Medicinec, Molecular Physiology and Biophysicsd, Anatomy and Cell Biologye, Biomedical Engineeringf, Howard Hughes Medical Instituteg, Carver College of Medicine, University of Iowa, Iowa City, IA-52242 Division of Thoracic Surgeryh, Toronto General Hospital, University Health Network, University of Toronto, Toronto, Canada-M5G 2C4 Integrated DNA Technologiesi, Coralville, IA-52241 To whom correspondence should be addressed: Email: [email protected] (M.J.W.); yi- [email protected] (Y.X.); Email: [email protected] (P.B.M.) This PDF file includes: Materials and Methods References Fig. S1. miR-138 regulates SIN3A in a dose-dependent and site-specific manner. Fig. S2. miR-138 regulates endogenous SIN3A protein expression. Fig. S3. miR-138 regulates endogenous CFTR protein expression in Calu-3 cells. Fig. S4. miR-138 regulates endogenous CFTR protein expression in primary human airway epithelia. Fig. S5. miR-138 regulates CFTR expression in HeLa cells. Fig. S6. miR-138 regulates CFTR expression in HEK293T cells. Fig. S7. HeLa cells exhibit CFTR channel activity. Fig. S8. miR-138 improves CFTR processing. Fig. S9. miR-138 improves CFTR-ΔF508 processing. Fig. S10. SIN3A inhibition yields partial rescue of Cl- transport in CF epithelia. -
Targeting the Epidermal Growth Factor Receptor in EGFR-Mutated Lung Cancer: Current and Emerging Therapies
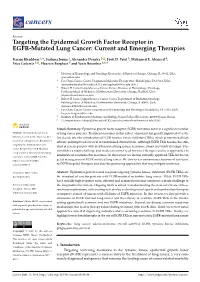
cancers Review Targeting the Epidermal Growth Factor Receptor in EGFR-Mutated Lung Cancer: Current and Emerging Therapies Karam Khaddour 1,*, Sushma Jonna 1, Alexander Deneka 2 , Jyoti D. Patel 3, Mohamed E. Abazeed 4, Erica Golemis 2 , Hossein Borghaei 5 and Yanis Boumber 3,6,* 1 Division of Hematology and Oncology, University of Illinois at Chicago, Chicago, IL 60612, USA; [email protected] 2 Fox Chase Cancer Center, Program in Molecular Therapeutics, Philadelphia, PA 19111, USA; [email protected] (A.D.); [email protected] (E.G.) 3 Robert H. Lurie Comprehensive Cancer Center, Division of Hematology/Oncology, Feinberg School of Medicine, Northwestern University, Chicago, IL 60611, USA; [email protected] 4 Robert H. Lurie Comprehensive Cancer Center, Department of Radiation Oncology, Feinberg School of Medicine, Northwestern University, Chicago, IL 60611, USA; [email protected] 5 Fox Chase Cancer Center, Department of Hematology and Oncology, Philadelphia, PA 19111, USA; [email protected] 6 Institute of Fundamental Medicine and Biology, Kazan Federal University, 420008 Kazan, Russia * Correspondence: [email protected] (K.K.); [email protected] (Y.B.) Simple Summary: Epidermal growth factor receptor (EGFR) mutations occur in a significant number Citation: Khaddour, K.; Jonna, S.; of lung cancer patients. Treatment outcomes in this subset of patients has greatly improved over the Deneka, A.; Patel, J.D.; Abazeed, M.E.; last decade after the introduction of EGFR tyrosine kinase inhibitors (TKIs), which demonstrated high Golemis, E.; Borghaei, H.; Boumber, Y. efficacy and improved survival in randomized clinical trials. Although EGFR TKIs became the stan- Targeting the Epidermal Growth dard of care in patients with EGFR-mutated lung cancer, resistance almost inevitably develops. -

Advances in Epidermal Growth Factor Receptor Specific Immunotherapy: Lessons to Be Learned from Armed Antibodies
www.oncotarget.com Oncotarget, 2020, Vol. 11, (No. 38), pp: 3531-3557 Review Advances in epidermal growth factor receptor specific immunotherapy: lessons to be learned from armed antibodies Fleury Augustin Nsole Biteghe1,*, Neelakshi Mungra2,*, Nyangone Ekome Toung Chalomie4, Jean De La Croix Ndong5, Jean Engohang-Ndong6, Guillaume Vignaux7, Eden Padayachee8, Krupa Naran2,* and Stefan Barth2,3,* 1Department of Radiation Oncology and Biomedical Sciences, Cedars-Sinai Medical, Los Angeles, CA, USA 2Medical Biotechnology & Immunotherapy Research Unit, Institute of Infectious Disease and Molecular Medicine, Faculty of Health Sciences, University of Cape Town, Cape Town, South Africa 3South African Research Chair in Cancer Biotechnology, Department of Integrative Biomedical Sciences, Faculty of Health Sciences, University of Cape Town, Cape Town, South Africa 4Sun Yat-Sen University, Zhongshan Medical School, Guangzhou, China 5Department of Orthopedic Surgery, New York University School of Medicine, New York, NY, USA 6Department of Biological Sciences, Kent State University at Tuscarawas, New Philadelphia, OH, USA 7Arctic Slope Regional Corporation Federal, Beltsville, MD, USA 8Department of Physiology, University of Kentucky, Lexington, KY, USA *These authors contributed equally to this work Correspondence to: Stefan Barth, email: [email protected] Keywords: epidermal growth factor receptor (EGFR); recombinant immunotoxins (ITs); targeted human cytolytic fusion proteins (hCFPs); recombinant antibody-drug conjugates (rADCs); recombinant antibody photoimmunoconjugates (rAPCs) Received: May 30, 2020 Accepted: August 11, 2020 Published: September 22, 2020 Copyright: © 2020 Biteghe et al. This is an open access article distributed under the terms of the Creative Commons Attribution License (CC BY 3.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. -

Human and Recombinat Coagulation Factor VIII
08 July 2016 EMA/PRAC/471535/2016 PRAC List of questions To be addressed by the marketing authorisation holder(s) for human and recombinant coagulation factor VIII containing medicinal products Referral under Article 31 of Directive 2001/83/EC resulting from pharmacovigilance data Procedure number: EMEA/H/A-31/1448 Advate EMEA/H/C/0520/A31/0078 Elocta EMEA/H/C/3964/A31/0006 Helixate Nexgen EMEA/H/C/0276/A31/0178 Iblias EMEA/H/C/4147/A31/0002 Kogenate EMEA/H/C/0275/A31/0185 Kovaltry EMEA/H/C/3825/A31/0004 Novoeight EMEA/H/C/2719/A31/0014 Nuwiq EMEA/H/C/2813/A31/0015 Obizur EMEA/H/C/2792/A31/0003 Refacto AF EMEA/H/C/0232/A31/0134 Voncento EMEA/H/C/2493/A31/0022 Active substances: human coagulation factor VIII; efmoroctocog alfa; moroctocog alfa; octocog alfa; simoctocog alfa; susoctocog alfa; turoctocog alfa 30 Churchill Place ● Canary Wharf ● London E14 5EU ● United Kingdom Telephone +44 (0)20 3660 6000 Facsimile +44 (0)20 3660 5555 Send a question via our website www.ema.europa.eu/contact An agency of the European Union © European Medicines Agency, 2016. Reproduction is authorised provided the source is acknowledged. 1. Background Today’s standard treatment of congenital haemophilia (and acquired haemophilia A) is based on prophylactic or on-demand replacement therapy with coagulation factor VIII (FVIII), either with plasma derived or with recombinant FVIII products. Principally both substance classes may be used for prophylactic treatment as well as for therapeutic treatment in case of spontaneous bleedings. Inhibitor development in haemophilia A patients receiving FVIII products mostly occurs in previously untreated or minimally treated patients (PUPs), who are still within the first 50 days of exposure to the treatment.