Aboriginal Community Controlled Health Services in a Challenging Policy Context
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Cooks River Valley Association Inc. PO Box H150, Hurlstone Park NSW 2193 E: [email protected] W: ABN 14 390 158 512
Cooks River Valley Association Inc. PO Box H150, Hurlstone Park NSW 2193 E: [email protected] W: www.crva.org.au ABN 14 390 158 512 8 August 2018 To: Ian Naylor Manager, Civic and Executive Support Leichhardt Service Centre Inner West Council 7-15 Wetherill Street Leichhardt NSW 2040 Dear Ian Re: Petition on proposal to establish a Pemulwuy Cooks River Trail The Cooks River Valley Association (CRVA) would like to submit the attached petition to establish a Pemulwuy Cooks River Trail to the Inner West Council. The signatures on the petition were mainly collected at two events that were held in Marrickville during April and May 2018. These events were the Anzac Day Reflection held on 25 April 2018 in Richardson’s Lookout – Marrickville Peace Park and the National Sorry Day Walk along the Cooks River via a number of Indigenous Interpretive Sites on 26 May 2018. The purpose of the petition is to creatively showcase the history and culture of the local Aboriginal community along the Cooks River and to publicly acknowledge the role of Pemulwuy as “father of local Aboriginal resistance”. The action petitioned for was expressed in the following terms: “We, the undersigned, are concerned citizens who urge Inner West Council in conjunction with Council’s Aboriginal and Torres Strait Islander Reference Group (A&TSIRG) to designate the walk between the Aboriginal Interpretive Sites along the Cooks River parks in Marrickville as the Pemulwuy Trail and produce an information leaflet to explain the sites and the Aboriginal connection to the Cooks River (River of Goolay’yari).” A total of 60 signatures have been collected on the petition attached. -

EORA Mapping Aboriginal Sydney 1770–1850 Exhibition Guide
Sponsored by It is customary for some Indigenous communities not to mention names or reproduce images associated with the recently deceased. Members of these communities are respectfully advised that a number of people mentioned in writing or depicted in images in the following pages have passed away. Users are warned that there may be words and descriptions that might be culturally sensitive and not normally used in certain public or community contexts. In some circumstances, terms and annotations of the period in which a text was written may be considered Many treasures from the State Library’s inappropriate today. Indigenous collections are now online for the first time at <www.atmitchell.com>. A note on the text The spelling of Aboriginal words in historical Made possible through a partnership with documents is inconsistent, depending on how they were heard, interpreted and recorded by Europeans. Original spelling has been retained in quoted texts, while names and placenames have been standardised, based on the most common contemporary usage. State Library of New South Wales Macquarie Street Sydney NSW 2000 Telephone (02) 9273 1414 Facsimile (02) 9273 1255 TTY (02) 9273 1541 Email [email protected] www.sl.nsw.gov.au www.atmitchell.com Exhibition opening hours: 9 am to 5 pm weekdays, 11 am to 5 pm weekends Eora: Mapping Aboriginal Sydney 1770–1850 was presented at the State Library of New South Wales from 5 June to 13 August 2006. Curators: Keith Vincent Smith, Anthony (Ace) Bourke and, in the conceptual stages, by the late Michael -

Koori Centre Handbook
Koori Centre handbook Set a course for Handbooks online: www.usyd.edu.au/handbooks Acknowledgements Acknowledgements The Arms of the University Sidere mens eadem mutato Though the constellation may change the spirit remains the same Copyright Disclaimers This work is copyright. No material anywhere in this work may be 1. The material in this handbook may contain references to persons copied, reproduced or further disseminated ± unless for private use who are deceased. or study ± without the express and written permission of the legal 2. The information in this handbook was as accurate as possible at holder of that copyright. The information in this handbook is not to be the time of printing. The University reserves the right to make used for commercial purposes. changes to the information in this handbook, including prerequisites for units of study, as appropriate. Students should Official course information check with faculties for current, detailed information regarding Faculty handbooks and their respective online updates, along with units of study. the University of Sydney Calendar, form the official legal source of Price information relating to study at the University of Sydney. Please refer to the following websites: The price of this handbook can be found on the back cover and is in Australian dollars. The price includes GST. www.usyd.edu.au/handbooks www.usyd.edu.au/calendar Handbook purchases You can purchase handbooks at the Student Centre, or online at Amendments www.usyd.edu.au/handbooks All authorised amendments to this handbook -

Koori Centre
2008 handbook Koori Centre Set a course for Handbooks online … visit www.usyd.edu.au/handbooks Acknowledgements Acknowledgements The Arms of the University Sidere mens eadem mutato Though the constellation may change the spirit remains the same Copyright Disclaimers This work is copyright. No material anywhere in this work may be 1. The material in this handbook may contain references to persons copied, reproduced or further disseminated ± unless for private use who are deceased. or study ± without the express and written permission of the legal 2. The information in this handbook was as accurate as possible at holder of that copyright. The information in this handbook is not to be the time of printing. The University reserves the right to make used for commercial purposes. changes to the information in this handbook, including prerequisites for units of study, as appropriate. Students should Official course information check with faculties for current, detailed information regarding Faculty handbooks and their respective online updates along with the units of study. University of Sydney Calendar form the official legal source of Price information relating to study at the University of Sydney. Please refer to the following websites: The price of this handbook can be found on the back cover and is in www.usyd.edu.au/handbooks Australian dollars. The price includes GST. www.usyd.edu.au/calendar Handbook purchases Amendments You can purchase handbooks at the Student Centre, or online at All authorised amendments to this handbook can be found -

Historical Information About the 1780S in Australia
The information supplied in this document was sourced from the Decade timeline section of MY PLACE FOR TEACHERS website: www.myplace.edu.au Historical information about the 1780s in Australia Cultural differences On 26 January 1788, the British government through Governor Arthur Phillip (1738–1814) claimed sovereignty over the area that Captain James Cook had named New South Wales. They also claimed ownership of the land through the legal concept of terra nullius (land belonging to no-one), ignoring the already existing land ownership and lore of the Indigenous peoples there. Land was at the centre of the conflict between the Sydney clans and the British colonists. In 1787 Lord Sydney of the Colonial Office had officially recognised the presence of Indigenous inhabitants by giving instructions to Governor Phillip to open friendly communications with them and encourage the convicts and marines to show them kindness. His instructions included measures of protection for the local Indigenous people, and punishments for those who harmed them. The British did not, however, acknowledge Indigenous ownership of the land. The people of the First Fleet did not understand the ways of the local Indigenous peoples they encountered, and their diaries and journals record the lack of respect that many members of the First Fleet had for local Indigenous people. The colonists did not understand the diversity of Indigenous Australian nations, each with a distinct language and culture, or the complexity of Indigenous systems of lore. For example, an important understanding is to seek permission to enter another group's country. On seeing the First Fleet, the Cadigal people ran down to the water's edge and shook their spears at them. -
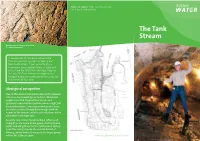
The Tank Stream Today
Front cover photo: In the Tank Stream today. Photograph: Sydney Water. The Tank Stream Mason’s marks in the block work inside the Tank Stream tunnel. In recognition of the importance of the Tank Stream to the people of Sydney and New South Wales, it was protected by a Permanent Conservation Order in 1989 and entered on the NSW State Heritage Register in 1999. The Tank Stream is recognised as being of national importance to the European settlement of Australia. Aboriginal occupation Due to the almost immediate impact of European colonists, our knowledge of Sydney’s Aboriginal people is limited. Early settlers casual and systematic observations provide some insight, but basic information is missing or ambiguous. Even the names of the Aboriginal landscape with the names of the stream and the other features in the catchment have been lost. Recently researchers favour Gadigal (often spelt Cadigal) as the name of the group that had some rights and obligations for the land around Sydney Cove. The Gadigal spoke the coastal dialect of Dharug, which makes them part of a larger group within the Sydney region. SW94 09/10 Printed on recycled paper John Skinner Prout, The Tank Stream, Sydney, circa 1842. A tour group inspects the Tank Stream. pencil,watercolour, opaque white highlights, 25.5 x 37.5cm Purchased 1913 Collection: Art Gallery of NSW The Tank Stream runs underground from near Hyde Park to Circular Quay. Photograph: Brenton McGeachie of AGNSW ydney’s first water supply As the water source for both humans and their Major Grose made a significant environmental livestock, it was essential to maintain water quality decision. -
Attachment A4
Attachment A4 Brief Aboriginal Historical Study of the Botany Road Precinct and Surrounds – Botany Road Precinct Brief Aboriginal History of the Botany Road Corridor and Surrounds Cox Inall Ridgeway for THE CITY OF SYDNEY FINAL April 2021 About this document This brief Aboriginal Historical Study has been prepared by Indigenous social change agency Cox Inall Ridgeway (CIR) for the City of Sydney Council (the City) as part of the strategic planning review of an area known as the ‘Botany Road Corridor’ (the Study Area). It is one of a number of reports prepared by CIR for the City, including a Project Report, Statement of Aboriginal Significance for the area, and an Archaeological Assessment. This brief history draws on historical research including interviews conducted by CIR with Aboriginal and Torres Strait Islander community members in 2020. It provides a brief overview of the history of the Study Area and surrounds (including Redfern, Waterloo, Eveleigh and Alexandria) and profiles a number of places which help illustrate the rich and diverse social history of the area, prioritising Aboriginal voices, views and stories. It is a short introductory history and is not intended to be a complete account of the rich and diverse histories of the Study Area and surrounds. This document has been authored by CIR for the City. It reflects the independent insights and analysis of CIR, not the City of Sydney Council or any other organisation. While all care has been taken by CIR to ensure information is accurate, the document may contain errors. i The copyright for this document is vested with the City of Sydney Council. -

Living Centres for Living Cultures 2 a Snapshot Report on the Status of NSW Aboriginal Cultural Venues
Living Centres for Living Cultures 2 A snapshot report on the status of NSW Aboriginal Cultural Venues Produced by Museums & Galleries of NSW With the support of Terri Janke & Company Funded by Create NSW Living Centres for Living Cultures 2 Living Centres for Living Cultures 2 Written and researched by: Steve Miller, Michael Rolfe, Terri Janke and Melissa Abraham Museums & Galleries of NSW, 2017 Commissioned by: Create NSW Writing assistance: Sarah Grant, Paralegal Citation: Steve Miller, Michael Rolfe, Terri Janke and Melissa Abraham, Living Centres for Living Cultures 2: A snapshot report of the status of NSW Aboriginal cultural venues, Museums & Galleries of NSW, 2017 © Museums & Galleries of NSW, 2017 WARNING The document contains names of deceased persons of Aboriginal and Torres Strait Islander. It also contains some language that might be considered offensive. Important legal notice The laws and policies cited in this book are current as at August 2017. They are generally discussed for the purposes of providing this report. No person should rely on the contents of this report for a specific legal matter but should obtain professional legal advice from a qualified legal practitioner. 2 Living Centres for Living Cultures 2 1.Indigenous peoples have the right to maintain, control, protect and develop their cultural heritage, traditional knowledge and traditional cultural expressions, as well as the manifestations of their sciences, technologies and cultures, including human and genetic resources, seeds, medicines, knowledge of the properties of fauna and flora, oral traditions, literatures, designs, sports and traditional games and visual and performing arts. They also have the right to maintain, control, protect and develop their intellectual property over such cultural heritage, traditional knowledge, and traditional cultural expressions. -

A History of Aboriginal Illawarra Volume 1: Before Colonisation
University of Wollongong Research Online Senior Deputy Vice-Chancellor and Deputy Vice- Senior Deputy Vice-Chancellor and Deputy Vice- Chancellor (Education) - Papers Chancellor (Education) 1-1-2015 A history of Aboriginal Illawarra Volume 1: Before colonisation Mike Donaldson University of Wollongong, [email protected] Les Bursill University of Wollongong Mary Jacobs TAFE NSW Follow this and additional works at: https://ro.uow.edu.au/asdpapers Part of the Arts and Humanities Commons, and the Social and Behavioral Sciences Commons Recommended Citation Donaldson, Mike; Bursill, Les; and Jacobs, Mary: A history of Aboriginal Illawarra Volume 1: Before colonisation 2015. https://ro.uow.edu.au/asdpapers/581 Research Online is the open access institutional repository for the University of Wollongong. For further information contact the UOW Library: [email protected] A history of Aboriginal Illawarra Volume 1: Before colonisation Abstract Twenty thousand years ago when the planet was starting to emerge from its most recent ice age and volcanoes were active in Victoria, the Australian continent’s giant animals were disappearing. They included a wombat (Diprotodon) seen on the right, the size of a small car and weighing up to almost three tons, which was preyed upon by a marsupial lion (Thylacoleo carnifex) on following page. This treedweller averaging 100 kilograms, was slim compared to the venomous goanna (Megalania) which at 300 kilograms, and 4.5 metres long, was the largest terrestrial lizard known, terrifying but dwarfed by a carnivorous kangaroo (Propleopus oscillans) which could grow three metres high. Keywords before, aboriginal, colonisation, 1:, history, volume, illawarra Disciplines Arts and Humanities | Social and Behavioral Sciences Publication Details Bursill, L., Donaldson, M. -

Aboriginal-Sydney-Index.Pdf (Pdf, 664.12
Aboriginal Sydney 2nd Edition Index INDEX Aboriginal community NAISDA; Powerhouse Birnie, Captain James, 96 organisations, 71, 78–82 Museum; Tank Stream Black Theatre, 81–82, 83 Aboriginal Dance Theatre, 82 public artworks; Yiribana Blacktown (also ‘the Black Aboriginal Heritage Office, 47, Gallery Town’), 117, 123, 131–135, 55–56 Cranebrook, 140–141 137 Aboriginal Housing Company, Parramatta, 120–121 Maria Lock, 139, 143–145 78–79 Redfern, 74–75, 81–82 Blacktown Native Institution, Aboriginal Land Rights Act see also Boomalli Aboriginal 117, 120, 131–135, 136–138 (NSW), 101, 104 Artists Cooperative; Timbery, Maria Lock, 143–145 Aboriginal Legal Service, 79–80 Laddie; Watson, Judy see also Parramatta Native Aboriginal Medical Service, Australia Day, 3–4, 17, 22, 28, Institution 80–81 73, 97 ‘The Block’, 79 Aboriginal reserves, xxvi, Australian Hall building, Bondi Golf Course, 71, 86–87 101–102, 106, 1, 16–18 Bondi Points, 87 Aboriginal skeletal remains, Australian Museum, iv, Boomalli Aboriginal Artists xviii, 86 1, 12–13, 86, 87, 141 Cooperative, iv, 71, 82, 88–91 Aboriginal trade routes, 132, Boorooberongal clan, 123, 144 138 backed blades, 87 bora rings, 5 Aborigines Advancement Balls Head Reserve, 31, 34–35 Bostock, Euphemia, 90 League, 17 Balmoral Beach, 31, 48–49 Bostock, Gerald, 82 Aborigines Progressive Baluderri, 11, 128–129 Bostock, Lester, 82 Association, 17 Bangarra Dance Theatre, iv, 1, Botanic Gardens, iv, 1, 3–6, 7 Aborigines Protection Act, 17, 19–20, 82 Botany Bay National Park, see 145 Banks, Sir Joseph, 97, 130 Kamay -

Facts for Students
www.forteachersforstudents.com.au Copyright © 2017 FOR TEACHERS for students NEW SOUTH WALES Facts for Students New South Wales (NSW) is a large state in south-eastern Australia. It is home to many famous attractions, including its capital city: Sydney. The history of New South Wales Indigenous History The original inhabitants of Sydney (the Cadigal people) spoke the Eora language. In Eora, Sydney is called Warran meaning ‘here’ or ‘this place’. Other dialects of the Sydney area include Dharug, Kurringgai and Dhawawal. The Eora people were hunters and gatherers and inhabited coastal campsites where fish (such as snapper) and shellfish (oysters, mussels and cockles) were plentiful. Song and dance were important elements of Aboriginal life. Rock engravings depicting humans and native animals such as whales and wallabies have been found throughout the Sydney area, although many have been covered by roads or buildings. European Arrival New South Wales is Australia’s oldest state. It was named in 1770 by Captain James Cook who, after falsely proclaiming that the land was uninhabited, claimed it for Britain. On 26 January 1788 the First Fleet, eleven ships commanded by Captain Arthur Phillip, arrived in Botany Bay. The ships carried 700 convicts sent from Britain’s overflowing gaols and 150 officers and Marine guards. Botany Bay was the intended location of the penal colony, however, the site was judged unfit and Port Jackson was chosen instead. Page 1 www.forteachersforstudents.com.au Copyright © 2017 FOR TEACHERS for students NEW SOUTH WALES In 1793, the first free settlers arrived in NSW: five single men and two families. -
Dr Charles Perkins AO
Dr Charles Perkins AO Annual Memorial Oration and Memorial Prize Thursday 26 October 2006 The University of Sydney in collaboration with the Koori Centre PROGRAM 6.00pm Event commences The Great Hall 6.30pm Official proceedings begin Mr Neville Perkins OAM, Master of Ceremonies 6.40pm Welcome to Country Mr Charles Madden Director, Aboriginal Medical Service 6.45pm Vice-Chancellor’s Address Professor Gavin Brown AO FAA Vice-Chancellor and Principal The University of Sydney 6.50pm Dr Charles Perkins AO Annual Memorial Oration Professor Sandra Eades The Sax Institute Faculty of Medicine, The University of Sydney 7.25pm Vote of Thanks and Introduction to Dr Charles Perkins AO Memorial Prize Ms Michelle Blanchard, Acting Director, Koori Centre, The University of Sydney 7.30pm Presentation of the Dr Charles Perkins AO Annual Memorial Prize Ms Michelle Blanchard, Acting Director of the Koori Centre Prizes to be presented by The Chancellor, The Honourable Justice Kim Santow OAM and Mrs Eileen Perkins 7.45pm Summation and Close of Proceedings Mr Neville Perkins OAM, Master of Ceremonies 8.30pm Event concludes The Great Hall Dr Charles Perkins AO Annual Memorial Oration In 2001, The University of Sydney in collaboration with the Koori Centre launched the Dr Charles Perkins AO Annual Memorial Oration. The establishment of the Oration began as a recommendation of the Committee to Review Aboriginal Education at The University of Sydney, of which Dr Perkins was a member. The University, in consultation with the Koori Centre, adopted in principle that the University establish an Annual Oration, “to be given by an internationally high-profile race relations leader…as a demonstration of its continuing commitment to fostering excellence in education and leadership among its Indigenous staff and graduates.” (Vice-Chancellor’s Preliminary Response to the Report of the Committee established to review Aboriginal education in the University of Sydney, 2000).