Mpha-Magazine-Winter-2020.Pdf
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
2020 Final Public Subsidy Payments
CAMPAIGN FINANCE AND PUBLIC DISCLOSURE BOARD RELEASES FINAL PUBLIC SUBSIDY PAYMENT AMOUNTS FOR 2020 ELECTION During 2020 the Campaign Finance and Public Disclosure Board distributed $2,131,887 in public subsidy payments to 349 candidates running for state senate or state representative. The 349 candidates who received a public subsidy payment represent 78% of the 449 legislative candidates who were on the general election ballot. A list of qualifying candidates and the payments they received is attached. Of the 504 candidates who filed for state legislative office this year, 401 (79.3%) signed voluntary agreements to abide by spending limits and other conditions required to be eligible for public subsidy payments for their campaigns. To qualify for public subsidy a candidate must: • be opposed at either the primary or general election, • appear on the general election ballot, • sign and file a public subsidy agreement with the Board to abide by applicable campaign expenditure limits, and • raise a specified amount in contributions from individuals eligible to vote in Minnesota counting only the first $50 from each donor. Money for the public subsidy program comes from the state general fund. A portion of public subsidy money is allocated to specific parties and districts based on taxpayer checkoffs on income and property tax returns. By office and party, the total public subsidy payments totaled: DFL RPM State Senate $670,054 $393,772 House of Representatives $663,589 $404,471 Total $1,333,643 $798,243 DFL = Democratic Farmer Labor RPM = Republican Party of Minnesota Note: No other major or minor party candidates qualified for a public subsidy payment in 2020. -
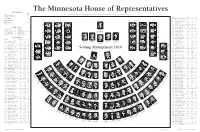
2020 Minnesota House of Representatives Seating Chart
The Minnesota House of Representatives House Leadership Seat Melissa Hortman .................................... 139 Minnesota House of Representatives Public Information Services, 651-296-2146 or 800-657-3550 Speaker of the House District Room* 296- Seat Ryan Winkler.......................................... 102 44A Klevorn, Ginny (DFL) .........581 ....... 5511 ..... 104 Majority Leader 37A Koegel, Erin (DFL) .............375 ....... 5369 ..... 126 48B Kotyza-Witthuhn, Carlie (DFL) ....567 ............7449 ...........81 Golden Valley—45B Bloomington—49B Shelly Christensen Kurt Daudt ............................................... 23 Mike Freiberg Stillwater—39B 58A Koznick, Jon (R) .................229 ....... 6926 ......... 5 Seat 129 Steve Elkins Seat 135 Minority Leader Seat 124 9B Kresha, Ron (R) ...................207 ....... 4247 ....... 12 Seat 6 41B Kunesh-Podein, Mary (DFL)... 445 ..........4331 ......... 97 Seat 1 Seat 11 Mary Franson Luverne—22A Alexandria—8B Joe Schomacker 5B Layman, Sandy (R) ..............233 ....... 4936 ....... 38 Shane Mekeland House Officers Clear Lake—15B Maplewood—53A Rosemount—57B St. Peter—19A Jeff Brand 59A Lee, Fue (DFL) ....................485 ....... 4262 ..... 125 Seat 128 John Huot Tou Xiong Tou Seat 134 Patrick D. Murphy .......... 142 Marilee Davis .................. 141 Seat 123 Seat 139 Chief Clerk Desk Clerk Melissa Hortman 66B Lesch, John (DFL) ...............563 ....... 4224 ..... 116 Timothy M. Johnson ....... 143 David G. Surdez ............. 140 Brooklyn Park—36B Seat 7 Seat 2 26A Liebling, Tina (DFL) ...........477 ....... 0573 ..... 114 Speaker of the House Seat 12 Peggy Scott Ron Kresha 1st Asst. Chief Clerk Legislative Clerk John Poston Andover—35B Little Falls—9B Brooklyn Center—40B Lake Shore—9A International Falls—3A 4A Lien, Ben (DFL) ..................415 ....... 5515 ....... 72 Gail C. Romanowski ....... 144 Bob Meyerson ................... 69 South St. Paul—52A Samantha Vang Seat 127 2nd Asst. -

MACTE Weekly Legislative Update, 2.16.20 Prepared by Cyndy Crist, MACTE Legislative and Policy Liaison 2020 Session Underway. Th
MACTE Weekly Legislative Update, 2.16.20 Prepared by Cyndy Crist, MACTE Legislative and Policy Liaison 2020 Session Underway. The Minnesota Legislature opened its 2020 session on Tuesday, February 11. As in all even-numbered years, this shorter session will focus on a bonding bill as well as other policy and funding issues it may choose to address. It seems likely that many of the policy issues that were included in omnibus bills last year but ultimately not enacted because of the deep divisions between the House, Senate, and Governor will be brought up again this year. This could include many of the preparation and licensure issues of interest to us in 2019, including changes in the tiered licensure structure and measures to increase the diversity of teachers in our state. In addition, the predicted budget surplus will be much on the minds of legislators as they decide whether to use or save surplus dollars and/or cut planned spending to reflect the additional funding. The committee structure from 2019 remains unchanged, although two new legislators have now been sworn in. In House District 60A, DFLer Sydney Jordan won a special election to fill the seat left vacant by the death of Diane Loeffler. House District 30A will now be represented by Republican Paul Novotny who was elected to fill the seat left vacant by the resignation of Nick Zerwas. Since the new members are of the same party as the incumbents they are replacing, there is no change in the balance between the two parties in the House. It is also worth noting that all members of the House and Senate are up for election this year, and to date, approximately 14 current members have announced that they will not be seeking re-election. -

Minnesota House of Representatives Bonding Bill Roll Call Vote Total 75 Yea and 57 Nay
Minnesota House of Representatives bonding bill roll call vote Total 75 yea and 57 nay. Does not meet required 81 yea votes to pass. July 20, 2020 44B DFL Rep. Patty Acomb Minnetonka Y 55B R Rep. Tony Albright Prior Lake N 12B R Rep. Paul Anderson Starbuck N 12A R Rep. Jeff Backer Browns Valley N 34B DFL Rep. Kristin Bahner Maple Grove Y 31B R Rep. Cal Bahr East Bethel N 17B R Rep. Dave Baker Willmar N 42B DFL Rep. Jamie Becker-Finn Roseville Y 27A R Rep. Peggy Bennett Albert Lea N 41A DFL Rep. Connie Bernardy New Brighton Y 57A DFL Rep. Robert Bierman Apple Valley Y 47B R Rep. Greg Boe Chaska N 19A DFL Rep. Jeff Brand St. Peter Y 56A DFL Rep. Hunter Cantrell Savage Y 50B DFL Rep. Andrew Carlson Bloomington Y 45A DFL Rep. Lyndon Carlson, Sr. Crystal Y Rep. Michelle (Shelly) 39B DFL Christensen Stillwater Y 54A DFL Rep. Anne Claflin South St. Paul Y 19B DFL Rep. Jack Considine Jr. Mankato Y 24B R Rep. Brian Daniels Faribault N 31A R Rep. Kurt Daudt Crown N 28B R Rep. Greg Davids Preston N 63A DFL Rep. Jim Davnie Minneapolis Y 59B DFL Rep. Raymond Dehn Minneapolis Y 13A R Rep. Lisa Demuth Cold Spring N 39A R Rep. Bob Dettmer Forest Lake N 21B R Rep. Steve Drazkowski Mazeppa N 03A DFL Rep. Rob Ecklund International Falls Y 49A DFL Rep. Heather Edelson Edina Y 49B DFL Rep. Steve Elkins Bloomington Y 15A R Rep. Sondra Erickson Princeton NV 01A R Rep. -

Regular City Council – February 10, 2020
CITY OF MADISON AGENDA AND NOTICE OF MEETING Regular Meeting of the City Council – 5:00 PM Monday February 10, 2020 Madison Municipal Building 1. CALL THE REGULAR MEETING TO ORDER Mayor Thole will call the meeting to order. 2. APPROVE AGENDA Approve the agenda as posted in accordance with the Open Meetings law, and herein place all agenda items on the table for discussion. A MOTION is in order. (Council) 3. APPROVE MINUTES Page 1 A copy of the January 27, 2020 regular meeting minutes are enclosed. A MOTION is in order. (Council) 4. PUBLIC PETITIONS, REQUESTS, HEARINGS, AND COMMUNICATIONS (public/mayor/council) Members of the audience wishing to address the Council with regard to an agenda item, presentation of a petition, utility customer hearing, or a general communication should be recognized at this time. A MOTION may be in order (Public/Council) 5. CONSENT AGENDA A. Cash Investment Balance – January 2020 - receive Page 4 B. MMUA Training – February 10, 2020 – receive Page 5 C. MRES Board Meeting – February 13, 2020 – receive Page 6 D. MRES Legislative Line – February 4, 2020 – receive Page 8 E. LqP Computer Commuter – February 2020 – receive Page 13 F. Council Revenue/Expenses – January 2020 – receive Page 14 G. Senator Dahmes – January 2020 – receive Page 17 H. Liquor Store Report – January 2020 – receive Page 20 I. MDH Sanitary Survey – receive Page 22 J. MEDA Loan Note Status – January 2020 – receive Page 32 K. Mediacom Franchise Fee – 2019 – receive Page 33 L. Regular Drill/Special Meeting – January 2020 - receive Page 34 M. Water Plant Report – January 2020 – receive Page 37 N. -
SC COLA Directory-Reference June 2020
Protecting our lakes, rivers and waterways today and tomorrow Directory & Reference For distribution to members only June 2020 We thank our sponsors because they help us meet our goals. Please buy from them and tell them you saw their ad here. Please note that SC COLA is not responsible for their goods or services. EROSION CONTROL HILLSIDE STABILIZATION LAND RECLAMATION Before Installation After Call: (651) 353-5144 Email: [email protected] www.midwesterosiontech.com 1 2 3 CONTENTS About SC COLA ......................................................................................................................... 5 SC COLA Contacts ................................................................................................................. 6-7 Fundraising Ideas ....................................................................................................................... 8 Educational Resources .............................................................................................................. 9 Grant Sources ............................................................................................................................ 9 Service Providers ................................................................................................................ 10-13 City/Township, County and Government Contacts .............................................................. 14-20 4 ABOUT SC COLA SC COLA is a Coalition of Lake Associations in Sherburne County, Minnesota formed in 2017. Working -

2021-2022 Minnesota House of Representatives Minneapolis and Saint Paul
2021-2022 Minnesota House of Representatives Minneapolis and Saint Paul North Oaks Brooklyn Park 10 St. Vincent Fridley ¤£ Mahtomedi Humboldt 41A Connie Bernardy (DFL) Brooklyn Center Warroad ¨¦§694 Lancaster Roseau New Brighton Birchwood Village Roosevelt Arden Hills Hallock Anoka Shoreview Kittson Gem Lake White Bear Lake Badger Vadnais Heights Roseau Williams Lake Bronson 42A Kelly Moller (DFL) Greenbush 40B Samantha Vang (DFL) Hilltop Baudette Halma Kennedy Columbia Heights 45A Cedrick Frazier (DFL) Donaldson Lake of the Woods Karlstad Ranier 42B Jamie Becker-Finn (DFL) Strathcona New Hope International Falls Strandquist 41B Sandra Feist (DFL) Crystal ¨¦§694 Stephen 01A John Burkel (R) ¤£75 Middle River Marshall Argyle Newfolden Littlefork Robbinsdale Little Canada St. Anthony Holt Grygla 59A Fue Lee (DFL) Oslo Viking ¤£61 Alvarado Warren Roseville Maplewood Koochiching North St. Paul Goodridge Big Falls Thief River Falls 43A Peter Fischer (DFL) Pennington 02A Matthew Grossell (R) 60A Sydney Jordan (DFl) St. Hilaire Orr 45B Mike Freiberg (DFL) ¤£71 East Grand Forks Plummer Kelliher Ramsey Beltrami Winton Lauderdale 66A Alice Hausman (DFL) 43B Leon Lillie (DFL) Red Lake Falls Mizpah Ely Oakdale Golden Valley 01B Debra Kiel (R) Red Lake Oklee Falcon Heights Northome 03A Rob Ecklund (DFL) Fisher Brooks Effie Cook Crookston Tower Trail Funkley Grand Marais Gully Bigfork 59B Esther Agbaje (DFL) Polk Mentor Gonvick Cook Clearbrook Blackduck 66B Athena Hollins (DFL) Erskine Climax McIntosh Leonard Tenstrike Babbitt Squaw Lake 394 Fosston -

ELECTION DIRECTORY for the 2021-2022 MINNESOTA LEGISLATURE
Preliminary 2020 ELECTION DIRECTORY for the 2021-2022 MINNESOTA LEGISLATURE Minnesota House of Representatives and Minnesota Senate Jan. 5, 2021 2021-2022 House Membership Statistics 70 DFL members 64 Republican members 51 members are women 83 members are men 13 Republican women 51 Republican men 38 DFL women 32 DFL men Newly elected members 23 newly elected members for 2021-22, includes two former members 12 newly elected DFL members 11 newly elected Republican members 17.2 percent of 2021-22 members did not serve last session 11 newly elected members are women 12 newly elected members are men 89 percent of incumbents on the ballot were re-elected 0 Republican incumbents lost 5 DFL incumbents lost 18 seats were open at the time of the election 4 races were uncontested (18A Dean Urdahl; 28A Gene Pelowski, Jr.; 49A Heather Edelson; 60B Mohamud Noor) New House DFL members Esther Agbaje ............................... 59B Emma Greenman ........................ 63B Kaela Berg ..................................... 56B Jessica Hanson .............................56A Liz Boldon .................................... 25B Athena Hollins ............................. 66B Sandra Feist .................................. 41B Heather Keeler ...............................4A Cedrick Frazier ............................45A Liz Reyer ....................................... 51B Luke Frederick ............................. 19B John Thompson ...........................67A New House Republican members Susan Akland ...............................19A Patricia -

April 29, 2020 Governor Tim Walz 130 State Capitol 75 Rev. Dr. Martin
April 29, 2020 Governor Tim Walz 130 State Capitol 75 Rev. Dr. Martin Luther King Jr. Blvd. St. Paul, MN 55155 via electronic delivery Dear Governor Walz: Minnesotans have done an outstanding job staying in place, flattening the curve, and giving hospitals and health care providers the time they need to prepare for COVID-19. As the state brings down the rate of infections, closures have resulted in significant economic hardship for small businesses—leading to an unemployment crisis. We appreciate the steps you took in your most recent executive order that will allow businesses in manufacturing, industrial, and office settings that are non-customer facing to reopen. We hope that this is a first step in the process of getting more Minnesotans back to work. Today, we are asking you to continue this process by allowing RV resorts and campgrounds to reopen. We have the privilege to represent areas of the state known for its lakes and outdoor recreational opportunities. The tourism industry is vital for our local economy and the current closures are hurting many family businesses that have owned and operated resorts and campgrounds for generations. Giving campgrounds and RV resorts the flexibility to reopen will help these family owned businesses recover some of the losses they have incurred. Minnesotans have proven time and again that they care about their health and safety of their neighbors. We have no doubt that these families can reopen their businesses in a way that preserves the health and safety of their customers. Please give them the opportunity to do so. -

2019-2020 Minnesota House of Representatives Minneapolis and Saint Paul
2019-2020 Minnesota House of Representatives Minneapolis and Saint Paul Includes Results from 02/04/2020 Special Election North Oaks Brooklyn Park 10 St. Vincent Fridley Mahtomedi Humboldt 41A Connie Bernardy DFL Brooklyn Center Warroad 694 Lancaster Roseau New Brighton Birchwood Village Roosevelt Arden Hills Hallock Anoka Shoreview Kittson White Bear Lake Badger Gem Lake Vadnais Heights Roseau Williams Lake Bronson 42A Kelly Moller DFL Greenbush 40B Samantha Vang DFL Hilltop Baudette Halma Kennedy Columbia Heights 45A Lyndon R. Carlson DFL Donaldson Lake of the Woods Karlstad Ranier 42B Jamie Becker-Finn DFL Strathcona New Hope International Falls Strandquist 41B Mary Kunesh-Podein DFL Crystal 694 Stephen 01A Dan Fabian R 75 Middle River Marshall Argyle Newfolden Littlefork Robbinsdale Little Canada St. Anthony Holt Grygla 59A Fue Lee DFL Oslo Viking 61 Alvarado Warren Roseville Maplewood Koochiching North St. Paul Goodridge Big Falls Thief River Falls 43A Peter M Fischer DFL Pennington 02A Matthew J. Grossell R 60A Sydney Jordan DFL St. Hilaire Orr 45B Mike Freiberg DFL 71 East Grand Forks Plummer Kelliher Ramsey Beltrami Winton Lauderdale 66A Alice Hausman DFL 43B Leon M. Lillie DFL Red Lake Falls Mizpah Ely Oakdale Golden Valley 01B Debra Kiel R Red Lake Oklee Falcon Heights Northome 03A Rob Ecklund DFL Fisher Brooks Effie Cook Crookston Tower Trail Funkley Grand Marais Gully Bigfork 59B Raymond Dehn DFL Polk Mentor Gonvick Cook Clearbrook Blackduck 66B John Lesch DFL Erskine Climax McIntosh Leonard Tenstrike Babbitt Squaw Lake 394 Clearwater Turtle River Nielsville Beltrami Fosston 60B Mohamud Noor DFL 67A Tim Mahoney DFL Fertile Winger St. -

House District Reports by Institution
Alexandria Technical and Community College Credit Student Enrollment by House District Fiscal Year 2018-2019 Representative and District Enrollment District 08B: Rep. Mary Franson 654 District 12B: Rep. Paul Anderson 499 District 12A: Rep. Jeff Backer 318 District 01B: Rep. Debra Kiel 167 District 09A: Rep. John Poston 134 District 01A: Rep. John Burkel 131 District 02A: Rep. Matt Grossell 93 District 09B: Rep. Ron Kresha 92 District 02B: Rep. Steve Green 92 District 04B: Rep. Paul Marquart 87 District 17A: Rep. Tim Miller 80 District 08A: Rep. Jordan Rasmusson 73 District 13A: Rep. Lisa Demuth 54 District 17B: Rep. Dave Baker 52 District 16A: Rep. Chris Swedzinski 48 District 16B: Rep. Paul Torkelson 43 District 05A: Rep. Matt Bliss 42 District 13B: Rep. Tim O'Driscoll 39 District 14A: Rep. Tama Theis 38 District 15B: Rep. Shane Mekeland 37 District 21A: Rep. Barb Haley 35 District 18A: Rep. Dean Urdahl 33 District 18B: Rep. Glenn Gruenhagen 28 District 29A: Rep. Joe McDonald 24 District 30B: Rep. Eric Lucero 23 District 14B: Rep. Dan Wolgamott 22 District 29B: Rep. Marion O'Neill 22 District 22B: Rep. Rod Hamilton 21 District 21B: Rep. Steve Drazkowski 20 District 15A: Rep. Sondra Erickson 19 District 31A: Rep. Kurt Daudt 18 District 11B: Rep. Nathan Nelson 17 District 06A: Rep. Julie Sandstede 16 District 23B: Rep. Jeremy Munson 15 District 30A: Rep. Paul Novotny 15 District 05B: Rep. Spencer Igo 15 District 32A: Rep. Brian Johnson 14 District 47A: Rep. Jim Nash 14 District 22A: Rep. Joe Schomacker 14 System Office Research, Academic and Student Affairs Division 11/19/2020 Alexandria Technical and Community College Credit Student Enrollment by House District Fiscal Year 2018-2019 Representative and District Enrollment District 10B: Rep. -

Journal of the House [60Th Day
60TH DAY] TUESDAY, FEBRUARY 11, 2020 6081 STATE OF MINNESOTA NINETY-FIRST SESSION - 2020 _____________________ SIXTIETH DAY SAINT PAUL, MINNESOTA, TUESDAY, FEBRUARY 11, 2020 The House of Representatives convened at 12:00 noon and was called to order by Melissa Hortman, Speaker of the House. Prayer was offered by the Reverend Richard D. Buller, Valley Community Presbyterian Church, Golden Valley, Minnesota. The members of the House gave the pledge of allegiance to the flag of the United States of America. The Speaker administered the oath of office to the new House member, Paul Novotny, from District 30A. His certificate of election is on file. He was elected in a special election held on Tuesday, February 4, 2020 to replace Nick Zerwas whose resignation was effective on Friday, December 6, 2019. The Speaker administered the oath of office to the new House member, Sydney Jordan, from District 60A. Her certificate of election is on file. She was elected in a special election held on Tuesday, February 4, 2020 to replace Diane Loeffler, who passed away on Saturday, November 16, 2019. The roll was called and the following members were present: Acomb Dehn Hausman Lillie Nornes Stephenson Albright Demuth Heinrich Lippert Novotny Sundin Anderson Dettmer Heintzeman Lislegard O'Driscoll Swedzinski Backer Drazkowski Her Long Olson Tabke Bahner Ecklund Hertaus Lucero O'Neill Theis Bahr Edelson Hornstein Lueck Pelowski Torkelson Baker Elkins Howard Mahoney Persell Urdahl Becker-Finn Erickson Huot Mann Petersburg Vang Bennett Fabian Johnson Mariani Pierson Vogel Bernardy Fischer Jordan Marquart Pinto Wagenius Bierman Franson Jurgens Masin Poppe Wazlawik Boe Freiberg Kiel McDonald Poston West Brand Garofalo Klevorn Mekeland Pryor Winkler Cantrell Gomez Koegel Miller Quam Wolgamott Carlson, A.