Trapezius Transfers for Irreparable Rotator Cuff Tears
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
The Structure and Function of Breathing
CHAPTERCONTENTS The structure-function continuum 1 Multiple Influences: biomechanical, biochemical and psychological 1 The structure and Homeostasis and heterostasis 2 OBJECTIVE AND METHODS 4 function of breathing NORMAL BREATHING 5 Respiratory benefits 5 Leon Chaitow The upper airway 5 Dinah Bradley Thenose 5 The oropharynx 13 The larynx 13 Pathological states affecting the airways 13 Normal posture and other structural THE STRUCTURE-FUNCTION considerations 14 Further structural considerations 15 CONTINUUM Kapandji's model 16 Nowhere in the body is the axiom of structure Structural features of breathing 16 governing function more apparent than in its Lung volumes and capacities 19 relation to respiration. This is also a region in Fascla and resplrstory function 20 which prolonged modifications of function - Thoracic spine and ribs 21 Discs 22 such as the inappropriate breathing pattern dis- Structural features of the ribs 22 played during hyperventilation - inevitably intercostal musculature 23 induce structural changes, for example involving Structural features of the sternum 23 Posterior thorax 23 accessory breathing muscles as well as the tho- Palpation landmarks 23 racic articulations. Ultimately, the self-perpetuat- NEURAL REGULATION OF BREATHING 24 ing cycle of functional change creating structural Chemical control of breathing 25 modification leading to reinforced dysfunctional Voluntary control of breathing 25 tendencies can become complete, from The autonomic nervous system 26 whichever direction dysfunction arrives, for Sympathetic division 27 Parasympathetic division 27 example: structural adaptations can prevent NANC system 28 normal breathing function, and abnormal breath- THE MUSCLES OF RESPIRATION 30 ing function ensures continued structural adap- Additional soft tissue influences and tational stresses leading to decompensation. -

Bilateral Sternalis Muscles Were Observed During Dissection of the Thoraco-Abdominal Region of a Male Cadaver
Case Reports Ahmed F. Ibrahim, MSc, MD, Saeed A. Makarem, MSc. PhD, Hassem H. Darwish, MBBCh. ABSTRACT Bilateral sternalis muscles were observed during dissection of the thoraco-abdominal region of a male cadaver. A full description of the muscles, as well as their attachments and innervations were reported. A brief review of the existing literature, regarding the nomenclature, incidence, attachments, innervations and clinical relevance of the sternalis muscle, is also presented. Neurosciences 2005; Vol. 10 (2): 171-173 he importance of continuing to record and Case Report. A well defined sternalis muscle Tdiscuss anatomical anomalies was addressed (Figures 1 & 2) was found, bilaterally, during recently1 in light of technical advances and dissection of the thoraco-abdominal region of a interventional methods of diagnosis and treatment. male cadaver in the Department of Anatomy, The sternalis muscle is a small supernumerary College of Medicine, King Saud University, Riyadh, muscle located in the anterior thoracic region, Kingdom of Saudi Arabia. Both muscles were superficial to the sternum and the sternocostal covered by superficial fascia, located superficial to fascicles of the pectoralis major muscle.2 In the the corresponding sternocostal portion of pectoralis literature, sternalis muscle is called "a normal major and separated from it by pectoral fascia. The anatomic variant"3 and "a well-known variation",4 left sternalis was 19 cm long and 3 cm wide at its although in most textbooks of anatomy, it is broadest part. Its upper end formed a tendon insufficiently mentioned. Yet, clinicians are continuous with that of the sternal head of left surprisingly unaware of this common variation. -

The Laminated Nature of the Pectoralis Major Muscle and the Redefinition of the Inframammary Fold Clinical Implications in Aesthetic and Reconstructive Breast Surgery
The Laminated Nature of the Pectoralis Major Muscle and the Redefinition of the Inframammary Fold Clinical Implications in Aesthetic and Reconstructive Breast Surgery Melvin M. Maclin II, MDa,*, Olivier A. Deigni, MD, MPHb, Bradley P. Bengtson, MDc KEYWORDS Pectoralis major muscle Inframammary fold Subpectoral augmentation Breast augmentation Breast reconstruction Acellular dermal matrix Breast inflection points Chest wall anatomy KEY POINTS The inframammary fold (IMF) is a critical landmark and aesthetic structure in breast surgery, yet it is poorly understood. The skin envelope is considered a separate entity from the chest wall; however, its surgical manip- ulation is not independent of chest wall anatomy. The pectoralis major muscle is a key structure in both cosmetic and reconstructive surgery, and its structure and performance are related to its inferior costal origins. A better understanding of the relationship of the IMF, pectoralis, and chest wall anatomy can offer improved outcomes in breast surgery. INTRODUCTION intimately aware of its relationship to the chest The breast is appreciated aesthetically and clini- wall and the breast soft tissues. Both are able to cally for its shape, projection, and volume. Multiple achieve outstanding outcomes; however, the au- techniques have evolved over the years to modify, thors present an alternative appreciation of the enhance, or recreate the breast mound. To this pectoralis and its relationship to the breast. The end surgical techniques have evolved to manipu- authors liken the comparison to the tale retold by late the breast skin envelope, soft tissues, and John Saxe of the 6 blind wise men and the chest wall anatomy, with and without prosthetic elephant (Fig. -

Pectoral Region and Axilla Doctors Notes Notes/Extra Explanation Editing File Objectives
Color Code Important Pectoral Region and Axilla Doctors Notes Notes/Extra explanation Editing File Objectives By the end of the lecture the students should be able to : Identify and describe the muscles of the pectoral region. I. Pectoralis major. II. Pectoralis minor. III. Subclavius. IV. Serratus anterior. Describe and demonstrate the boundaries and contents of the axilla. Describe the formation of the brachial plexus and its branches. The movements of the upper limb Note: differentiate between the different regions Flexion & extension of Flexion & extension of Flexion & extension of wrist = hand elbow = forearm shoulder = arm = humerus I. Pectoralis Major Origin 2 heads Clavicular head: From Medial ½ of the front of the clavicle. Sternocostal head: From; Sternum. Upper 6 costal cartilages. Aponeurosis of the external oblique muscle. Insertion Lateral lip of bicipital groove (humerus)* Costal cartilage (hyaline Nerve Supply Medial & lateral pectoral nerves. cartilage that connects the ribs to the sternum) Action Adduction and medial rotation of the arm. Recall what we took in foundation: Only the clavicular head helps in flexion of arm Muscles are attached to bones / (shoulder). ligaments / cartilage by 1) tendons * 3 muscles are attached at the bicipital groove: 2) aponeurosis Latissimus dorsi, pectoral major, teres major 3) raphe Extra Extra picture for understanding II. Pectoralis Minor Origin From 3rd ,4th, & 5th ribs close to their costal cartilages. Insertion Coracoid process (scapula)* 3 Nerve Supply Medial pectoral nerve. 4 Action 1. Depression of the shoulder. 5 2. Draw the ribs upward and outwards during deep inspiration. *Don’t confuse the coracoid process on the scapula with the coronoid process on the ulna Extra III. -
Muscles of Mastication Muscles That Move the Head
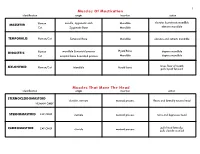
1 Muscles Of Mastication identification origin insertion action maxilla, zygomatic arch Mandible elevates & protracts mandible MASSETER Human Cat Zygomatic Bone Mandible elevates mandible TEMPORALIS Human/Cat Temporal Bone Mandible elevates and retracts mandible Hyoid Bone DIGASTRIC Human mandible & mastoid process depress mandible Cat occipital bone & mastoid process Mandible depress mandible raises floor of mouth; MYLOHYOID Human/Cat Mandible Hyoid bone pulls hyoid forward Muscles That Move The Head identification origin insertion action STERNOCLEIDOMAStoID clavicle, sternum mastoid process flexes and laterally rotates head HUMAN ONLY STERNOMAStoID CAT ONLY sternum mastoid process turns and depresses head pulls head laterally; CLEIDOMAStoID CAT ONLY clavicle mastoid process pulls clavicle craniad 2 Muscles Of The Hyoid, Larynx And Tongue identification origin insertion action Human Sternum Hyoid depresses hyoid bone STERNOHYOID Cat costal cartilage 1st rib Hyoid pulls hyoid caudally; raises ribs and sternum sternum Throid cartilage of larynx Human depresses thyroid cartilage STERNothYROID Cat costal cartilage 1st rib Throid cartilage of larynx pulls larynx caudad elevates thyroid cartilage and Human thyroid cartilage of larynx Hyoid THYROHYOID depresses hyoid bone Cat thyroid cartilage of larynx Hyoid raises larynx GENIOHYOID Human/Cat Mandible Hyoid pulls hyoid craniad 3 Muscles That Attach Pectoral Appendages To Vertebral Column identification origin insertion action Human Occipital bone; Thoracic and Cervical raises clavicle; adducts, -

Congenital Absence of the Pectoral Muscles
Arch Dis Child: first published as 10.1136/adc.12.68.123 on 1 April 1937. Downloaded from CONGENITAL ABSENCE OF THE PECTORAL MUSCLES BY E. D. IRVINE, M.D., AND J. B. TILLEY, M.D. (Blackburn). The four patients described in this paper exhibit congenital absence of the pectoral muscles in varying degree, and illustrate many points of interest. Three of them were observed during routine and special medical examinations of approximately 15,000 elementary school children, and one was a pre-school child in hospital: it is interesting to note that Scheslinger, according to Rector', discovered five cases in 54,000 patients. Case 1 was discovered during the examination of a boy aged ten, the second of four children, who complained of cough: he is under observation http://adc.bmj.com/ on September 30, 2021 by guest. Protected copyright. FIG. 1. as a tuberculosis contact. The sterno-costal portion of the left pectoralis major and the left pectoralis minor are both missing. Although not previously noted, this is believed to be a congenital defect. The clavicular head of the pectoralis major is well developed and arises from the inner half of the clavicle; the deltoid is not hypertrophied (fig. 1). When the arms are extended above the head, a well-marked fold of skin running vertically across the axilla to the second left rib and interspace can be seen and in Arch Dis Child: first published as 10.1136/adc.12.68.123 on 1 April 1937. Downloaded from I 2d4 AIICIlIVES 0O' DISEASE IN CHILDHOOD the fold fibrous tissue can be felt deep to the skin: whether this is simply fascia or a vestigial or degenerated muscle is not known. -

The Expiratory Muscles in Tetraplegia
Paraplegia 29 (1991) 359-363 © 1991 International Medical Society of Paraplegia Paraplegia J Review Article: The Expiratory Muscles in Tetraplegia A. De Troyer, MD, M. Estenne, MD Respiratory Research Unit and Chest Service, Erasme University Hospital, Brussels School of Medicine, Brussels, Belgium. All the well-recognised muscles of expiration, such as the muscles of the anterolate ral wall of the abdomen, the expiratory intercostals, and the triangularis sterni, have a motor innervation that depends on segments situated in the thoracic or lum bar cord.I-3 Consequently, subjects with tetraplegia caused by transection of the cervical cord have severely compromised expiratory muscle function. Cough in these subjects is markedly impaired, and the clearance of bronchial secretions is defective. As a result, retention of secretions leading to atelectasis and bronchopul monary infections is a frequent occurrence. Expiratory muscle function, in fact, has traditionally been perceived as being totally lost in tetraplegia. Hence, cough would be a passive process resulting only from the elastic recoil properties of the respiratory system.4 Expiratory muscle function is totally lost indeed in subjects with transection of the upper cervical cord (CI-C4). However, a number of spirographic studies have established that most C5-C8 tetraplegic subjects generate a small expiratory reserve volume.5-1O Thus, although all the well-known muscles of expiration are paralysed, most tetraplegic subjects are still able to activate some muscles that can overcome the elastic resist ance to deflation of the chest wall and cause emptying of the lungs. If these muscles could be identified, one could train them for .strength and perhaps· improve the effectiveness of cough so as to reduce the number of bronchopulmonary infections. -

Sonographic Tracking of Trunk Nerves: Essential for Ultrasound-Guided Pain Management and Research
Journal name: Journal of Pain Research Article Designation: Perspectives Year: 2017 Volume: 10 Journal of Pain Research Dovepress Running head verso: Chang et al Running head recto: Sonographic tracking of trunk nerve open access to scientific and medical research DOI: http://dx.doi.org/10.2147/JPR.S123828 Open Access Full Text Article PERSPECTIVES Sonographic tracking of trunk nerves: essential for ultrasound-guided pain management and research Ke-Vin Chang1,2 Abstract: Delineation of architecture of peripheral nerves can be successfully achieved by Chih-Peng Lin2,3 high-resolution ultrasound (US), which is essential for US-guided pain management. There Chia-Shiang Lin4,5 are numerous musculoskeletal pain syndromes involving the trunk nerves necessitating US for Wei-Ting Wu1 evaluation and guided interventions. The most common peripheral nerve disorders at the trunk Manoj K Karmakar6 region include thoracic outlet syndrome (brachial plexus), scapular winging (long thoracic nerve), interscapular pain (dorsal scapular nerve), and lumbar facet joint syndrome (medial branches Levent Özçakar7 of spinal nerves). Until now, there is no single article systematically summarizing the anatomy, 1 Department of Physical Medicine sonographic pictures, and video demonstration of scanning techniques regarding trunk nerves. and Rehabilitation, National Taiwan University Hospital, Bei-Hu Branch, In this review, the authors have incorporated serial figures of transducer placement, US images, Taipei, Taiwan; 2National Taiwan and videos for scanning the nerves in the trunk region and hope this paper helps physicians University College of Medicine, familiarize themselves with nerve sonoanatomy and further apply this technique for US-guided Taipei, Taiwan; 3Department of Anesthesiology, National Taiwan pain medicine and research. -

A Detailed Review on the Clinical Anatomy of the Pectoralis Major Muscle
SMGr up Review Article SM Journal of A Detailed Review on the Clinical Clinical Anatomy Anatomy of the Pectoralis Major Muscle Alexey Larionov, Peter Yotovski and Luis Filgueira* University of Fribourg, Faculty of Science and Medicine, Switzerland Article Information Abstract Received date: Aug 25, 2018 The pectoralis major is a muscle of the upper limb girdle. This muscle has a unique morphological Accepted date: Sep 07, 2018 architectonic and a high rate of clinical applications. However, there is lack of data regarding the morphological and functional interactions of the pectoralis major with other muscle and fascial compartments. According to the Published date: Sep 12, 2018 applied knowledge, the “Humero-pectoral” morpho-functional concept has been postulated. The purpose of this review was the dissectible investigation of the muscle anatomy and literature review of surgical applications. *Corresponding author Luis Filgueira, University of Fribourg, General Anatomy Faculty of Science and Medicine,1 Albert Gockel, CH-1700 Fribourg, Switzerland, The pectoralis major is a large, flat muscle of the pectoral girdle of the upper limb. It has a fan- Tel: +41 26 300 8441; shaped appearance with three heads or portions: the clavicular, the sternocostal and the abdominal Email: [email protected] head. Distributed under Creative Commons The clavicular head originates from the medial two-thirds of the clavicle (collar bone). The muscle fibers of the clavicular head have a broad origin on the caudal-anterior and caudal-posterior surface CC-BY 4.0 of the clavicle covering approximately half to two-thirds of that surface and converting toward the humerus, resulting in a triangular shape [1]. -

The Pectoral-Sternalis Complex: an Unusual Case Report
Case Report http://dx.doi.org/10.4322/jms.64113 The pectoral-sternalis complex: an unusual case report BALA, M.1*, PASSI, D. K.2 and KAUSHAL, S.3 1Medical college Mullana, Ambala. Haryana. India (Anatomy), Ambala – Índia 2Civil Hospital, Samana, Patiala (Civil Hospital, Samana, Patiala), 147101 Patiala – Índia 3Govt. Medical College, Patiala (Govt. Medical College, Patiala), 147001 Patiala – Índia *e-mail: [email protected] Abstract A unilateral absence of sternocostal fibers of pectoralis major muscle with unilateral presence of sternalis muscle has been noticed in right side of an adult male cadaver during routine dissection. All slips of pectoralis major muscle as well sternalis muscle innervated by medial and lateral pectoral nerves. Absence of pectoralis major has been described extensively, both as an isolated anomaly, with varying levels of hypoplasia, and in association with congenital syndromes. But the partial hypoplasia of pectoralis muscle with compensatory presence of one of the rare muscle of anterior thoracic wall the sternalis muscle make this case as unique and rare. This finding adds to our existing knowledge for the origin of sternalis, an identity not explored fully yet. Awareness of anomalous pectoralis major musculature as well presence of sternalis muscle is important for reconstructive surgeons who perform mastectomy and for radiologists during interpretation of skiagrams. Keywords: pectoralis major muscle, sternalis muscle, innervation. 1 Introduction The pectoralis major muscle is a thick triangular fan RATH, SHARMA et al., 2003). We report here an example shaped muscle of anterior chest wall. The clavicular head of appearance of the sternalis muscle with accompanying arises from the medial half of the anterior surface of the pectoralis major muscle anomaly. -

The Clavicular Part of the Pectoralis Major: a True Entity of the Upper Limb on Anatomical, Phylogenetic, Ontogenetic, Functional and Clinical Bases
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Firenze University Press: E-Journals IJAE Vol. 119, n. 1: 49-59, 2014 ITALIAN JOURNAL OF ANATOMY AND EMBRYOLOGY Research Article: Human Anatomy Case Report The clavicular part of the pectoralis major: a true entity of the upper limb on anatomical, phylogenetic, ontogenetic, functional and clinical bases. Case report and review of the literature Fabrizio Barberini Department of Anatomical, Histological, Forensic and Locomotor Apparatus Sciences, Section of Human Anatomy, University of Rome “La Sapienza”, Rome, Italy Submitted February 28, 2013; accepted revised July 12, 2013 Abstract The pectoralis major consists of three parts: clavicular, sternocostal and abdominal. The first is usually separated from the deltoid by a deltopectoral triangular space, and often from the ster- nocostal part by another triangular space. The clavicular part is a new acquisition in Anthro- poids, to optimize stabilization of the upper limb to the thorax thus permitting an increased limb mobility in Primates. It is synergetic with the deltoid in arm flexion and even more in adduc- tion. This action is important in Humans, as the coracobrachialis becomes smaller in Mammals. Among non human Primates, those having cranially displaced shoulder joint show a significant clavicular origin of the pectoralis major. The clavicular origin might be necessary in flexion of the forelimb, when the humeral insertion of the muscle is on the same transverse plane as, or cranial to, the sternal manubrium. As to the blood and nerve supply, occurrence in Humans of a neuro-vascular pedicle for the clavicular part, shared with the deltoid, indicates a relatively morpho-functional independence of this part from the rest of the muscle. -

A New Technique for Repairing Pectoralis Major Muscle Injuries with Cortical Button Fixation
TECHNIQUE A New Technique for Repairing Pectoralis Major Muscle Injuries With Cortical Button Fixation Erik A. Schnaser, MD,* Curtis Noel, MD,* and Reuben Gobezie, MDw unless a fragment of bone is avulsed with the tendon, and an Abstract: Several techniques have been described for the treatment magnetic resonance imaging verifies a complete rupture and of pectoralis major tendon injuries. Surgical intervention has shown to insures that there is enough pectoralis tendon to repair. yield superior clinical results in complete injuries. Without fixation, the After appropriate preoperative planning, the patient patient may have poor functional and cosmetic results. We describe receives an interscalene regional block before general here a new technique for repairing complete ruptures of the pectoralis anesthesia. The beach-chair position is used with the operative major tendon back to its insertion onto the humerus. To date, we have arm placed in either an arm positioner or on a padded Mayo had promising results with this technique and believe it may have stand. Perioperative antibiotics are administered before skin superior biomechanical properties over other methods of fixation. incision, and the skin is prepped and draped in standard sterile fashion. An Ioband (3M, St Paul, MN) is then used to seal the Key Words: pectoralis major rupture, cortical button, unicortical, drapes and axilla. The inferior aspect of the deltopectoral humerus approach is used, making a small incision in the upper medial (Tech Should Surg 2010;11: 81--84) humerus near the axillary fold. Sharp dissection is completed through the subcutaneous fat layer and hemostasis achieved with electrocautery. Care is taken when entering the fascial layer and once through the fascia, blunt finger dissection medially toward the pectoralis muscle belly will reveal the ectoralis major muscle injuries are relatively rare injuries retracted pectoralis tendon.