Genetic Disorders Associated with Gingival Enlargement
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
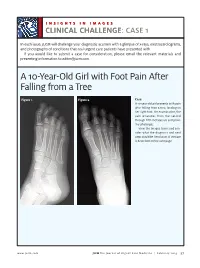
A 10-Year-Old Girl with Foot Pain After Falling from a Tree
INSIGHTS IN IMAGES CLINICAL CHALLENGECHALLENGE: CASE 1 In each issue, JUCM will challenge your diagnostic acumen with a glimpse of x-rays, electrocardiograms, and photographs of conditions that real urgent care patients have presented with. If you would like to submit a case for consideration, please email the relevant materials and presenting information to [email protected]. A 10-Year-Old Girl with Foot Pain After Falling from a Tree Figure 1. Figure 2. Case A 10-year-old girl presents with pain after falling from a tree, landing on her right foot. On examination, the pain emanates from the second through fifth metatarsals and proxi- mal phalanges. View the images taken and con- sider what the diagnosis and next steps would be. Resolution of the case is described on the next page. www.jucm.com JUCM The Journal of Urgent Care Medicine | February 2019 37 INSIGHTS IN IMAGES: CLINICAL CHALLENGE THE RESOLUTION Figure 1. Mediastinal air Figure 1. Differential Diagnosis Pearls for Urgent Care Management and Ⅲ Fracture of the distal fourth metatarsal Considerations for Transfer Ⅲ Plantar plate disruption Ⅲ Emergent transfer should be considered with associated neu- Ⅲ Sesamoiditis rologic deficit, compartment syndrome, open fracture, or vas- Ⅲ Turf toe cular compromise Ⅲ Referral to an orthopedist is warranted in the case of an in- Diagnosis tra-articular fracture, or with Lisfranc ligament injury or ten- Angulation of the distal fourth metatarsal metaphyseal cortex derness over the Lisfranc ligament and hairline lucency consistent with fracture. Acknowledgment: Images courtesy of Teleradiology Associates. Learnings/What to Look for Ⅲ Proximal metatarsal fractures are most often caused by crush- ing or direct blows Ⅲ In athletes, an axial load placed on a plantar-flexed foot should raise suspicion of a Lisfranc injury 38 JUCM The Journal of Urgent Care Medicine | February 2019 www.jucm.com INSIGHTS IN IMAGES CLINICAL CHALLENGE: CASE 2 A 55-Year-Old Man with 3 Hours of Epigastric Pain 55 years PR 249 QRSD 90 QT 471 QTc 425 AXES P 64 QRS -35 T 30 Figure 1. -

Glossary for Narrative Writing
Periodontal Assessment and Treatment Planning Gingival description Color: o pink o erythematous o cyanotic o racial pigmentation o metallic pigmentation o uniformity Contour: o recession o clefts o enlarged papillae o cratered papillae o blunted papillae o highly rolled o bulbous o knife-edged o scalloped o stippled Consistency: o firm o edematous o hyperplastic o fibrotic Band of gingiva: o amount o quality o location o treatability Bleeding tendency: o sulcus base, lining o gingival margins Suppuration Sinus tract formation Pocket depths Pseudopockets Frena Pain Other pathology Dental Description Defective restorations: o overhangs o open contacts o poor contours Fractured cusps 1 ww.links2success.biz [email protected] 914-303-6464 Caries Deposits: o Type . plaque . calculus . stain . matera alba o Location . supragingival . subgingival o Severity . mild . moderate . severe Wear facets Percussion sensitivity Tooth vitality Attrition, erosion, abrasion Occlusal plane level Occlusion findings Furcations Mobility Fremitus Radiographic findings Film dates Crown:root ratio Amount of bone loss o horizontal; vertical o localized; generalized Root length and shape Overhangs Bulbous crowns Fenestrations Dehiscences Tooth resorption Retained root tips Impacted teeth Root proximities Tilted teeth Radiolucencies/opacities Etiologic factors Local: o plaque o calculus o overhangs 2 ww.links2success.biz [email protected] 914-303-6464 o orthodontic apparatus o open margins o open contacts o improper -

Keratocystic Odontogenic Tumour Mimicking As a Dentigerous Cyst – a Rare Case Report Dr
DOI: 10.21276/sjds.2017.4.3.16 Scholars Journal of Dental Sciences (SJDS) ISSN 2394-496X (Online) Sch. J. Dent. Sci., 2017; 4(3):154-157 ISSN 2394-4951 (Print) ©Scholars Academic and Scientific Publisher (An International Publisher for Academic and Scientific Resources) www.saspublisher.com Case Report Keratocystic Odontogenic Tumour Mimicking as a Dentigerous Cyst – A Rare Case Report Dr. K. Saraswathi Gopal1, Dr. B. Prakash vijayan2 1Professor and Head, Department of Oral Medicine and Radiology, Meenakshi Ammal Dental College and Hospital, Chennai 2PG Student, Department of Oral Medicine and Radiology, Meenakshi Ammal Dental College and Hospital, Chennai *Corresponding author Dr. B. Prakash vijayan Email: [email protected] Abstract: Keratocystic odontogenic tumor (KCOT) formerly known as odontogenic keratocyst (OKC), is considered a benign unicystic or multicystic intraosseous neoplasm and one of the most aggressive odontogenic lesions presenting relatively high recurrence rate and a tendency to invade adjacent tissue. On the other hand Dentigerous cyst (DC) is one of the most common odontogenic cysts of the jaws and rarely recurs. They were very similar in clinical and radiographic characteristics. In our case a pathological report following incisional biopsy turned out to be dentigerous cyst and later as Keratocystic odontogenic tumour following total excision. The treatment was chosen in order to prevent any pathological fracture. A recurrence was noticed after 2 months following which the lesion was surgically enucleated. At 2-years of follow-up, patient showed no recurrence. Keywords: Dentigerous cyst, Keratocystic odontogenic tumour (KCOT), Recurrence, Enucleation INTRODUCTION Keratocystic odontogenic tumour (KCOT) is a CASE REPORT rare developmental, epithelial and benign cyst of the A 17-year-old patient reported to the OP with a jaws of odontogenic origin with high recurrence rates. -

59. Lateral Facial Clefts
59 LATERAL FACIAL CLEFTS LI OR TRANSVERSE CLEFTS ARE CONSIDERED THE RESULT OF FAILURE OF MESODERM MIGRATION OR MERGING TO OBLITERATE MANDIBULAR THE EMBRYONIC GROOVES BETWEEN THE MAXILLARY AND PROMINENCES TRANSVERSE CLEFTS AS THESE CLEFTS ARE RARE AND ALMOST EVERYBODY HAVING ONE HAS AND REPORTED IT IT IS POSSIBLE TO REVIEW MOST OF THE REPORTED CASES 769 DESCRIBED THE AFTER WHEN NOTE TREATMENT SPECIFIC CASE RECORDINGS IN WHAT MAY SEEM HELTERSKELTER ARRANGEMENT GENERALIZATIONS MAY BE OF VALUE IN 1891 ROSE NOTED FOR LONG THE VERY EXISTENCE OF THIS MACROSROMATOUS DEFORMITY WAS DOUBTED BUT CASES HAVE BEEN RECOGNIZED MORE OR LESS SINCE 1715 WHEN MURALT PICTURED IT FOR THE FIRST TIME ONE OF THE FIRST CASES REPORTED WAS BY VROLIK WHOIN HIS 1849 CLEFTS WORK GAVE SEVERAL ILLUSTRATIONS OF COMMISSURAL AS WELL AS OTHER DEFORMITIES OF THE FACE OTHER CASES WERE REPORTED BY REISSMANN IN 1869 AND MORGAN IN 1882 MACROSTOMIA OR COMMISSURAL HARELIP ACCORDING TO ROSE IS DIAMETER OF WHICH EVIDENCED BY AN INCREASED THE MOUTH MAY VARY IN FROM SLIGHT INCREASE TO CONSIDERABLE DISTANCE CASE RE PORTED BY RYND IN 1862 THE MOUTH OPENING EXTENDED AS FAR AS THE THE LEFT FIRST MOLAR ON THE RIGHT SIDE AND TO THE LAST MOLAR ON IN 1887 SUTTON PUBLISHED THE DRAWING OF CHILD WITH VERY LARGE RED CICATRIX THIS CLEFT THE ANGLES OF WHICH GRADUALLY PASSED INTO SCAR ENDED IN GAPING WOUND OVER THE TEMPORAL REGION EXTEND ING TO THE DURA MATER ROSE ALSO POINTED OUT MACROSROMA IS NOR ONLY ATTENDED BY GREAT DISFIGUREMENT HUT IS ALSO TROU BLESOME FROM THE IMPOSSIBILITY OF THE CHILD RETAINING -

OCSHCN-10G, Medical Eligibility List for Clinical and Case Management Services.Pdf
OCSHCN-10g (01 2019) (Rev 7-15-2017) Office for Children with Special Health Care Needs Medical Eligibility List for Clinical and Case Management Services BODY SYSTEM ELIGIBLE DISEASES/CONDITIONS ICD-10-CM CODES AFFECTED AUTISM SPECTRUM Autistic disorder, current or active state F84.0 Autistic disorder DISORDER (ASD) F84.3 Other childhood disintegrative disorder Autistic disorder, residual state F84.5 Asperger’s Syndrome F84.8 Other pervasive developmental disorder Other specified pervasive developmental disorders, current or active state Other specified pervasive developmental disorders, residual state Unspecified pervasive development disorder, current or active Unspecified pervasive development disorder, residual state CARDIOVASCULAR Cardiac Dysrhythmias I47.0 Ventricular/Arrhythmia SYSTEM I47.1 Supraventricular/Tachycardia I47.2 Ventricular/Tachycardia I47.9 Paroxysmal/Tachycardia I48.0 Paroxysmal atrial fibrillation I48.1 Persistent atrial fibrillationar I48.2 Chronic atrial fibrillation I48.3 Typical atrial flutter I48.4 Atypical atrial flutter I49.0 Ventricular fibrillation and flutter I49.1 Atrial premature depolarization I49.2 Junctional premature depolarization I49.3 Ventricular premature depolarization I49.49 Ectopic beats Extrasystoles Extrasystolic arrhythmias Premature contractions Page 1 of 28 OCSHCN-10g (01 2019) (Rev 7-15-2017) Office for Children with Special Health Care Needs Medical Eligibility List for Clinical and Case Management Services I49.5 Tachycardia-Bradycardia Syndrome CARDIOVASCULAR Chronic pericarditis -

Genetic Mechanisms of Disease in Children: a New Look
Genetic Mechanisms of Disease in Children: A New Look Laurie Demmer, MD Tufts Medical Center and the Floating Hospital for Children Boston, MA Traditionally genetic disorders have been linked to the ‘one gene-one protein-one disease’ hypothesis. However recent advances in the field of molecular biology and biotechnology have afforded us the opportunity to greatly expand our knowledge of genetics, and we now know that the mechanisms of inherited disorders are often significantly more complex, and consequently, much more intriguing, than originally thought. Classical mendelian disorders with relatively simple genetic mechanisms do exist, but turn out to be far more rare than originally thought. All patients with sickle cell disease for example, carry the same A-to-T point mutation in the sixth codon of the beta globin gene. This results in a glutamate to valine substitution which changes the shape and the function of the globin molecule in a predictable way. Similarly, all patients with achondroplasia have a single base pair substitution at nucleotide #1138 of the FGFR3 gene. On the other hand, another common inherited disorder, cystic fibrosis, is known to result from changes in a specific transmembrane receptor (CFTR), but over 1000 different disease-causing mutations have been reported in this single gene. Since most commercial labs only test for between 23-100 different mutations, interpreting CFTR mutation testing is significantly complicated by the known risk of false negative results. Many examples of complex, or non-Mendelian, inheritance are now known to exist and include disorders of trinucleotide repeats, errors in imprinting, and gene dosage effects. -

Segmental Overvekst Og Vaskulærmalformasjoner V02
2/1/2021 Segmental overvekst og vaskulærmalformasjoner v02 Avdeling for medisinsk genetikk Segmental overvekst og vaskulærmalformasjoner Genpanel, versjon v02 * Enkelte genomiske regioner har lav eller ingen sekvensdekning ved eksomsekvensering. Dette skyldes at de har stor likhet med andre områder i genomet, slik at spesifikk gjenkjennelse av disse områdene og påvisning av varianter i disse områdene, blir vanskelig og upålitelig. Disse genetiske regionene har vi identifisert ved å benytte USCS segmental duplication hvor områder større enn 1 kb og ≥90% likhet med andre regioner i genomet, gjenkjennes (https://genome.ucsc.edu). Vi gjør oppmerksom på at ved identifiseringav ekson oppstrøms for startkodon kan eksonnummereringen endres uten at transkript ID endres. Avdelingens websider har en full oversikt over områder som er affisert av segmentale duplikasjoner. ** Transkriptets kodende ekson. Ekson Gen Gen affisert (HGNC (HGNC Transkript Ekson** Fenotype av symbol) ID) segdup* ACVRL1 175 NM_000020.3 2-10 Telangiectasia, hereditary hemorrhagic, type 2 OMIM ADAMTS3 219 NM_014243.3 1-22 Hennekam lymphangiectasia- lymphedema syndrome 3 OMIM AKT1 391 NM_005163.2 2-14 Cowden syndrome 6 OMIM Proteus syndrome, somatic OMIM AKT2 392 NM_001626.6 2-14 Diabetes mellitus, type II OMIM Hypoinsulinemic hypoglycemia with hemihypertrophy OMIM AKT3 393 NM_005465.7 2-14 Megalencephaly-polymicrogyria- polydactyly-hydrocephalus syndrome 2 OMIM file:///data/SegOv_v02-web.html 1/7 2/1/2021 Segmental overvekst og vaskulærmalformasjoner v02 Ekson Gen Gen affisert (HGNC (HGNC -

PTEN Mutations the PTEN Hamartoma Tumor Synd
Updated December 2019 (NCCN v1.2020) Cowden Syndrome/PTEN Hamartoma Tumor Syndrome: PTEN Mutations The PTEN Hamartoma Tumor Syndrome (PHTS) is a spectrum of highly variable conditions with overlapping features. This spectrum includes Cowden syndrome (CS), Bannayan-Riley-Ruvalcaba syndrome (BRRS), and PTEN-related autism spectrum disorder.1-3 The term PHTS describes any individual with a germline pathogenic PTEN mutation, regardless of their clinical presentation.4 PHTS is a multisystem syndrome primarily characterized by noncancerous (benign), tumor-like growths called hamartomas that can develop throughout the body. There is also an increased risk of adult-onset cancers.5 Cancer Risks and General Management Recommendations PTEN Mutation General Surveillance/Management Recommendations9 Carrier Cancer Population Risks2,4-8 Lifetime Cancer Risks Female Breast: 12.4% Surveillance Primary: 33-60% Breast awareness, including periodic, consistent breast self exams, Second Primary: starting at age 18 years 29% within 10 Clinical breast exam every 6-12 months starting at age 25 years, or 5- years10 10 years before the earliest breast cancer diagnosis in the family (whichever comes first) Annual mammogram with consideration of tomosynthesis and breast MRI with contrast at age 30-35 years, or 5-10 years before the earliest breast cancer diagnosis in the family (whichever comes first) Age >75 years: Management should be considered on an individual basis Surgery Discuss option of risk-reducing mastectomy, including degree of protection, reconstruction -

Review: Differential Diagnosis of Drug-Induced Gingival Hyperplasia and Other Oral Lesions
ISSN: 2469-5734 Moshe. Int J Oral Dent Health 2020, 6:108 DOI: 10.23937/2469-5734/1510108 Volume 6 | Issue 2 International Journal of Open Access Oral and Dental Health REVIEW ARTICLE Review: Differential Diagnosis of Drug-Induced Gingival Hyper- plasia and Other Oral Lesions Einhorn Omer Moshe* Private Dental Office, Israel Check for *Corresponding author: Einhorn Omer Moshe, Private Dental Office, Dr. Einhorn, 89 Medinat Hayehudim updates street, Herzliya, Israel tooth discoloration, alteration of taste sensation and Abstract even appearance of lesions on the tissues of the oral Chronic medication usage is a major component of the cavity. Early recognition and diagnosis of these effects medical diagnosis of patients. Nowadays, some of the most common diseases such as cancer, hypertension, diabetes can largely assist in the prevention of further destruc- and etc., are treated with drugs which cause a variety of oral tive consequences in patients’ health status. As life ex- side-effects including gingival over growth and appearance pectancy increases, the number of elderly patients in of lesions on the tissues of the oral cavity. As such, drug-in- the dental practice also rises. Individuals of this popula- duced oral reactions are an ordinary sight in the dental prac- tice. This review will point out the main therapeutic agents tion are usually subjected to chronic medication intake causing gingival hyperplasia and other pathologic lesions which requires the clinician to be aware of the various in the oral cavity. Some frequently used medications, in side-effects accompanying these medications. This re- particular antihypertensives, nonsteroidal anti-inflammatory view will point out the main therapeutic agents causing drugs and even antibiotics, can lead to overgrowth of the gingival hyperplasia and other pathologic lesions in the gingiva and to the multiple unwanted conditions, namely: Lupus erythematosus, erythema multiforme, mucositis, oral oral cavity. -

Orofacial Manifestations of COVID-19: a Brief Review of the Published Literature
CRITICAL REVIEW Oral Pathology Orofacial manifestations of COVID-19: a brief review of the published literature Esam HALBOUB(a) Abstract: Coronavirus disease 2019 (COVID-19) has spread Sadeq Ali AL-MAWERI(b) exponentially across the world. The typical manifestations of Rawan Hejji ALANAZI(c) COVID-19 include fever, dry cough, headache and fatigue. However, Nashwan Mohammed QAID(d) atypical presentations of COVID-19 are being increasingly reported. Saleem ABDULRAB(e) Recently, a number of studies have recognized various mucocutaneous manifestations associated with COVID-19. This study sought to (a) Jazan University, College of Dentistry, summarize the available literature and provide an overview of the Department of Maxillofacial Surgery and potential orofacial manifestations of COVID-19. An online literature Diagnostic Sciences, Jazan, Saudi Arabia. search in the PubMed and Scopus databases was conducted to retrieve (b) AlFarabi College of Dentistry and Nursing, the relevant studies published up to July 2020. Original studies Department of Oral Medicine and published in English that reported orofacial manifestations in patients Diagnostic Sciences, Riyadh, Saudi Arabia. with laboratory-confirmed COVID-19 were included; this yielded 16 (c) AlFarabi College of Dentistry and Nursing, articles involving 25 COVID-19-positive patients. The results showed a Department of Oral Medicine and Diagnostic Sciences, Riyadh, Saudi Arabia. marked heterogeneity in COVID-19-associated orofacial manifestations. The most common orofacial manifestations were ulcerative lesions, (d) AlFarabi College of Dentistry and Nursing, Department of Restorative Dental Sciences, vesiculobullous/macular lesions, and acute sialadentitis of the parotid Riyadh, Saudi Arabia. gland (parotitis). In four cases, oral manifestations were the first signs of (e) Primary Health Care Corporation, Madinat COVID-19. -

Oral Manifestations of Systemic Disease Their Clinical Practice
ARTICLE Oral manifestations of systemic disease ©corbac40/iStock/Getty Plus Images S. R. Porter,1 V. Mercadente2 and S. Fedele3 provide a succinct review of oral mucosal and salivary gland disorders that may arise as a consequence of systemic disease. While the majority of disorders of the mouth are centred upon the focus of therapy; and/or 3) the dominant cause of a lessening of the direct action of plaque, the oral tissues can be subject to change affected person’s quality of life. The oral features that an oral healthcare or damage as a consequence of disease that predominantly affects provider may witness will often be dependent upon the nature of other body systems. Such oral manifestations of systemic disease their clinical practice. For example, specialists of paediatric dentistry can be highly variable in both frequency and presentation. As and orthodontics are likely to encounter the oral features of patients lifespan increases and medical care becomes ever more complex with congenital disease while those specialties allied to disease of and effective it is likely that the numbers of individuals with adulthood may see manifestations of infectious, immunologically- oral manifestations of systemic disease will continue to rise. mediated or malignant disease. The present article aims to provide This article provides a succinct review of oral manifestations a succinct review of the oral manifestations of systemic disease of of systemic disease. It focuses upon oral mucosal and salivary patients likely to attend oral medicine services. The review will focus gland disorders that may arise as a consequence of systemic upon disorders affecting the oral mucosa and salivary glands – as disease. -

Unusual Imaging Features of Dentigerous Cyst: a Case Report
dentistry journal Case Report Unusual Imaging Features of Dentigerous Cyst: A Case Report Carla Patrícia Martinelli-Kläy 1,2,*, Celso Ricardo Martinelli 2, Celso Martinelli 2, Henrique Roberto Macedo 2 and Tommaso Lombardi 1 1 Laboratory of Oral & Maxillofacial Pathology, Oral Medicine and Oral and Maxillofacial Pathology Unit, Division of Oral Maxillofacial Surgery, Department of Surgery, Geneva University Hospitals, University of Geneva, 1211 Geneva, Switzerland 2 Centre for Diagnosis and Treatment of Oral Diseases, Ribeirão Preto 14025-250, Brazil * Correspondence: [email protected]; Tel.: +41-22-379-4034 Received: 26 March 2019; Accepted: 5 July 2019; Published: 1 August 2019 Abstract: Dentigerous cysts (DC) are cystic lesions radiographically represented by a well-defined unilocular radiolucent area involving an impacted tooth crown. We present an unusual radiographic feature of dentigerous cyst related to the impacted mandibular right second molar, in a 16-year-old patient, which suggested an ameloblastoma or odontogenic keratocyst (OKC) because of its multilocular appearance seen on the panoramic radiography. A multi-slice computed tomography (MSCT), however, revealed a unilocular lesion without septations, with an attenuation coefficient from 3.9 to 22.9 HU suggesting a cystic lesion. Due to its extension, a marsupialization was performed together with the histopathological analysis of the fragment removed which suggested a dentigerous cyst. Nine months later, the lesion was reduced in size and then totally excised. The impacted mandibular right second molar was also extracted. Histopathological examination confirmed the diagnosis of a dentigerous cyst. One year later, the panoramic radiography showed a complete mandible bone healing. Large dentigerous cysts can sometimes suggest other more aggressive pathologies.